
Abstract
Background and Objectives:
Myocardial hypertrophy and fibrosis are important determinants of congestive heart failure. Previous work has shown that hepatocyte growth factor (HGF) can reduce acute myocardial injury and tissue fibrosis. This study was designed to examine the effects of HGF on myocardial remodeling following sustained hypertension.
Methods and Results:
There were 4 experimental groups (n = 6) that included spontaneously hypertensive rats (SHRs) injected with 0.1 mL of adenovirus (Ad)-null into the left ventricular (LV) free wall, SHR injected with 0.1 mL of Ad-HGF gene (5 × 109 pfu/mL), and SHR injected with 0.1 mL of normal saline, and Wistar Kyoto rats injected with 0.1 mL of Ad-null served as control. At 4 weeks after injection, rats were sacrificed, and HGF expression, myocardial fibrosis, and LV function were determined. We observed that HGF protein expression was reduced in the hearts of SHR (P < .05 vs normal control) and it was markedly increased in SHR injected with Ad-HGF (P < .01 vs SHR injected with Ad-null). Myocardial fibrosis, collagen I, LV mass index (LVMI), and LV end-diastolic pressure (LVEDP) were increased and −dP/dtmax was decreased in SHR injected with Ad-null or normal saline (P < .01 vs normal control). Upregulation of myocardial HGF expression in SHR significantly suppressed myocardial fibrosis, collagen I content, LVMI, LVEDP, and increased −dP/dtmax (all P < .05 vs SHR-Ad-null, n = 6).
Conclusions:
These findings indicate that HGF expression is attenuated in hypertrophic and fibrotic myocardium of SHR. The forced increase in HGF exerts a salutary effect on myocardial fibrosis, collagen I expression, and hemodynamic parameters.
Introduction
Hypertensive cardiomyopathy and associated complications, such as congestive heart failure, are a major health issue worldwide. The pathological features of hypertensive cardiomyopathy include increased myocardial oxygen consumption, 1 impaired epicardial coronary perfusion, 2 ventricular fibrosis and hypertrophy, 3 and abnormalities in long-axis function and torsion, 4 leading to systolic and diastolic functional abnormalities. Therapies aimed at reversing myocardial fibrosis and hypertrophy may improve exercise capacity and decrease mortality.
Hepatocyte growth factor (HGF) is a multifunctional growth factor. It attaches to its specific receptor c-Met on the cell membrane and results in phosphorylation of protein tyrosine kinase. 5 Studies in animal models of acute myocardial infarction have shown that an increase in HGF expression in the regional myocardium can reduce myocardial fibrosis, 6,7 inhibit apoptosis, 8,9 promote angiogenesis, 10,11 and improve myocardial function. 6,7,10 The HGF reduces the generation of extracellular matrix, 12 activates matrix metalloproteinase 1 (MMP-1), and increases matrix degradation. 13 However, the effects of HGF on myocardial remodeling in hypertensive cardiomyopathy is not clear.
In this study, we examined the role of HGF in myocardial fibrosis, collagen synthesis, and left ventricular mass index (LVMI) and ventricular hemodynamic changes in spontaneously hypertensive rats (SHR) using HGF gene delivery by adenovirus vector technology.
Materials and Methods
Experimental Animals and Groups
This study was approved by the ethics committee of the First Affiliated Hospital, Anhui Medical University, Hefei, China. All rats were bred with humane care in compliance with the “Principles of Laboratory Animal Care” formulated by the USA National Society for Medical Research and the Guide for the Care and Use of Laboratory Animals. The 14-week-old SHR weighing 260 ± 10 g (Beijing Weitong Lihua Laboratory Animal Technique Company, Beijing, China) served as the model of hypertensive cardiomyopathy. Animals were randomly divided into 3 groups, SHR injected with 0.1 mL of adenovirus-null (SHR-Ad group), SHR-Ad-HGF injected with 0.1 mL of 5 × 109 pfu/mL Ad with HGF gene (SHR-Ad-HGF group), and SHR-NS injected 0.1 mL of normal saline (SHR-NS group). Wistar Kyoto (WKY) rats were injected with null-Ad (control group).
Transfection of the Ad-HGF Gene
Each rat was anesthetized with 10% chloraldural and then intubated. After left thoracotomy, the heart was exposed, and then 0.1 mL of null-Ad, 0.1 mL of 5 × 109 pfu/mL Ad-HGF, or 0.1 mL of normal saline was directly injected into the left ventricular (LV) free wall at 5 different sites. The Ad-null and Ad-HGF gene were purchased from the Institute of Academy of Military Medical Radiology (Beijing, China). The chest was closed after injection. The procedure was performed under sterile conditions. Each rat was given penicillin 4 00 000 units daily for 3 days intramuscularly.
Hemodynamic Measurements
At 4 weeks after injection, the rats were anesthetized and intubated. A silicone tube was inserted into the right common carotid artery and advanced into the LV to measure the LV end-diastolic pressure (LVEDP) and the maximum descending rate of the LV pressure (–dP/dtmax) during 10 stable cardiac cycles using a high fidelity transducer (Chengdu Tai Meng Science and Technology Co Ltd, Chengdu, China).
Measurements of Myocardial HGF Content
A small piece of the LV free wall was homogenized in phosphate-buffered saline. After centrifugation, the supernatant was collected. Myocardial HGF content was measured using enzyme-linked immunosorbent assay (Yuan Ye Biotechnology Reagent Company, Shanghai, China) and expressed as ng/g of myocardial tissue.
Histological Analyses
After measurement of hemodynamics, the heart was excised quickly. The LV was harvested and washed thoroughly with saline and weighed after drying using a filter paper. The LVMI (left ventricle/body weight) was calculated. Afterward, the LV was cut in short axis, and a part of it was fixed in 10% formalin for 48 to 72 hours, dehydrated, embedded in paraffin, and cut into 5-μm thick slices.
Myocardial fibrosis was assessed using Masson-trichrome staining (Fuzhou Maixin Biotechnology Development Co, Ltd, Fuzhou, China), in which myocardial cells appear red and fibrotic myocardium appears blue. Six slices of LV tissue were obtained from each rat and evaluated by one of the authors in a blinded fashion. Five fields of each slide (magnification 200×) were randomly selected for assessment of myocardial fibrosis.
Collagen I was detected with immunohistochemical analysis (Sigma-Aldrich, Inc, Missouri). Area of collagen I-positive staining was calculated using Image-Pro Plus 6.0 image analysis software (Media Cybernetics, Inc. Bethesda, MD).
Western Blot Analysis of Collagen I
An aliquot of LV was cut into small pieces in radioimmunoprecipitation assay (RIPA) buffer and homogenized, followed by centrifugation. Western blotting was carried out by standard methodology. Collagen I monoclonal antibody was obtained from Sigma (Springfield, Missouri) and secondary antibody (1:5000 dilution) from Amersham (Glen Carbon, Illinois). The membranes were washed, and collagen I band was detected with the ECL system (Amersham) and compared with β-actin as an internal reference.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation, and the differences among the groups were assessed using 1-way analysis of variance, followed by Student Newman-Keuls test for multiple comparisons. All statistical tests were 2 tailed, and P < .05 was considered statistically significant.
Results
Hepatocyte Growth Factor Expression in the Heart
We observed that HGF expression in the LV sections from SHR was significantly lower (P < .05 vs WKY rats, n = 6). The HGF level in LV sections of SHR was markedly increased in rats given injection of Ad-HGF gene (vs rats injected with Ad-null or normal saline, P < .01, n = 6). The Ad-null or normal saline injection had no effect on HGF expression in the myocardium (Figure 1).
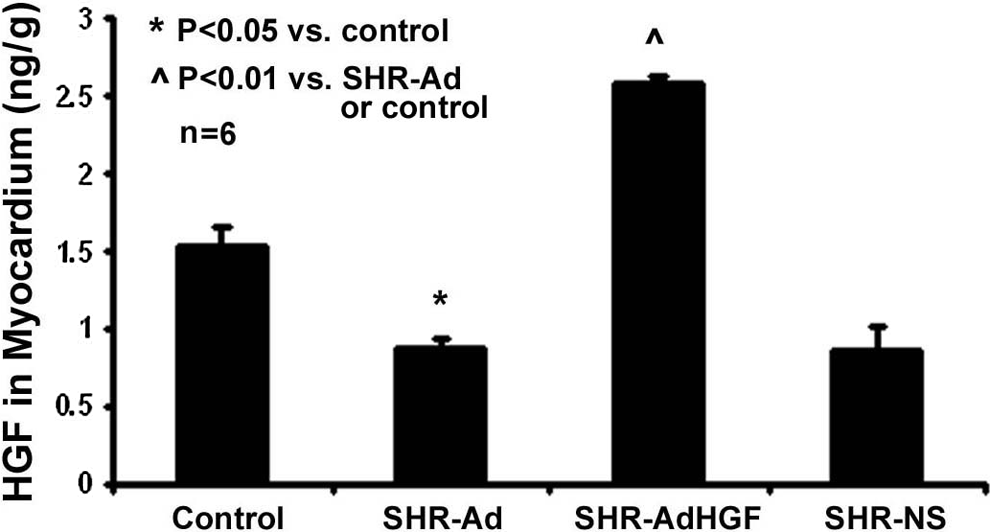
The HGF expression in myocardium. The HGF expression in the SHR-Ad group was reduced compared with that in the normal control. The HGF level in the SHR-Ad-HGF group was increased compared with that in the SHR-Ad group. The SHR-Ad or SHR-NS had no effect on HGF expression in the myocardium. HGF indicates hepatic growth factor; SHR, spontaneous hypertensive rats; Ad, adenovirus; NS, normal saline.
Effects of HGF on Myocardial Collagen I Synthesis
Collagen I expression (Western blotting) was markedly increased in the hearts of SHR injected with Ad-null or normal saline compared to that in the normal control rats (both P < .01, n = 6). Importantly, the injection of Ad-HGF significantly attenuated collagen I expression in SHR (vs injections of Ad-null or normal saline, both P < .01, n = 6 in each group). The results of collagen I staining (Figure 2) and Western blotting (Figure 3) were similar.

Effects of HGF on myocardial collagen I content. Myocardial immunostaining showed that collagen I in SHR-Ad or SHR-NS group was increased compared with that in the normal control. Importantly, increase in HGF in the SHR-Ad-HGF group significantly attenuated collagen I synthesis. The left panel shows representative collagen I staining areas. The right panel is the summary data based on average optical density (AOD). Ad indicates adenovirus; HGF, hepatic growth factor; NS, normal saline; SHR, spontaneous hypertensive rats.

The HGF and collagen I synthesis. Collagen I in SHR-Ad or SHR-NS group was increased compared with that in the normal control. Consistent with immunostaining data shown in Figure 2, increased HGF content in the SHR-Ad-HGF group attenuated collagen I synthesis. The top panel shows representative staining areas. The bottom panel is the summary data. Ad indicates adenovirus; HGF, hepatocyte growth factor; NS, normal saline; SHR, spontaneous hypertensive rats.
Effects of HGF on Myocardial Fibrosis
Image analysis showed that myocardial fibrosis as determined by optical density (OD) was markedly higher in SHR than in normal control rats (P < .01, n = 6). With the forced overexpression of HGF, myocardial fibrosis in the hearts of SHR indicated by OD was significantly reduced (vs injections of Ad-null or normal saline, both P < .01, n = 6 in each group; Figure 4).

Effects of HGF on myocardial fibrosis. Myocardial fibrosis determined by optical density in the SHR-Ad group was markedly increased compared with that in the normal control. Myocardial fibrosis was not affected by Ad-null or normal saline, but Ad-HGF significantly decreased fibrosis. The left panel shows representative areas of fibrosis staining. The right panel is the summarized data of fibrosis, which is expressed as fibrotic area–tissue area ratio. Ad indicates adenovirus; HGF, hepatocyte growth factor; SHR, spontaneous hypertensive rats.
Effects of HGF on LVMI and Hemodynamic Parameters
The LVMI in the SHR group was consistently increased compared with that in the normal control rats (both P < .01, n = 6). With the forced overexpression of HGF, LVMI in the hearts of SHR was significantly reduced (vs injection of Ad-null or normal saline, both P < .01, n = 6 in each group; Figure 4; Table 1).
Effects of HGF on LVMI and Hemodynamics.a
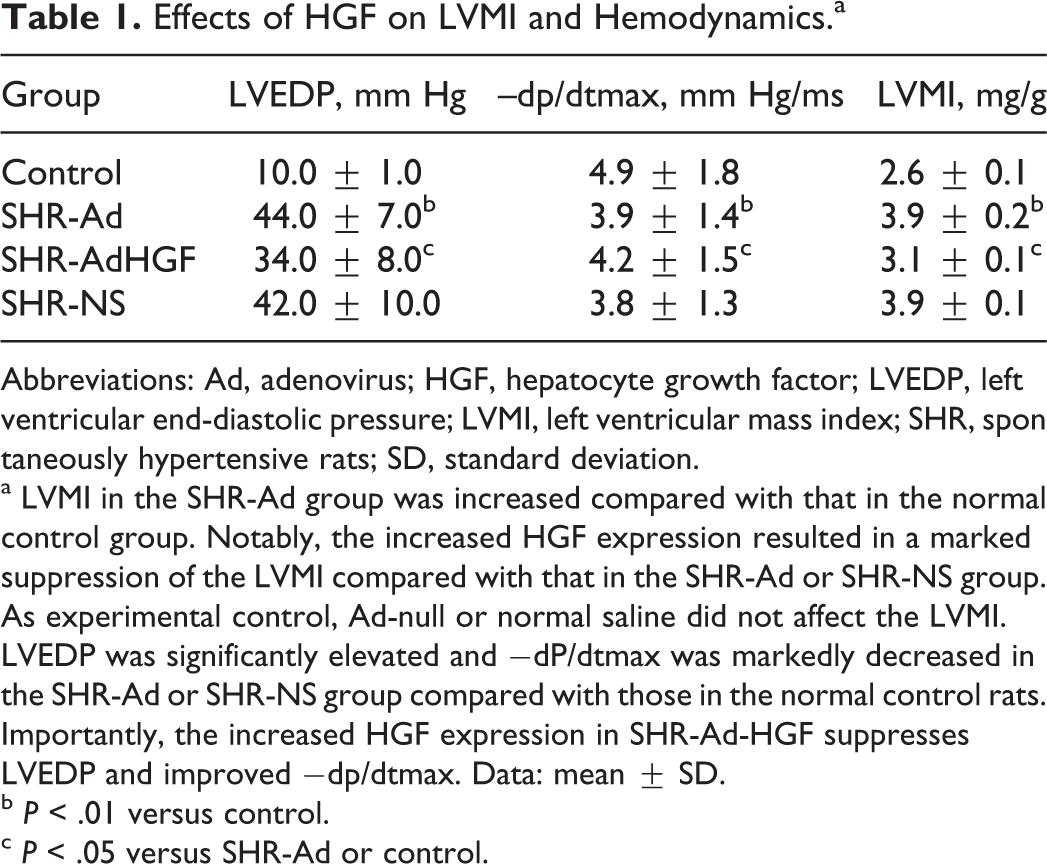
Abbreviations: Ad, adenovirus; HGF, hepatocyte growth factor; LVEDP, left ventricular end-diastolic pressure; LVMI, left ventricular mass index; SHR, spontaneously hypertensive rats; SD, standard deviation.
a LVMI in the SHR-Ad group was increased compared with that in the normal control group. Notably, the increased HGF expression resulted in a marked suppression of the LVMI compared with that in the SHR-Ad or SHR-NS group. As experimental control, Ad-null or normal saline did not affect the LVMI. LVEDP was significantly elevated and −dP/dtmax was markedly decreased in the SHR-Ad or SHR-NS group compared with those in the normal control rats. Importantly, the increased HGF expression in SHR-Ad-HGF suppresses LVEDP and improved −dp/dtmax. Data: mean ± SD.
b P < .01 versus control.
c P < .05 versus SHR-Ad or control.
The SHR had a significantly increased LVEDP and diminished −dP/dtmax (vs normal control rats, P < .05), and the injection of Ad-null or normal saline had no effect. Concurrent with the modification of collagen I, myocardial fibrosis and LVMI in the SHR with overexpression of HGF, the hemodynamic data were also significantly improved (vs injection of Ad-null or normal saline, both P < .01, n = 6 in each group), indicating positive cardiac remodeling effect of HGF (Table 1).
Discussion
The present study demonstrated that myocardial HGF content is significantly reduced in the hearts of SHR. Second, HGF expression can be upregulated by injection of Ad-HGF locally into the LV free wall. Third, collagen I synthesis, myocardial fibrosis, and LVMI all are markedly increased in the hypertensive hearts; these changes are associated with an increase in LVEDP and a reduction in −dP/dtmax. Importantly, these pathological and hemodynamic changes can be attenuated by upregulating myocardial HGF gene expression.
Regulation of HGF Expression in Hypertensive Cardiomyopathy
The evolution of hypertensive cardiomyopathy, cardiomyocyte hypertrophy, myofibrillar disarray, and myocardial interstitial fibrosis leads to a heterogeneous cardiac remodeling that increases ventricular wall stiffness and impairs cardiac diastolic function. 14,15 The most commonly used pharmacological agents to attenuate hypertensive myocardial remodeling are angiotensin-converting enzyme inhibitors, angiotensin II type 1 receptor blockers, and β-blockers. These drugs have indeed improved morbidity and mortality of these patients. Nevertheless, the rates of morbidity and mortality are still high in patients with hypertensive cardiomyopathy. An appropriate treatment of hypertensive cardiomyopathy would include drugs or gene therapies that target underlying molecular mechanisms of the pathologic process.
The HGF is a multifunctional growth factor. Its biological effects are mediated by its specific receptor c-Met, triggering protein phosphorylation of tyrosine kinase. 5 Studies in vitro have demonstrated that an increase in HGF expression inhibits apoptosis, 12 promotes angiogenesis, 7 and reduces the generation of extracellular matrix. 16 Studies in the animal models of ischemia–reperfusion injury have shown that HGF induces myocardial protection and improves cardiac function. 6,17 However, the effects of HGF in hypertensive cardiomyopathy have not been examined so far.
In this study, we explored the potential beneficial effects of overexpression of HGF gene on cardiac hypertrophy and fibrosis and LV relaxation function. In fact, we found HGF expression to be significantly reduced in the myocardium of SHR. The HGF gene expression could be readily upregulated by multiple injections of Ad-HGF, which resulted in diffused overexpression of HGF protein throughout the LV. Importantly, the increase in HGF expression in the myocardium reduced cardiac hypertrophic and areas of fibrosis; this resulted in a marked reduction in LVMI and LVEDP and an improvement in the LV relaxation potential.
Role of HGF in Myocardial Remodeling and Its Effect on Hemodynamics
It is widely appreciated that structural remodeling of the myocardium, including cardiac hypertrophy, fibrosis, and capillary formation (angiogenesis), determines the functional state in various acquired and hereditary cardiomyopathies. 18,19 Collagen turnover is known to be much greater in patients with hypertensive cardiomyopathy than in normal participants. 20,21 Interstitial fibrosis is also a morphological characteristic of hypertensive cardiomyopathy and results in stiffness (as evident from measurement of LVEDP) and impaired relaxation pattern.
Several studies have documented that HGF is an important antifibrotic factor. 22 It reduces extracellular matrix generation, activates MMP-1, and increases matrix degradation through the inhibition of angiotensin II and transforming growth factor β1. 12 In animal models of acute myocardial infarction and heart failure, it is evident that the increase in HGF by gene transfection inhibits cardiac fibrosis and improves LV function. 23,24 However, a similar pattern has not been shown previously in patients with hypertensive cardiomyopathy.
In this study, we demonstrated that collagen I and myocardial fibrosis are significantly increased in SHR with cardiac remodeling. Myocardial fibrosis was associated with significant functional deterioration, same as in chronic ischemia models. Importantly, the measures of pathological process were suppressed by upregulation of HGF, resulting in improvement of the cardiac function.
In summary, the current study shows that insufficiency of HGF is an important determinant of cardiac remodeling associated with sustained hypertension. Importantly, this study shows that a selective upregulation of HGF has the potential to reverse the adverse cardiac remodeling associated with this common malady.
Footnotes
Authors’ Note
Drs Hu and Bao contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by grants from Anhui Provincial Natural Science Foundation (11040606M157 and 11040606Q20).