
Abstract
Aim:
Ventricular arrhythmia (VA) is a risk for sudden death. Polymorphic ventricular tachycardia (VT) degenerating to ventricular fibrillation occurs subsequent to the prolongation of the QT interval following administration of catecholamines under Ca2+ loading. Fatal VA also occurs in ischemia and ischemic–reperfusion. We compared the suppressive effect of K201 (JTV519), a multiple-channel blocker and cardiac ryanodine receptor-calcium release channel (RyR2) stabilizer, with that of diltiazem, a Ca2+ channel blocker, in 2 studies of isoproterenol-induced (n = 30) and ischemic–reperfusion-induced VAs (n = 38) in rats.
Methods:
Adult male Wistar rats were administered 12 mg/kg/min calcium chloride (CaCl2) for 20 minutes and then 6 μg/kg/min isoproterenol was infused with CaCl2 for a further 20 minutes. In other rats, the left coronary artery was ligated for 5 minutes followed by reperfusion for 20 minutes. K201 or diltiazem (both 1 mg/kg) was administered before infusion of the isoproterenol or induction of ischemia.
Results:
After administration of isoproterenol under Ca2+ loading, fatal VA frequently occurred in the vehicle (9 of 10 animals, 90%) and diltiazem (8 of 10, 80%) groups, and K201 significantly suppressed the incidences of arrhythmia and mortality (2 of 10, 20%). In the reperfusion study, the incidence and the time until occurrence of reperfusion-induced VA and mortality were significantly suppressed in the K201 (2 of 15 animals, 13%) and diltiazem (1 of 9 animals, 11%) groups compared to the vehicle group (8 of 14 animals, 57%).
Significance:
Induction of VA in an experimental model was achieved with a low dose of isoproterenol under Ca2+ loading. K201 markedly suppressed both the isoproterenol-induced and the reperfusion-induced VAs, whereas diltiazem did not suppress the isoproterenol-induced VA. The results suggest that both VAs are related to early after depolarization (EAD) and indicate that K201 has the potential to suppress EAD by stabilizing RyR2 to mediate Ca2+ release from the sarcoplasmic reticulum and acting as a multiple-channel blocker.
Keywords
Introduction
Ventricular arrhythmias (VAs) such as ventricular tachycardia (VT) and ventricular fibrillation (VF) are potentially fatal arrhythmias and a risk for sudden cardiac death. 1 VAs develop during reperfusion therapy for acute myocardial infarction. 2 Catecholamines also induce VA in patients with ischemic heart disease and heart failure. 3 Therefore, elucidation of the pathogenic mechanism of VAs is important for the development of therapeutic agents. The general processes involved in the pathogenesis of VA with tachycardia include abnormal automaticity, triggered activity, and re-entry. Triggered activity is a transient depolarization that occurs following early after depolarization (EAD) and delayed after depolarization (DAD). 4 Marked prolongation of the QT intervals induces torsades de pointes (TdP) and EAD that has been associated with the L-type Ca2+ channel (LTCC) or Na+/Ca2+ exchanger. 5 DAD accompanies diastolic Ca2+ release from the sarcoplasmic reticulum following an increase in the intracellular Ca2+ concentration ([Ca2+]i) ie, cellular Ca2+ overload. 1 Simultaneous appearance of both EDA and DAD has been shown experimentally in monophasic and transmembrane action-potential recordings. 1,4
K201 (JTV-519) is a 1,4-benzothiazepine derivative ([4-{3-(4-benzylpiperidin-1-yl) propionyl]-7-methoxy-2,3,4,5-tetrahydro-1,4-benzothiazepine monohydrochloride; C25H32N2O2S·HCl; MW:461.07) that was developed as a drug with a stronger myocardial protective effect than Ca2+ channel blockers and β-adrenoceptor blockers but with extremely weak negative inotropic and chronotropic effects. 6 Based on the molecular and cellular studies, K201 has multiple actions on the cardiac function as an α1-blocker, 6,7 a multiple-channel blocker, 7,8 and a stabilizer of the cardiac ryanodine receptor-calcium release channel (RyR2) in the sarcoplasmic reticulum. 9,10 RyR2 is a large tetrameric channel that mediates Ca2+-induced Ca2+ release (CICR) of intracellularly stored Ca2+ into the cytosol following opening of the voltage-dependent sarcolemmal LTCC during action potentials. 11 –13
In this study, we evaluated the suppressive effect of K201 on VAs in an isoproterenol-induced rat model of VA under Ca2+ loading and in ischemic–reperfusion-induced VA after coronary artery ligation. This effect was compared with that of diltiazem, a 1,5-benzothiazepine derivative and Ca2+ channel blocker.
Materials and Methods
Experimental Procedure
Sixty-eight adult Wistar male rats (body weight 260-320 g) were used in the study. The study was conducted in accordance with the animal ethics code of Dokkyo Medical University, after approval by the University Animal Ethics Committee.
All animals were anesthetized, endotracheally intubated with a polyethylene tube (SP102, Natsume, Seisakusho Co Ltd, Tokyo, Japan), and mechanically ventilated with a tidal volume of 2 mL at a rate of 60 strokes/min using a ventilator (SN-48-7; Shinano Manufacturing Co Ltd, Tokyo, Japan). A micromanometer-tipped pressure catheter (2F, SPC-320, Millar Instruments Inc, Houston, Texas) was inserted from the right cervical artery to measure the aortic pressure or ventricular pressure and the heart rate. A polyethylene tube for solution injection was inserted from the right femoral vein and test solutions were administered using a continuous injector. An electrocardiographic (ECG) apparatus was attached to the extremities of the animals and lead II was monitored. ECGs and pressure curves were stored on a personal computer (Power Lab, AD Instruments Ltd, Sydney, Australia).
In the 2 studies described in the following section, the animals were randomly assigned to 3 groups: vehicle (5% glucose), K201 (1 mg/kg), and diltiazem (1 mg/kg). Each drug was dissolved in 5% glucose solution.
Materials
K201 was provided by Aetas Pharma Co Ltd, Tokyo, Japan. Diltiazem and isoproterenol were obtained from Sigma, St Louis, Missouri. Isoflurane for animals was obtained from Mylan Seiyaku, Osaka, Japan.
Isoproterenol Administration Under Ca2+ Loading
Animals were anesthetized by inhalation of 3% isoflurane and maintained under 1.7% isoflurane anesthesia during administration of CaCl2 solution at 12 mg/kg/min for 20 minutes and then infusion of isoproterenol at 0.6 μg/kg/min with CaCl2 for a further 20 minutes. Vehicle, K201, or diltiazem (n = 10 animals in each group) was given in a volume of 1 mL within 1 minute at the beginning of infusion of isoproterenol.
An ECG was continuously recorded from 2 minutes before administration of CaCl2 solution for 40 minutes, except in cases of death. Heart rate and aortic pressure were recorded by ECG and measured from at least 5 complexes in the ECG before administration of CaCl2 (baseline), after 20 minutes of administration of CaCl2 (Ca2+ loading), and 20 minutes after administration of isoproterenol (Ca2+ loading + Iso). The double product (heart rate [beats/min]) × systolic aortic pressure [mm Hg]) was calculated using values measured before administration of CaCl2 (baseline), after 20 minutes of administration of CaCl2 (Ca2+ loading), and 1, 5, 10, 15, and 20 minutes after administration of isoproterenol. The mean value before administration was used as 100% and changes thereafter are given as percentages. The first time of occurrence and the number of incidences of polymorphic VT 7 and mortality were examined during the 20-minute period of isoproterenol administration.
Ischemic–Reperfusion Study
Animals were anesthetized in the same manner as describe above, endotracheally intubated, and mechanically ventilated. After midline thoracotomy, the pericardium was incised and the left anterior descending coronary artery was ligated with 6.0 polypropylene sutures for 5 minutes, followed by reperfusion in the vehicle (n = 14), K201 (n = 15), and diltiazem (n = 9) groups. K201 or diltiazem dissolved in 5% glucose solution were administered to animals of the treated group at a dose of 1 mg/kg/mL for 1 minute, 10 minutes before ligation of the coronary artery. The 5% glucose solution was given to animals in the vehicle group. The left ventricular pressure and ECG were recorded from 10 minutes before ligation to 20 minutes after reperfusion. The occurrence of ventricular tachycardia (VT) and fibrillation (VF), 7 the time until occurrence, and mortality were compared among the vehicle, K201, and diltiazem groups.
Statistical Analysis
Values are shown as means ± standard error (SE). Data analysis was performed by analysis of variance (ANOVA) followed by a Tukey test and Fisher exact test. The significance level was considered to be less than 5%.
Results
Isoproterenol Administration Under Ca2+ Loading
Heart rate remained unchanged after isoproterenol administration in the vehicle and K201 groups, but decreased 1 minute after isoproterenol administration in the diltiazem group, in which atrioventricular block occurred, and then recovered after 10 minutes. Aortic pressure significantly increased after 20 minutes of administration of CaCl2 in each group, compared to the data before administration, and decreased after 10 minutes of administration of isoproterenol (Table 1). In animals administered isoproterenol alone of the preliminary study, heart rate increased and arrhythmia did not occur for 40 minutes. The double product gradually decreased in the vehicle and K201 groups but fell at 1 minute, recovered, and then decreased in the diltiazem group. The double product in the diltiazem group was significantly reduced compared to the vehicle and K201 groups (P <.05 for both groups; Figure 1).
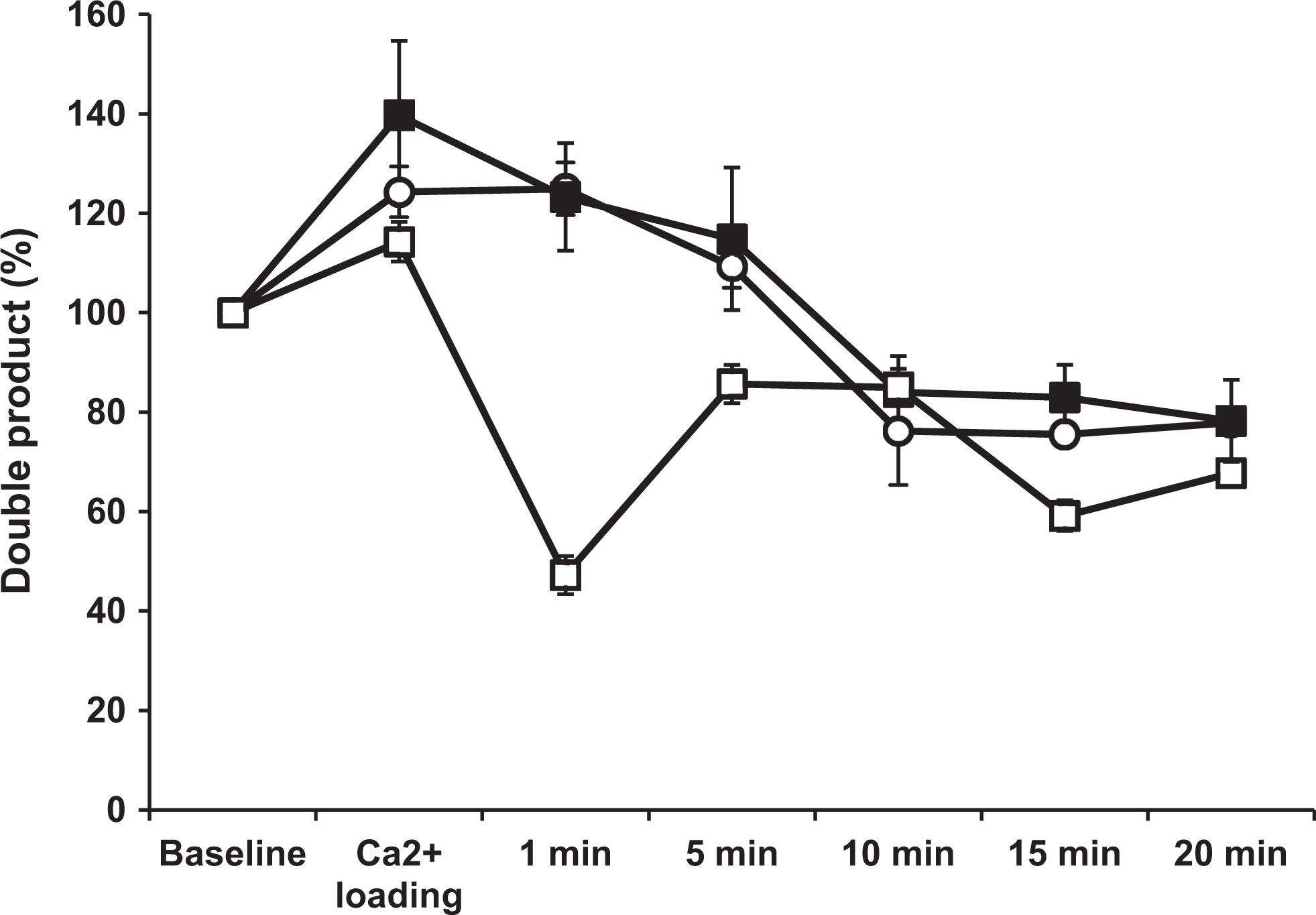
Double product. Changes in the double product after administration of isoproterenol vehicle (solid box), K201 (open circle), or diltiazem (open box). In the vehicle and K201 groups, the double product decreased and then reached a plateau after 10 minutes. In the diltiazem group, the double product significantly decreased after 1 minute, recovered, and then decreased again. The Ca2+ loading = after 20 minutes of administration of calcium chloride. Values represent mean ± standard error. The double product in the diltiazem group was significantly reduced compared to the vehicle and K201 groups (P < .05 for both groups).
Heart Rate and Aortic Pressure Before Ca2+ Loading (Baseline), After 20 minutes of Ca2+ Loading (Ca2+ Loading), and After Isoproterenol Administration With Ca2+ Loading. a

* P < 0.01 and ** P < 0.001 versus the respective value before Ca2+ loading and administration of isoproterenol and baseline.
aThe statistical analysis was not done 15 and 20 minutes after the administration of isoproterenol because of a small number.
No arrhythmias appeared before administration of isoproterenol. The isoprpterenol-induced VA waveform induced by isoproterenol is shown in Figure 2. Polymorphic ventricular tachycardia (VT) occurred, but monomorphic VT did not occur in any of the groups. Polymorphic VT occurred 14 times in the vehicle group, 13 times in the diltiazem group, and twice in the K201 group. The times until the initial occurrence of polymorphic VT were similar among the groups: 623 ± 53 seconds, 618 ± 24 seconds, and 676 ± 116 seconds in the vehicle, K201, and diltiazem groups, respectively. All animals with polymorphic VT occurred following VF and subsequently died. Thus, the mortality was high in the vehicle (9 of 10, 90%) and diltiazem (8 of 10, 80%) groups and significantly lower in the K201 group (2 of 10, 20%; P < .01 versus vehicle, P <.05 vs diltiazem; Figure 3).

Isoproterenol-induced ventricular fibrillation waveform. The bottom column shows the enlarged view.

Mortality of the isoproterenol-induced ventricular arrhythmia. The numbers in the figure indicate the mortality (death cases/all cases). **P < .01 versus the value of the vehicle group; †P < .05 versus the value of the diltiazem group.
Ischemic–Reperfusion-Induced Ventricular Arrhythmia
No VA occurred during ligation of the coronary artery in each group. The reperfusion-induced VF waveform is shown in Figure 4. Following reperfusion, the incidences of VT indicated that K201 (7 of 15 animals, 47%) and diltiazem (7 of 9, 78%) groups significantly suppressed VT compared to the vehicle group (14 of 14, 100%; P < .01 versus K201). The times until the occurrence of VT were 17.8 ± 7.1 seconds, 161 ± 75 seconds, and 185 ± 64 seconds in the vehicle, K201, and diltiazem groups, respectively, indicating significant prolongation of this time in both treated groups compared to the vehicle group (P < .05 and P < .01, respectively).

Ischemia–reperfusion-induced ventricular fibrillation waveform. The bottom column shows the enlarged view.
The incidences of VF in the K201 (3 of 15 animals, 20%) and diltiazem (3 of 9, 33%) groups indicated significant suppression of VF compared to the vehicle group (12 of 14, 86%; P < .001 and P < .05, respectively). The time until occurrence of VF was 505 ± 196 seconds in the diltiazem group that was significantly prolonged compared to the vehicle group (85 ± 25 seconds, P < .01). However, in the K201 group, the time, 154 ± 75 seconds, did not differ significantly from that in the vehicle group. Mortality in the K201 (2 of 15 animals, 13%) and diltiazem (1 of 9, 11%) groups was significantly lower than that in the vehicle group (8 of 14, 57%; P < .05 and P < .01, respectively; Figure 5).
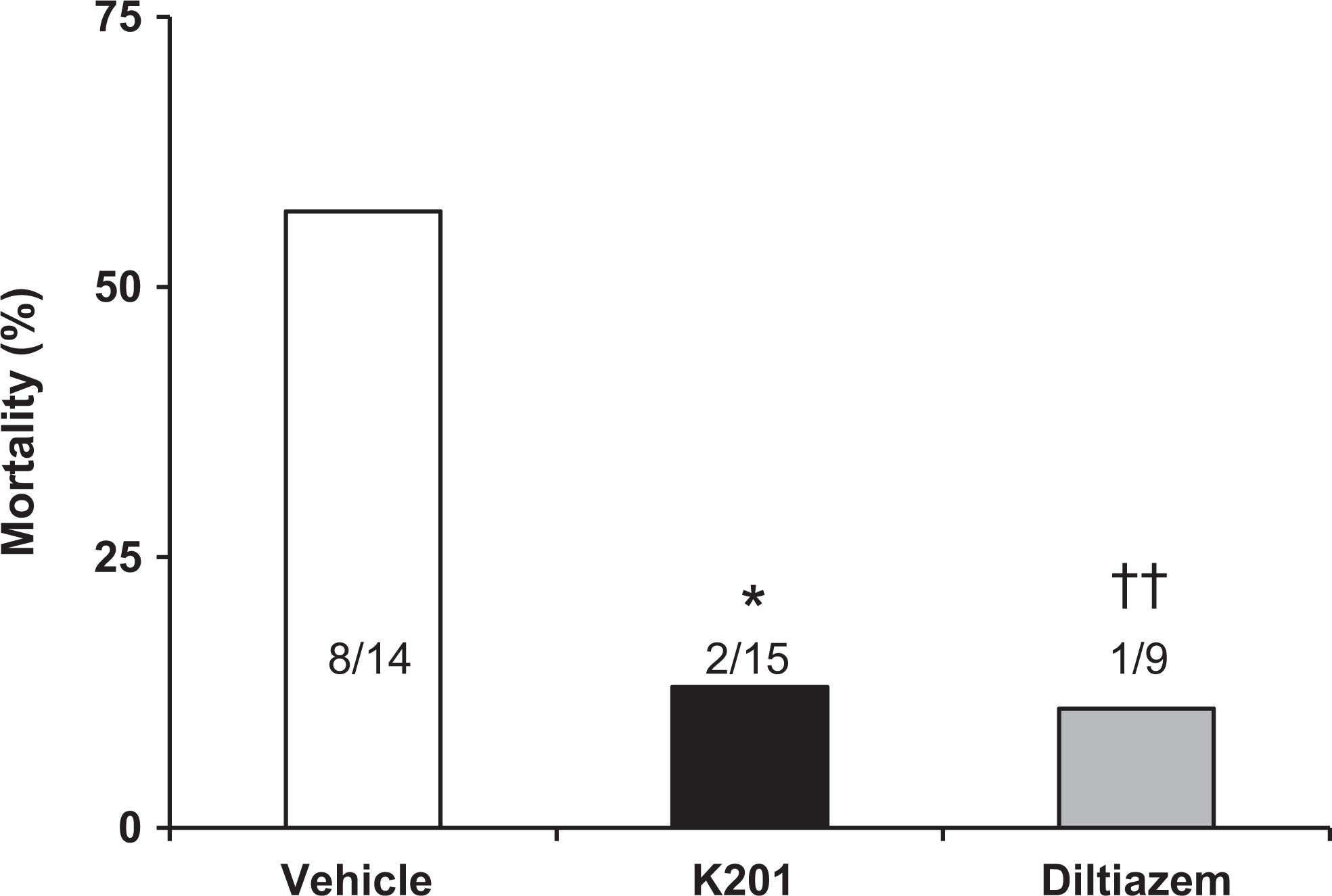
Mortality in the ischemic–reperfusion study. The numbers in the figure indicate the mortality (death cases/all cases). *P < .05; ††P < .01 versus the respective value of the vehicle group.
Discussion
The results of the first study showed a high incidence of polymorphic VT degenerating to VF during administration of low doses of isoproterenol under Ca2+ loading in anesthetized adult rats. This arrhythmia model was significantly suppressed by K201 but was not suppressed by diltiazem. In the second study, K201 and diltiazem significantly inhibited the occurrence of VT and VF after ischemic–reperfusion and decreased the mortality compared to the vehicle.
Heart rate and aortic pressure during isoproterenol administration with Ca2+ loading decreased 1 minute after the administration of isoproterenol and then rapidly recovered in the diltiazem group. The double product in the diltiazem group significantly reduced compared to the vehicle and K201 groups. The decrease in aortic pressure may reflect dilation of the peripheral vessels by isoproterenol itself in the vehicle and K201 groups. There was no relationship between the double product, which is an index of oxygen consumption in the heart, and the incidence of VA in the K201 and diltiazem groups.
The β-Adrenergic stimulation with isoproterenol at a low concentration also induces prolongation of the action potential duration (APD) and results in marked shortening at a higher isoproterenol concentration. 3 The Ca2+ loading in cardiomyocytes induces Ca2+ waves due to diastolic Ca2+ sparks in the cells, 14 and the Ca2+ wave depolarizes cardiomyocytes through activation of inward INa/Ca. 5 K201 has been shown to suppress spontaneous Ca2+ spark under Ca2+ loading in isolated normal myocytes 15 and improve the Ca2+ leak from the sarcoplasmic reticulum under Ca2+ overload in human failing myocardium. 16 In addition, Marx et al showed that RyR2 hyperphosphorylated by protein kinase A (PKA) dissociates from FK506 binding protein (FKBP) and induces Ca2+ loading, leading to malignant arrhythmia in patients with heart failure. 17 K201 increases the affinity of calstabin2 for RyR2 that stabilizes the closed state of RyR2 and prevents the Ca2+ leak that triggers arrhythmias. 9 K201 may inhibit isoproterenol-induced VA under Ca2+ loading through a RyR2 stabilizing effect, that is, an intracellular Ca2+ blocking effect. The lack of suppression of isoproterenol-induced VA suggests that diltiazem has no effect on the PKA-mediated Ca2+ release from the sarcoplasmic reticulum.
Diltiazem and K201 significantly reduced fatal VA after ischemic reperfusion. It is well known that [Ca2+]i overload frequently occurs with the ischemic–reperfusion and induces severe VA. Although LTCC participates in the development of reperfusion-induced arrhythmias, more evidence is accumulating that shows Na+/Ca2+ exchanger to play a critical role in cardiac injury. The occurrence of reperfusion-induced arrhythmia depends on the ischemic time immediately before reperfusion, the rate of ischemia progression, and the reperfusion rate. 4,18 The major reason for reperfusion-induced arrhythmia is excess Ca2+ influx through Ca2+ channels in the cell membrane. The class III antiarrhythmic agent amiodarone, 19 an angiotensin II type 1 receptor antagonist (candesartan), 20 and an activator of cardiac M3 muscarinic acetylcholine receptors 21 have also been reported to prevent fatal VA during acute ischemia and reperfusion.
EADs and DADs are action potential aberrations that can be proarrhythmic. Exposure to isoproterenol has been associated with generation of EAD and DAD. 3 DAD is commonly seen in [Ca2+]i overload due to ischemia and reperfusion or digitalis and catecholamines. In the present 2 studies, the ECG tracing indicated EAD due to the appearance after depolarization, and K201 suppressed their EADs. It has been reported that K201 is potent to prevent and suppress EAD and DAD by specific mechanisms of action. 22 Isoproterenol caused both EAD and DAD in guinea pig ventricular myocytes due to differences in changes in [Ca2+]i during EAD; increases in [Ca2+]i occurred simultaneously throughout the cell, whereas during DAD, the increases originated in discrete cell sites and propagated as a wave. 23
It has been described that K201 prolongs the atrial action potential duration 24 and shorten the ventricular action potential duration in guinea pigs. 25 In dogs, K201 has reported QT prolongation without occurrence of TdP. 26 K201 also inhibited clofilium-induced TdP with an α1-agonist in rabbit. 7,27 In other studies in dogs, K201 neither suppressed nor prevented dofetilide-induced TdP at chronic atrioventricular block at the higher dose.28 Analysis of the QT and QTc intervals are critical and important for VA and TdP. However, in the present study, the QT interval could not be measured accurately because of tachycardia and atrioventricular block.
Currently, K201-suppressed initiation of atrial fibrillation 24,28–30 is being developed for the treatment of atrial fibrillation in humans. Abnormalities in intracellular Ca2+ handling may be crucial in the initiation of focal activity by atrial fibrillation and in its perpetuation by rapidly firing foci and re-entry. 31 Thus, K201 may regulate Ca2+ homeostasis in cardiac cells and play an important role in intracellular Ca2+ handling, which is delicate and complex. As the clinical applicability of the model of this study, K201 may be useful for the patient receiving the catecholamine or reperfusion treatment in order to prevent VA.
Conclusion
Isoproterenol caused fatal VA under Ca2+ loading in rats in vivo. This arrhythmia model may be appropriate for studying acquired VA. K201 gave significant protection against the occurrence of isoproterenol-induced VA and reperfusion-induced VF, whereas diltiazem suppressed reperfusion-induced VF but not isoproterenol-induced VA. The effects of K201 may occur through stabilization of RyR2 (ie, an intracellular Ca2+ blocking action) and inhibition of Ca2+ release from the sarcoplasmic reticulum via PKA, in addition to its function as a multichannel blocker. The results of this study are of interest, since the clinical goals of the use of antiarrhythmic drugs are to reduce the proarrhythmic potential and improve cardiac function. Drugs with a different mechanism to that of the conventional antiarrhythmic drugs may also be able to prevent or suppress triggered arrhythmia.
Footnotes
Acknowledgment
We are very grateful for the assistance of Makoto Shinozaki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article