
Abstract
Mildronate, an inhibitor of
Introduction
The present study was undertaken to delineate the importance of mildronate-induced changes in
Materials and Methods
Materials
Mildronate (3-[2,2,2-trimethylhydrazinium] propionate dihydrate) was obtained from JSC Grindeks (Riga, Latvia).
Animals and Treatments
A total of 75 male Wistar rats weighing 200 to 240 g were obtained from the Laboratory of Experimental Animals, Riga Stradins University (Riga, Latvia) and housed under standard conditions (21-23°C, 12-hour light/dark cycle, relative humidity 45%-65%) with unlimited access to food (R3 diet, Lactamin AB, Kimstad, Sweden) and water. Rats were adapted to these conditions for 2 weeks prior to the treatment.
Animals were randomly separated into 3 experimental groups and given daily oral doses of water (control rats, n = 29), 100 mg/kg mildronate (n = 25) or a combination of mildronate and
The experimental procedures were carried out in accordance with the guidelines of the European Community and local laws and policies, and the procedures were approved by the Latvian Animal Protection Ethical Committee of the Food and Veterinary Service, Riga, Latvia. All experiments were performed in a blinded manner.
Ten animals from each group were used for the isolated heart infarction study. Another 5 animals from each group were sacrificed at the end of the 14-day treatment, and aliquots of heart tissues of these animals were frozen in liquid nitrogen and stored at −80°C for analysis (lipid profile, glycogen concentration, and concentrations of carnitine, GBB, and mildronate) at a later time. Additional aliquots of the same tissues were immediately used for the isolation of mitochondria for the determination of CPT-I and CrAT activity. Another 6 animals from each group were used for the isolation of mitochondria for the determination of mitochondrial respiration. Another 4 animals from the control and mildronate-treated groups were used to determine the ischemia-induced respiration stimulation by exogenous cytochrome c in saponin-permeabilized cardiac left ventricular fibers isolated from ischemic hearts.
Determination of l -Carnitine, GBB, and Mildronate Concentrations
Determination of
Isolated Rat Heart Infarction Study and Hemodynamic Measurements
The infarction study was performed according to the Langendorff technique as described previously. 7 In brief, rats were anesthetized with sodium pentobarbital (60 mg/kg intraperitoneally [ip]), and heparin (1 IU/g) was administered concomitantly. Hearts were excised and retrogradely perfused with oxygenated Krebs-Henseleit buffer, via the aorta at a constant pressure of 60 mm Hg. Water–ethanol mixture (1:1)-filled balloon (polyethylene wrapping film) connected to a physiological pressure transducer (ADInstruments, Chalgrove, UK) was inserted into the left ventricle, and the baseline end-diastolic pressure was set at 5 to 10 mm Hg. Heart rate (HR), left-ventricle developed pressure (LVDP), contractility, and relaxation were recorded continuously using PowerLab8/30 system from ADInstruments. Coronary flow was measured using an ultrasound flow detector system connected to PowerLab8/30. A 4-0 coated, braided silk suture (Sofsilk; Syneture, Dublin, Ireland) was passed under the left anterior descending coronary artery (LAD) and threaded through a small plastic tube to permit reversible occlusion of the coronary artery. Hearts were adapted for 20 minutes and occlusion was performed for 60 minutes by constricting threads through a plastic tube. Successful occlusion was confirmed by a decrease in coronary flow of about 40%. 9,15 Reperfusion was achieved by releasing the threads. At the end of the 150-minute reperfusion, the LAD was reoccluded and the nonrisk zone was stained with 0.1% methylene blue solution in Krebs-Henseleit buffer infused via the aortic root. Hearts were sectioned transversely from the apex to the base into 4 slices of 2-mm thickness and incubated in 1% triphenyl-tetrazolium chloride in phosphate buffer (pH 7.4, 37°C) for 10 minutes to stain viable tissue red and necrotic tissue white. Computerized planemetric analysis of the photographs of left-ventricle slices was performed using Image-Pro Plus v6.3 software to determine the area at risk (AR) and area of necrosis (AN), each expressed as a percentage of the left ventricle area. Obtained values were then used to calculate the infarct size (IS) as a percentage of the risk area, according to the formula IS = AN/AR × 100%.
Determination of Lipid Profile and Heart Glycogen Concentration
The concentration of FAs (free FA and acyl-coenzyme A) and triglycerides in the heart tissue was determined using commercially available enzymatic kits from Wako (Neuss, Germany) and Instrumentation Laboratory (Lexington, Massachusetts) as previously described, with the exception that heart tissues were homogenized twice for 25 seconds. 16 Glycogen concentration in heart tissues was determined as previously described. 17 Glucose concentration was determined using a glucose determination kit from Instrumentation Laboratory. Absorption measurements were carried out using a µQuant Microplate Spectrophotometer (BioTek, Bad Friedrichshall, Germany).
Quantitative Reverse Transcriptase–Polymerase Chain Reaction Analysis of CPT-IA and CPT-IB Transcripts and Determination of Enzyme Activity
Quantitative reverse transcriptase–polymerase chain reaction (RT-PCR) analysis of CPT-IA and CPT-IB was performed as described previously.
6
Activities of CPT-I and CrAT were measured by isolation of mitochondria from heart tissues using a method adapted from Wilcke et al.
18
The heavy mitochondrial fraction was used for the experiment. The CPT-I activity was measured as previously described
14
in the presence of

Effects of 14-day treatment with mildronate (100 mg/kg; M 100) or mildronate and
Respiration Measurements
Mitochondrial respiration was measured at 37°C using Clark-type electrode (Microelectrodes Inc, Bedford, New Hampshire) as previously described,
20
with some modifications as indicated below. In brief, tissues were homogenized for 25 seconds in the medium (10 mL/g tissue) containing 180 mmol/L potassium chloride (KCl), 10 mmol/L Tris-HCl, and 1 mmol/L EGTA, and pH 7.7 at 4°C. The homogenate was centrifuged for 5 minutes at 750g and then the supernatant was centrifuged again for 10 minutes at 6800g to obtain the mitochondrial pellet. The final mitochondrial pellet was resuspended in the buffer containing 180 mmol/L KCl, 20 mmol/L Tris-HCl, and pH 7.2 at 4°C. Palmitoyl-coenzyme A (40 μmol/L) and corresponding
In order to evaluate the integrity of OMM, rat hearts (n = 4 per group) were isolated and perfused according to the Langendorff technique as described above. The only difference was that the hearts were adapted for 20 minutes and then subjected to 60 minutes of regional ischemia without the reperfusion period (nonischemic hearts [normal] were isolated and adapted for 20 minutes). Immediately after that the bundles of cardiac fibers were isolated from left ventricular ischemic area (from left ventricle tissues in case of nonischemic [normal] hearts) and were further prepared as described previously. 13 Briefly, bundles of fibers were permeabilized with 50 μg/mL saponin at 4°C for 30 minutes in buffer A (20 mmol/L imidazole, 0.5 mmol/L dithiothreitol, 20 mmol/L taurine, 7.1 mmol/L MgCl2, 50 mmol/L MES, 5 mmol/L ATP, 15 mmol/L phosphocreatine, 2.62 mmol/L CaK2EGTA, 7.38 mmol/L K2EGTA, pH 7.0 at 0°C). The fibers were washed twice for 10 minutes in buffer B (20 mmol/L imidazole, 0.5 mmol/L dithiothreitol, 20 mmol/L taurine, 1.61 mmol/L MgCl2, 100 mmol/L MES, 3 mmol/L KH2PO4, 2.95 mmol/L CaK2EGTA, 7.05 mmol/L K2EGTA, and pH 7.1 at 37°C). Oxygen uptake rates of permeabilized cardiac fibers were determined at 37°C with Clark-type electrode in buffer B containing respiratory substrates (6 mmol/L pyruvate/6 mmol/L malate or 10 mmol/L succinate) and 2 mg/mL BSA. To assess the integrity of OMM, 30 μmol/L cytochrome c was added after addition of 1 mmol/L ADP and the VADP+Cyt c/VADP ratio was calculated.
Statistical Analysis
All data are expressed as the mean ± standard error of the mean (SEM). For statistical analyses, the 1-way analysis of variance (ANOVA) followed by Newman-Keuls multiple comparison test or Student t test were used. To test the hemodynamic parameters before, during, and after occlusion, the repeated measures ANOVA followed by Tukey test was used. P values less than .05 were considered statistically significant. Statistical calculations were performed using Prism 3.0 software (GraphPad, San Diego, California).
Results
Concentrations of l -Carnitine, GBB, and Mildronate
After treatment with mildronate, the

Effects of 14-day treatment with mildronate (100 mg/kg; M 100) or mildronate and
Effects of Drug Treatment on Nonfasted Rat Tissue and Blood Plasma Parameters a

Abbreviations: FAs, fatty acids; SEM, standard error of the mean; CrAT, carnitine acetyltransferase; GBB, γ-butyrobetaine; M, mildronate; C + M,
aEffects of 14-day treatment with mildronate (100 mg/kg; M 100) or mildronate and
bIndicates significant difference from the control group.
As shown in Table 1 mildronate treatment significantly decreased the concentration of
Enzyme Activity, Mitochondrial Respiration Measurements, and RT-PCR Analysis of CPT-IA and CPT-IB
The activity of CPT-I was significantly decreased by 26% in the mildronate group when compared to control (Figure 2A). After treatment with mildronate, the mitochondrial respiration on palmitoyl-coenzyme A was significantly decreased by ∼27% (Figure 2B). Treatment with mildronate did not have any significant impact on mitochondrial respiration on pyruvate/malate when compared to control (data not shown). The activity of CrAT was similar in all groups (Table 1).
The cytochrome c effect was significantly higher in the left ventricular fibers isolated from ischemic hearts. Mildronate treatment significantly diminished the ischemia-induced respiration stimulation by exogenous cytochrome c when both pyruvate/malate and succinate were used as respiratory substrates (Figure 3).

The effect of cytochrome c on respiration of saponin-permeabilized cardiac ventricular fibers isolated from normoxic or ischemic hearts from control or mildronate treated (100 mg/kg, 14 days, M 100) animals. Values are represented as mean ± standard error of the mean (SEM) of 4 animals. #Indicates significant difference from the respective ischemic control group. *Indicates significant difference from the respective normal (nonischemic) control group.
No significant differences were observed in the mRNA levels of CPT-IA and CPT-IB in any of the treated groups when compared to control (data not shown).
Cardioprotective Effects During Isolated Rat Heart Infarction
The anti-infarction effect of mildronate was investigated in an isolated rat heart infarction model. Values for the AR were similar in hearts of all experimental groups, and the AR in all groups was about 40% of the area of the left ventricle (Figure 4A). Mildronate significantly reduced IS by 38% as compared to the control group (Figure 4B). In contrary, mildronate and

Effects of 14-day treatment with mildronate (100 mg/kg; M 100) or mildronate and
Hemodynamic Parameters
Results of the hemodynamic measurements are shown in Table 2. No significant differences were observed in the basal HR, LVDP, coronary flow, contractility/relaxation (dP/dt maximum and minimum), or the cardiac workload (HR × LVDP) in any of the treatment groups when compared to the control group. Similarly, no significant differences in hemodynamic parameters were observed during the occlusion procedure as compared to the control group. Meanwhile, during the occlusion procedure, coronary flow was decreased by an average of 39%, LVDP was decreased by an average of 33%, and cardiac workload (HR × LVDP) was decreased by an average of 36% for all experimental groups as compared to the values observed prior to occlusion.
Effects of Drug Treatment on Isolated Heart Parameters a
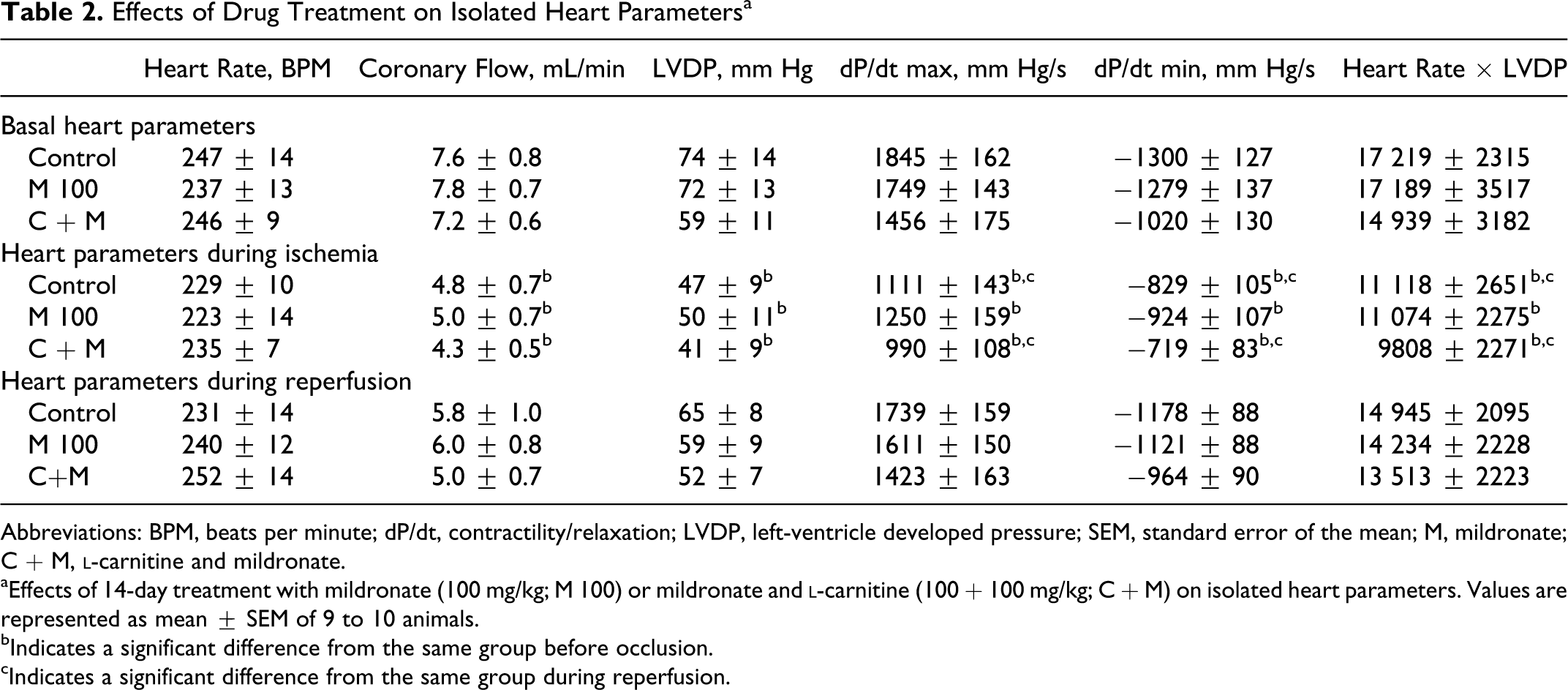
Abbreviations: BPM, beats per minute; dP/dt, contractility/relaxation; LVDP, left-ventricle developed pressure; SEM, standard error of the mean; M, mildronate; C + M,
aEffects of 14-day treatment with mildronate (100 mg/kg; M 100) or mildronate and
bIndicates a significant difference from the same group before occlusion.
cIndicates a significant difference from the same group during reperfusion.
In the reperfusion stage, the coronary flow recovered to 70% to 75% and the other hemodynamic parameters recovered to about 90% of their basal levels, but no significant differences were observed between the treated groups and the control.
Lipid Profile, Glucose Concentration, and Glycogen Concentration
The glycogen, FAs, and triglyceride concentrations in the heart tissues of nonfasted rats are shown in Table 1. No significant differences were observed in the tissue lipid profiles or glycogen concentration values for any of the treated groups when compared to the control group.
Discussion
The results of the present study, performed in an isolated rat heart ischemia–reperfusion injury model, provide evidence that the pivotal factor for the development of the anti-infarction activity of mildronate in heart tissue is a decreased
Mildronate treatment significantly diminished the ischemia-induced respiration stimulation by exogenous cytochrome c (Figure 3). These results indicate that the cardioprotective effect of mildronate could be attributed to the maintenance of the intactness of OMM which is expected to protect against ischemia-impaired ATP synthesis 22,23 and improve the survival prognosis of myocardium. The results of the present study (Figure 3) point to the maintained functionality of OMM as a possible mechanism behind the preserved ATP levels in mildronate-treated rat hearts in ischemia-related conditions reported in previous studies. 24,25
Treatment with mildronate alone or with the combination of mildronate and
Long-term treatment with mildronate induces preconditioning-like effects by causing changes in FA and glucose metabolism-related gene expression. Thus, treatment with mildronate at doses of 200 mg/kg6 and 800 mg/kg
27,28
induces a compensatory increase in CPT-I protein and mRNA expression as well as an increase in maximal CPT-I enzyme activity. Similarly, increased expression of glucose metabolism-related genes has been observed in heart tissue.
6
In the present study, due to the use of a lower dose of mildronate (100 mg/kg), we did not observe significant changes in mRNA expression of CPT-I. Activity of CPT-I in heart tissue was significantly reduced by 26% and mitochondrial respiration on palmitoyl-coenzyme A was significantly reduced by 27%, as measured in the presence of 200 μmol/L
Mildronate concentrations in the hearts of the mildronate-only treated rats were about 3 times higher than those in the hearts of rats treated with a combination of mildronate and
It is well documented that decrease in FA oxidation and increase in glucose oxidation are associated with protection and improvement in the functional recovery of the heart during ischemia–reperfusion.29,30 Biochemical consequences of decreased
In conclusion, the decrease in
Footnotes
The work reported was done at the Latvian Institute of Organic Synthesis.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The European Social Foundation agreement No. 2009/0147/1DP/1.1.2.1.2/09/IPIA/VIAA/009; The European Regional Development Fund grant No. 2DP/2.1.1.1.0/10/APIA/VIAA/063; the Latvian State Research Program grant No. 2010.10-4/VPP-4.