
Abstract
Aims:
The aims of this study were (1) to explore physicians’ self-reported treatment of patients with dyslipidemia and (2) to identify intercountry differences and associations between physicians’ characteristics and treatment patterns.
Methods:
A cross-sectional survey was performed in primary health care in 9 Central and Eastern European countries. An anonymous questionnaire, which included questions devoted to dyslipidemia treatment, was distributed.
Results:
A total of 3000 physicians were randomly chosen and 867 responded. The mean percentage of physicians in all countries who reported regular use of statins in primary prevention of cardiovascular diseases (CVD) was 86.4 (range between 91.0% of Polish physicians and 75.7% of Czech physicians; P < .01). In secondary prevention, the mean percentage was only a little higher, 89.9. The use of fibrates for primary prevention was reported by 40.3% of the respondents from Bulgaria and by 2% of the respondents from Estonia (P < .01). Also, significant differences between countries were found in the use of fibrates and combination therapy in secondary prevention. Atorvastatin and simvastatin were the most prescribed drugs in everyday practice (the mean percentage of physicians in all countries was 72.5% and 68.0%, respectively). More than three-fourth of the respondents reported prescribing lifelong treatment with statins. Inconsistent associations were found between the characteristics of physicians and their treatment patterns.
Conclusions:
There are significant variations in the use of lipid-lowering drugs in Central and Eastern European countries; however, statin monotherapy predominates. Some physicians’ decisions are made without supporting evidence from clinical trials. There is still scope to improve preventive care of CVD.
Keywords
Introduction
Raised levels of blood lipids are common findings in patients with cardiovascular diseases (CVDs) and also in healthy individuals. They are associated with CVD development, morbidity, and mortality. Patients with blood lipid abnormalities require lifestyle modification and sometimes pharmacotherapy. 1 Statins have been shown to promote regression of coronary atherosclerosis 2,3 and are effective in this respect for primary 4 and secondary 5 prevention of CVD.
Lovastatin was the first statin approved by the US Food and Drug Administration and became available for prescription in 1987. 6 Simvastatin and pravastatin were introduced in the early1990s. Landmark statin trials were published between 1990 and 2000. Moreover, in 1994 the first joint European guidelines which included recommendations about dyslipidemia treatment were issued. 7
In Central and Eastern European countries, pivotal political changes started in 1989 and have also encompassed health care systems. 8 The Soviet model of care, which was centrally planned and run by the government, was abandoned. In the 1990s, new regulations regarding drug registration, prescription, and reimbursement were introduced. In this part of Europe the first statin, lovastatin, was introduced in Yugoslavia (registration in 1989, on the market since 1990). In the mid-1990s of the last century, lovastatin shortly followed by other statins became available in all countries of the region. Former Communist countries also undertook reforms in primary care, where family physicians/general practitioners would have broad responsibilities in health promotion and disease prevention. 9
In Central and Eastern European countries, the emphasis on prevention of CVD has a great importance since these diseases are a leading cause of death and disability. Moreover, their prevalence is higher than in Western Europe or in the United States. 10 The role of primary care physicians in CVD prevention is of the utmost importance, both in large-scale population strategies and clinical strategies identifying individuals at the practice level. 11
In spite of these facts, only a few articles analyzing management of dyslipidemia in Central and Eastern European countries have been published in the international literature. 12 –14 Some of them suggest that lipid-lowering therapy is underused in these countries in comparison to other geographical areas. 15 Although some examples can be found, 16 not many are published in national languages.
This study was performed with the aims (1) to explore primary care physicians’ self-reported treatment of patients with dyslipidemia in Central and Eastern European countries; (2) to identify intercountry differences in physicians’ self-reported use of statins and fibrates in patients with elevated lipids levels; and (3) to investigate the association between physicians’ characteristics and their reported treatment of dyslipidemia.
Methods
Design
This study used a descriptive, observational design. It was performed as a cross-sectional survey investigating primary care physicians’ self-reported behavior in everyday practice.
Study Sample
The random samples of primary care physicians from Bulgaria (BG), Czech Republic (CZ), Estonia (EE), Hungary (HU), Lithuania (LT), Latvia (LV), Poland (PL), Slovakia (SK), and Slovenia (SL) were chosen from the national registers. A primary care physician was defined as provider of initial care for patients at the point of entry into the health care system, who completed vocational training in family medicine/general practice (FM/GP) or internal medicine or without any vocational training. The size of the samples varied from 150 to 500 and depended on the expected response rate to achieve at least 50 responses from smaller countries (EE, LT, LV, SK, and SL) and at least 100 from the remaining ones. In total, 3000 physicians were included in this study.
Questionnaire
The postal questionnaire, consisting of 3 parts, was used as a research tool. The first part explored the demographic and professional characteristics of the respondents, while the second and third ones contained, respectively, questions about the clinical management of common cardiovascular and gastrointestinal problems. The questionnaire has already been published as a supplemental digital content to our previous article. 17 Four questions in the cardiovascular part of the questionnaire were devoted to the use of lipid-lowering medicines in everyday practice. All of them had itemized answers to be judged on the Likert scale. The draft version of the questionnaire was developed by the core study group and then piloted in each of the participating countries. The final version of the questionnaire was translated into the respective languages of the countries being studied using rigorous methodology. The questionnaires were distributed by surface mail, followed by written and telephone reminders to nonrespondents. Responses were collected locally, but the data entry process was done centrally in the study coordinating center, which was also responsible for the data analysis. The main measures included self-reported (1) lipid-lowering drugs regularly used for primary prevention (asymptomatic patient with increased total and low-density lipoprotein cholesterol [LDL-C] and triglycerides [TGs]); (2) lipid-lowering drugs regularly used for secondary CVD prevention (patient with established CVD and increased total cholesterol (TC) and LDL-C and TGs); (3) types of statins prescribed in practice; and (4) duration of statin treatment.
The study was performed between October 2007 and February 2008 and a detailed description of the study design, participants, research tool, and its validation has been already published elsewhere. 17,18
Statistical Analysis
To present the characteristics of the respondents, measures of central tendency and measures of dispersion (mean and standard deviation) were calculated for quantitative features and the percentage distribution for variables measured on a nominal scale. For questions with answers on the Likert scale options were grouped to present the study results “never” with “sometimes” and “usually” with “‘always”. To compare country results the chi-squared test was used. Analyzing the association of decisions with age and experience in GP (in years) the Kruskal-Wallis test was used for question on statin treatment recommended to patients (with 4 nominal categories of answer) and the Gamma correlation coefficient was calculated for other questions using Likert scale options for answers (as it is preferable to Spearman R when the data contain many tied observations). Statistical significance was set at the 0.05 level.
The study was conducted under the terms of all relevant local legislation and the protocol conforms to the ethical guidelines of the 1975 Helsinki Declaration. Ethical committee approval was not obtained because the study did not involve patients or human material and was lawfully acceptable.
Results
Respondents’ Characteristics
Of the 3000 primary care physicians invited to participate, 867 responded. The intended number of responses (at least 50 doctors among the smaller nations and 100 doctors among the larger nations) was achieved among all the countries studied except for LT, where only 31 physicians replied. The overall response rate was 28.9% (the highest in the CZ: 85.6%, and the lowest in LT: 20.7%).
The mean age of the primary care physicians was 49.3 (standard deviation [SD]: 9.0) years. Their mean experience in primary care practice was 18.5 (SD: 10.0) years. The respondents group consisted of 33% male and 67% female doctors. Only in HU male physicians prevailed (59%). In all, 82% of the respondents specialized in FM/GP. The mean number of patients from the respondents’ practices was 2236. In all, 59% of the doctors provided care for urban, 21% for rural, and 20% for mixed dweller population. The detailed, country-by-country characteristics of primary care physicians participating in this study have been published previously. 18
Lipid-Modifying Medicines in Primary Prevention of CVD
The majority of the respondents (N = 729) declared regular prescription of statins in primary prevention of CVD (the mean percentage of physicians in all countries: 86.4). Less than one-fourth of the physicians (N = 194) reported giving fibrates and about one-tenth (N = 103) combination therapy with statins and fibrates (the mean percentage of physicians in all countries: 18.2 and 11.3, respectively). The use of statins and fibrates in lipid-modifying therapy in primary prevention of CVD is presented in the upper part of Figure 1.

Percentage of respondents reporting the use of particular lipid-modifying medicines in primary and secondary prevention of cardiovascular diseases (CVD).
The highest percentage of respondents admitting statin use in primary prevention of CVD was in PL (91.0%) and the lowest in CR (75.7%). The difference between all the countries was statistically significant (P < .01).
The use of fibrates for primary prevention was reported by 40.3% of the respondents from BG and only by 2% of the respondents from EE. Although none of the Estonian physician declared the use of combination therapy in primary prevention, it was done by 32.5% of the doctors from BG. The differences between the countries were statistically significant for both the above-mentioned types of therapy (P < .01).
The use of statins in primary prevention of CVD did not correlate with any of the respondents’ characteristics taken into analysis in this study. The use of fibrates was more often declared by physicians from large cities than from villages (31.3% vs 20.4%; P < .01). Combination therapy was declared to be used by 23.0% of the physicians without specialization in FM/GP and 9.1% of the physicians who had this speciality (P < .01). Older physicians would more often prescribe combination therapy. This correlation, although statistically significant (P < .01), was very weak (gamma correlation coefficient = 0.07).
Lipid-Modifying Medicines in Secondary Prevention of CVD
The vast majority of primary care physicians participating in the study (N = 782) confirmed the use of statins in secondary prevention of CVD (the mean percentage of physicians in all countries: 89.9). Fibrates were reported to be prescribed by 171 of the physicians and combination therapy by 139 of the physicians (the mean percentage of physicians in all countries was 17.1 and 16.0, respectively).
Significant differences were found between countries included in the study. Although 99.0% of Polish primary care physicians reported the regular use of statins in secondary prevention, only 81.6% of the Bulgarian doctors declared doing the same (P < .01).
In all, 38.6% of the doctors from BG and 3.8% of the doctors from SL (P < .01) confirmed the use of fibrates in secondary prevention of CVD. Although only 2% of the respondents from EE declared the use of the combination therapy, 32.2% of those in LT reported treatment with statins and fibrates (lower part of Figure 1).
Slightly more male than female respondents declared the use of statins in secondary prevention of CVD (94% vs 88.6%; P <.05). Also, more male (21.1%) than female (13.7%) physicians reported the use of fibrates (P < .01). There was an association between the therapy prescribed and the respondents’ specialty. The use of statins was reported by 91.1% of the doctors specialized in FM/GP and 85.9% of the doctors without this specialty (P < .05). By comparison, more physicians without a specialty in FM/GP would prescribe fibrates (29.4% vs 17.2%; P < .01).
Types of Statins in Cholesterol-Lowering Treatment
Approximately 3 out of 4 respondents from all countries included in the study declared the use of atorvastatin (the mean percentage of physicians in all countries: 72.5) and two-thirds the use of simvastatin (the mean percentage of physicians in all countries: 68.0), in lipid-lowering treatment. Only a minority of respondents reported the use of other types of statins.
The differences between particular countries were significant. Although atorvastin was declared to be used by 89.6% of the respondents from LV, only 33.3% of the Estonian doctors reported the use of this medication (P < .01). On the other hand, 52.9% of the primary care doctors from EE admitted to the treatment with rosuvastatin, while only 2% of the respondents from PL and 3.5% from SK declared the same (P < .01). Details about types of statins used in lipid-lowering treatment in particular countries are presented in Figure 2.
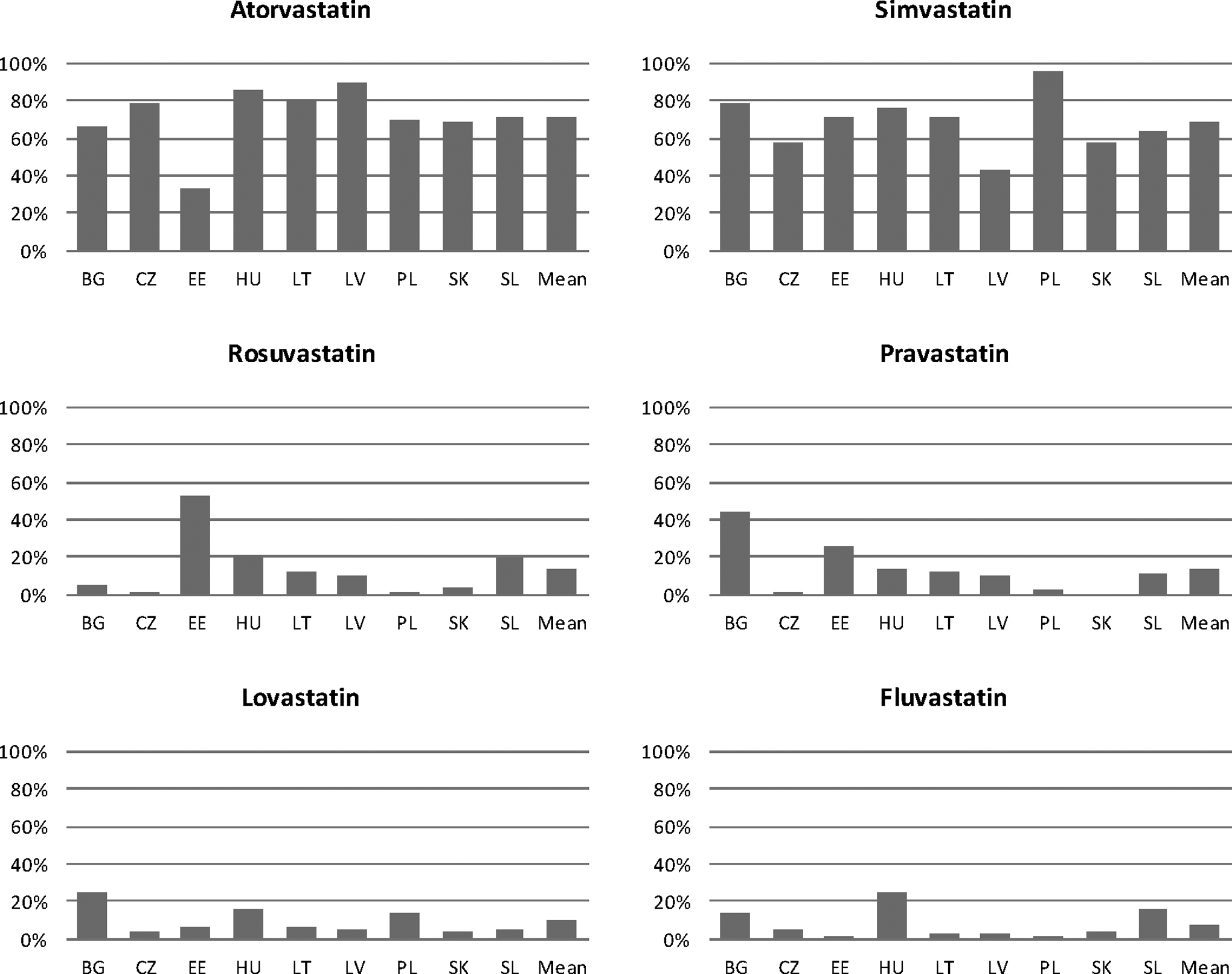
Percentage of respondents reporting the use of specific type of statins in prevention of cardiovascular diseases (CVD).
More male than female respondents reported the use of atorvastatin (79.2% vs 71.8%; P <.05). Simvastatin was declared to be used by 77.6% of the physicians with a specialty in FM/GP and 66.5% of the physicians without this specialty (P < .01). In contrast, more doctors without a specialty in FM/GP admitted the use of lovastatin (17.9% vs 8.3%; P < .01). A weak relationship was found between the age of respondents and the type of statins used in everyday practice. Older doctors were less likely to prescribe simvastatin, atorvastatin, and pravastatin than the younger ones (gamma correlation coefficient between −0.07 and −0.12; P < .05).
Duration of Statin Treatment
Of the 4 respondents, 3 reported that for patients with elevated LDL-C they usually recommended lifelong treatment with statins (the mean percentage of physicians in all countries: 75.4). In PL and HU 90.7% and 89.4% of the physicians, respectively, would order such a therapy (Figure 3). On the other hand, the same therapeutic decision would be made by 41.8% of the primary care doctors from LV (P < .01). Twenty-six percent of the physicians from this country would order statin treatment for a period of 1 to 5 years and the rest (13.4% of the physicians) for several months or until achieving LDL-C target levels (17.9% of the physicians). Differences between particular countries are significant (P < .01).

Percentage of physicians reporting specified duration of statin treatment to their patients.
Only 1 of the respondents’ characteristics (a specialty) correlated with the duration of statin treatment reported by primary care physicians. Lifelong therapy would be prescribed by 82% of the doctors with a speciality in FM/GP and 59.7% of the doctors without this specialism (P < .01).
Discussion
Main Findings
This cross-sectional study was carried out in order to get new insights into lipid-modifying drug therapy in Central and Eastern European countries. It was shown that the vast majority of primary care physicians reported the use of statins both in primary and secondary prevention of CVD. The use of fibrates and combination of statin–fibrate was declared by a much lower proportion of doctors. Atorvastatin and simvastatin were found to be the drugs, which doctors would prescribe most frequently in hypercholesterolemia treatment. Significant differences were found between countries included in the study in the field of lipid-lowering pharmacotherapy. Only weak and inconsistent associations were found between the characteristics of primary care physicians and their self-reported practice in the treatment of patients with elevated lipid levels.
Strengths and Limitations
To decrease selection bias, we chose a random sampling procedure and implemented it in all countries included in the study. Although the response rate in particular countries was not very high, it was comparable to similar surveys published in other major journals (10%-45%). 19 We are aware that the level of nonresponse to some extent limits the generalizability of the results. On the other hand, we reached a predefined number of participants in all countries (except LT) and this allowed us to draw a comparison between the countries. The overall high number of physicians participating in the study enabled a precise estimation of the association between the characteristics of respondents and their choice of lipid-lowering drug therapy.
With respect to measurement bias, it is necessary to highlight the fact that we did not study the real medical prescriptions (eg, from medical records or national/regional registers or practice observation) but only self-reported selection of drugs. Due to this fact a translation of the results from our study to everyday practice in Central and Eastern European countries is limited (as in most similar surveys). It is known that self-reported physicians’ data are likely to overestimate the practice. 20 This means that the everyday, routine practice of primary care doctors may look inferior to those presented in our study. To minimize measurement bias, several precautions were undertaken. First, a rigorous questionnaire translation procedure was implemented. Second, the face and content validity of the questionnaire was assessed (described previously). 18 Moreover, a large number of primary care physicians included in the study should be considered as a factor, which improves the quality of the results obtained.
Comparisons With Other Studies
In HU, like in our study, the vast majority (85%) of patients with dyslipidemia received statin monotherapy, only 10% received fibrates, and 5% received a combination regimen. 13 In Croatia, 87% of the physicians prescribed lipid-lowering treatment to every patient with CVD. 14
Walley et al obtained administrative data from the governmental or insurance fund sources in 13 European countries and described the lipid-lowering drug prescription. Statins predominated in all countries and similar to our results the most commonly used were simvastatin and atorvastatin. The use of fibrates was far lower than statins and only in France and Belgium they consisted of approximately 25% of all lipid-lowering agents. 21
A REALITY study, which was conducted in 10 European countries, showed that statin monotherapy was the initial treatment for 89.3% of the patients (ranging from 59.6% in France and 98.1% in Norway). Simvastatin and atorvastatin were the most commonly prescribed drugs. 22 In Finland 23 and Norway, 24 the majority of physicians also prescribed simvastatin or atorvastatin. On the other hand, pravastatin was the most popular statin in Ireland. 25
Stacy and Egger revealed that in the United States 87% of the patients were prescribed a single lipid modification medication and almost 90% of them received a statin, while 13% of the patients were prescribed combination therapy. 26
With regard to combination therapy of statins and fibrates, it was shown that such a prescription was seldom observed in Germany. 27 The REALITY study revealed that in Europe only 1% of the patients received combination therapy at the beginning of the treatment. 22
There is a lack of consensus with regard to the duration of statin therapy. No expert panel has made clear recommendations regarding how and when to stop statin treatment unless contraindicated. 28 The problem of discontinuation of this therapy was analyzed by Korhonen et al. They showed that in Finland almost half of the patients who initiated statin treatment had stopped it for at least 180 days. 29 The evidence suggests no increase in adverse outcomes following discontinuation of the therapy with statin in asymptomatic patients and those with stable chronic coronary artery disease. Conversely, under conditions of acute coronary syndrome, acute ischemic strokes or vascular surgery, cessation of statins is contraindicated. 30,31
Backlund et al studied GPs’ decisions in lipid-lowering drugs prescription and showed that doctors who adhered to the guidelines were younger than those who did not. 32 In our study, some of the correlations between the personal characteristics of respondents and the self-reported treatment of dyslipidemia were very weak.
Interpretation of Study Findings
In general, results concerning the use of statins for primary and secondary prevention of CVD in Central and Eastern European countries can be interpreted as satisfactory. The vast majority of primary care physicians reported the prescription of these drugs for the patients. Nonetheless, there are some countries (eg, the CZ) where the use of statins is lower. This fact can be explained by a special prescription regulation in the Czech health care system. The use of statins in primary prevention is limited to persons with CV score >5% and coprescription of statins and fibrates is limited to secondary care.
Physicians, from our study, would be more likely to order cheaper types of statins which can be replaced by generic equivalents. This approach agrees with current recommendations. The clinical benefit of hypercholesterolemia treatment is independent of the type of statins and relies on the extent of LDL-C lowering.
This study revealed intercountry variations in the type of statin used in everyday practice. Since there was not a strong relationship between the personal characteristics of primary care doctors and their prescription patterns, it seems that other factors are more important in Central and Eastern European countries. The differences in health care organization, insurance system, and reimbursement regulations might be those possible factors. Moreover, doctors’ and patients’ preferences, the cost of a particular medicine, and availability of generic parallels influence physicians’ prescription patterns.
There is only limited data about the influence of a physicians’ gender on the prescribed therapy in CVD. The fact that slightly more male physicians reported the use of statins and fibrates in our study is in accordance with the general trend described by Lagro-Janssen, who found that male physicians prescribed medications more frequently. 33 On the other hand, Guoni-Berthold et al suggested that female doctors in diseases such as CVD might provide higher quality care because they are more interested in prevention, more effective in communication, and encourage patients to participate in decision making. 34 The doctors’ gender discrepancies revealed in our study cannot be a basis for a conclusion about a difference in quality of care.
Other studies reported that in Eastern and Central Europe the achievement of lipid target levels is much lower than in Western Europe. Paragh et al showed that 26% of the Hungarian patients achieved their treatment goals for TC and LDL-C. 13 The WOBASZ 35 and LIPIDOGRAM 36 studies conducted on a random sample of Polish patients reported target levels attainment in less than 25% of the population. On the other hand, studies across Western European countries found that on average, approximately 40% of the patients met their cholesterol level goals and the highest percentage was shown in France (more than 50%). 22,37
Regarding therapy with fibrates, there are obvious gaps between the reported practice and the recommendations from international guidelines. In our study, almost the same percentage of physicians (about 20%) reported the use of fibrates for primary and secondary prevention of CVD. This percentage should be interpreted as very low in secondary prevention, while in primary prevention it is surprisingly high. As recommended in the European Society of Cardiology/European Atherosclerosis Society 38 and National Institute for Health and Clinical Excellence 39 guidelines fibrates should not routinely be offered for primary prevention. They may be considered (after introduction of lifestyle measures) when statins are not tolerated, patients are at high total CVD risk, and TG is above 2.3 mmol/L (200 mg/dL). Our results suggest that fibrates are still not used in secondary prevention as energetically as they should be. On the other hand, they may be being prescribed without proper justification in primary prevention.
Moreover, the combination of statins and fibrates in secondary prevention was reported to be prescribed only by a small proportion of physicians. This fact indicates another inadequacy in dyslipidemia treatment in Central and Eastern Europe. According to guidelines, this treatment can be beneficial and improve attainment of lipid goals especially in patients with atherogenic combined dyslipidemia and diabetes mellitus or metabolic syndrome. 38
Long-term statin therapy reported by physicians in this study is in accordance with current evidence. The Heart Protection Study Collaborative Group gives support for the prompt initiation and long-term continuation of statin treatment. 40 Kohli and Cannon reviewed the evidence from several other RCT and concluded that prolonged treatment with stains is safe, efficacious, and beneficial. 41
Implication of This Study
We believe that the results from this study may be of significant value for primary care physicians and especially public health professionals.
First, doctors providing primary care in Central and Eastern European countries should be aware of possible gaps between their everyday practice and current clinical guidelines in the area of dyslipidemia treatment. These gaps mainly relate to the use of fibrates and combination pharmacotherapy. As a consequence, doctors should identify their personal educational needs and start making a plan to update the necessary knowledge and skills. They should also pay attention to potential harm associated with unnecessary lipid-modifying pharmacotherapy for primary prevention, especially in patients with a low CVD risk.
Second, public health professionals from Central and Eastern European countries should realize that, in spite of evidence-based recommendations and the availability of effective drugs, there is considerable room for progress and improvement in cardiovascular preventive care. Administrative regulations and bureaucratic controls, which are widely used in post-communist countries, may not be effective to guarantee the improvement of quality of care over a longer period. Probably, several strategies have to be implemented, although the focus should be put on internal quality improvement methods. 42
Finally, this study suggests areas for future research which in the opinion of the authors of this article should be directed toward the identification of the real barriers which limit cholesterol goals achievement in primary care in Central and Eastern European countries.
Conclusion
The results of our study allow us to conclude that dyslipidemia treatment in primary care in Central and Eastern European countries is predominated by statin monotherapy.
There are discrepancies between lipid-lowering treatment recommendations from international guidelines and physicians’ self-reported routine practice. These discrepancies relate mainly to the use of fibrates and combination drug therapy.
There are significant variations in the use of lipid-lowering drugs between Central and Eastern European countries and these variations cannot be explained by the characteristics of primary care physicians but rather by financial or organizational factors.
There is still scope to improve preventive management in primary care settings in Central and Eastern Europe in order to reduce the risk and burden of CVD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work in the phase of planning and data collection was supported by an unrestricted grant from Zentiva.