
Abstract
Disorders of the brain and its sensory organs have traditionally been associated with deficits in movement, perception, cognition, emotion, and behavior. It is increasingly evident, however, that positive phenomena may also occur in such conditions, with implications for the individual, science, medicine, and for society. This article provides a selective review of such positive phenomena – enhanced function after brain lesions, better-than-normal performance in people with sensory loss, creativity associated with neurological disease, and enhanced performance associated with aging. We propose that, akin to the well-established field of positive psychology and the emerging field of positive clinical psychology, the nascent fields of positive neurology and positive neuropsychology offer new avenues to understand brain-behavior relationships, with both theoretical and therapeutic implications.
The traditional view of nervous system function postulates that a lesion to the brain will usually lead to a loss of function, that a second lesion will inevitably exacerbate the effects of the first lesion, that sensory loss will generally lead to impairment, and that aging is always associated with functional deficits. These assumptions, however, appear in some cases to be incorrect, with implications for our understanding of brain-behavior relations and also for therapeutic endeavors in clinical settings.
The study of individuals with cerebral pathology has traditionally been embedded in the lesion-deficit model. Although this framework has provided valuable insights into our understanding of the organization of function in the human brain, it has its drawbacks. By focusing on the negative effects of changes, the lesion-deficit model can overlook positive changes, such as plasticity-related phenomena. It can also introduce potential confounds since it can sometimes be problematical to make a direct link between a behavioral deficit and the locus of a lesion or disease state because of other nonspecific or distant effects of the lesion. Last, it may discourage thinking about the compensatory and adaptive strategies that the brain, and the person, could use and which assist in coping with disease and restoring function.
In this article, we explore examples that question the traditional view that lesion or dysfunction of the nervous system inevitably leads only to deficits in performance. Not only are these examples important clinically, but they also have scientific relevance. Science usually advances steadily, by convergence, and is wary of maverick theories that often capture attention. However, paradoxical phenomena that are outside prevailing models can occasionally illuminate underlying processes, and paradoxical behavior even appears to operate at a basic biological level such as molecules within cell circuits (Hart and others 2012). Thinking about exceptions may provide insights into how the brain functions, and also into how people who experience neurological difficulties may best be helped.
We do not challenge that, for most people, neurological impairment reduces their possibilities within the world and frequently requires them to relearn functions and actions that previously occurred automatically. But we do suggest that these losses are not always the only outcomes of nervous system insults. Such ideas are not new. “Neurology’s favourite word is deficit, denoting an impairment or incapacity of neurological function,” noted Oliver Sacks (1985, p. 1). Ten years later, in An Anthropologist on Mars, he wrote, “Defects, disorders, diseases, in this sense, can play a paradoxical role, by bringing out latent powers, developments, evolutions, forms of life, that might never be seen, or even be imaginable, in their absence” (Sacks 1995, p. xii). As early as 1929, Vygotsky made a similar point in “The Fundamental Problems of Defectology,” commenting on the importance of compensatory strategies and mechanisms in cases such as blindness (Vygotsky and others 1929/1993). Vygotsky noted,
The doctrine of overcompensation has an important significance and serves as a psychological basis for the theory and practice of educating a child with a loss of hearing, sight, and so forth. What horizons will open up to the pedagogue, when he recognizes that a defect is not only a minus, a deficit, or a weakness but also a plus, a source of strength and that it has some positive implications! (Vygotsky and others 1929/1993, p. 29)
Recently, a number of studies have challenged the standard lesion-deficit model. There may be limited correspondence between lesion and dysfunction or disability (Rovaris and Filippi 2005; Savva and others 2009; Strasser-Fuchs and others 2008), whereas in some instances lesions may be clinically “silent” for years (Hakiki and others 2008; Krampla and others 2008; Kuratsu and others 2000). Kapur’s (1996) article on paradoxical functional facilitation helped outline a new framework with which to view brain-behavior relationships. In developmental neuropsychology, there has also been a greater recognition of the occurrence of enhanced function in conditions such as autism (Frith and Happé 2009) and dyslexia (Schneps and others 2012; von Károlyi and others 2003).
The field of positive psychology is now well established (Baumgardner and Crothers 2009), with journals, organizations and government reports devoted to the topic. This movement emphasizes the role of dispositional optimism, the neural mechanisms of flourishing, and the importance of resilience and functional reserve in coping with impairment (Seligman 1999; Seligman and Csikszentmihalyi 2000). In parallel, the field of positive clinical psychology has recently begun to emerge as a distinct entity (Joseph and Wood 2010; Tarrier 2010; Wood and Tarrier 2010), which advocates a focus on the positive in traits and experiences and incorporates these as part of the assessment and treatment process in a therapeutic setting.
The focus of this article is somewhat different from most papers in clinical neuroscience—our focus is on the extent to which various brain conditions, of themselves and independent of resilience or optimism, enable and uncover enhancement, and how this enhancement may reveal brain mechanisms and opportunities for rehabilitation. As was implicit in Hughlings Jackson’s theory of recovery of function (York and Steinberg 1995), when confronted with a lesion or illness, the brain responds by adapting in a highly plastic fashion, and thus the various observable consequences are the manifestations of how the rest of the brain copes with the insults. As such, the consequences can be deleterious, beneficial, or show no clinical consequences at all—a “silent” lesion. Whereas traditionally only the first and last of these consequences have been discussed, we will focus on the second outcome.
To our knowledge, the term positive neurology has only been briefly used on a couple of occasions (Chatterjee 2004; Eide and Eide 2006), and the term positive neuropsychology only in a couple of conference presentations (Arnett 2011; Eslinger 2005). This review is intended to help set a foundation for the fields of positive neurology and positive neuropsychology and to illustrate how such a foundation may have significant theoretical and therapeutic implications.
Enhancement of Function after Brain Lesions
In neurological conditions, paradoxical enhancements of function generally take one of three forms; enhanced performance compared with neurologically intact individuals (“lesion facilitation”), alleviation or restoration to normal following a second brain lesion (“double-hit recovery”), and direct or indirect benefit for long-term neurological outcome after specific cognitive deficits (“paradoxical positive outcome”).
Enhanced Cognitive Performance in Neurological Patients (“Lesion Facilitation”)
Better-than-normal performance in neurological patients compared to healthy controls has been noted in perceptual performance (Fig. 1) in those with visual object agnosia (Moscovitch and others 1997), visual search in patients with semantic dementia (Viskontas and others 2011) and detection of deception from facial cues in those with aphasia (Etcoff and others 2000).
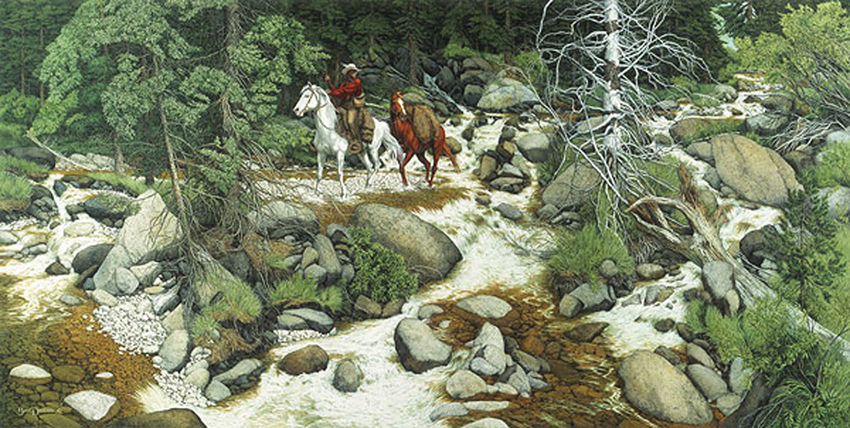
The “Faces in the Forest” by Beverely Doolittle. The faces are composed of rocks, trees, and streams. The patient in the study by Moscovitch and others (1997) was better able to detect the faces than healthy controls. © Beverly Dolittle, licensed by The Greenwich Workshop, Inc. Reproduced by permission.
In the case of amnesic patients, unlike healthy controls, they are less likely to extrapolate beyond the view in scenes and consequently make fewer boundary extension errors (Figures 2 and 3) in their recall of visual scenes and tactile arrays (Mullally and others 2012).
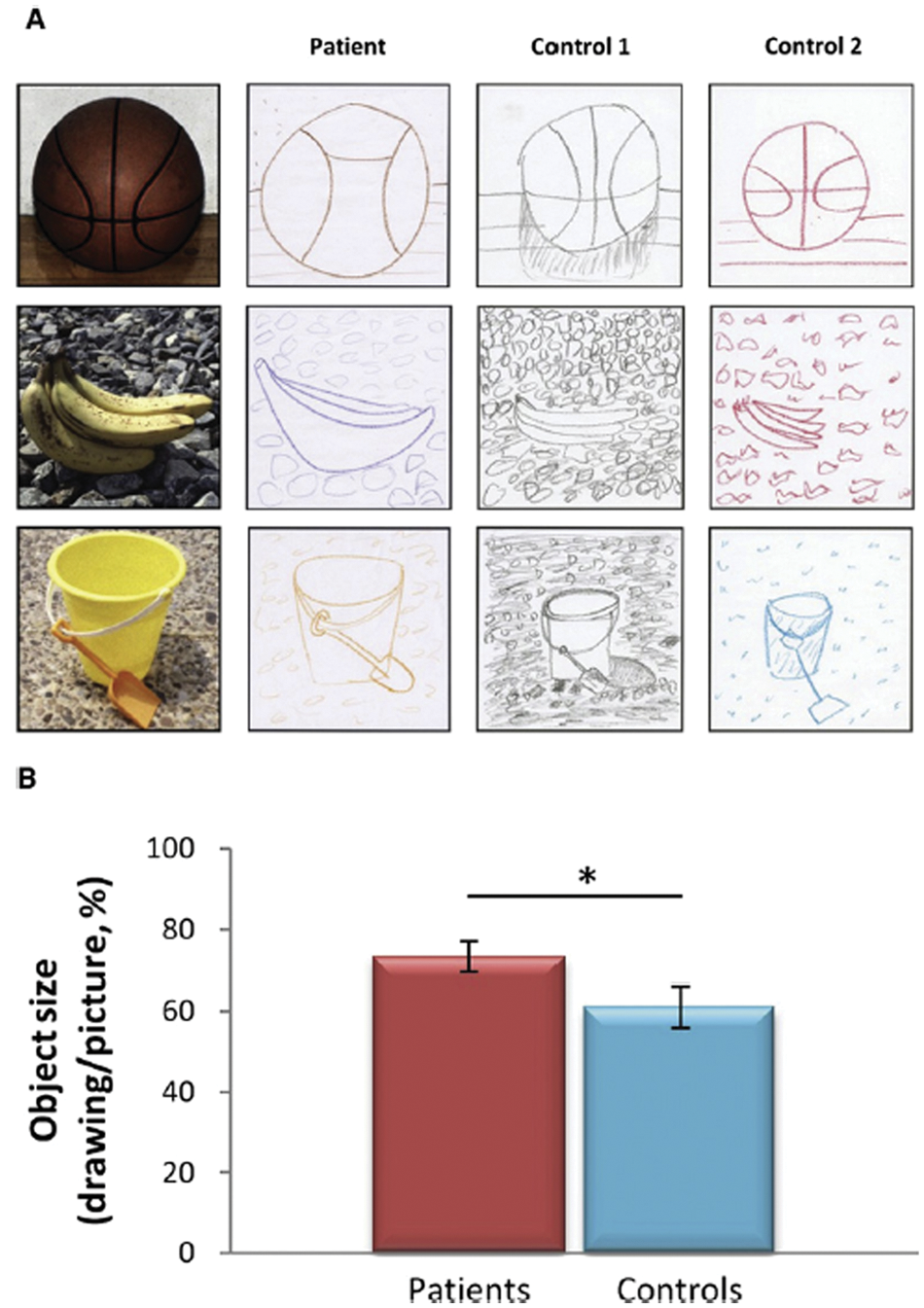
Boundary extension drawing task. (A) The left panel displays the three scene stimuli. Each scene photograph was surrounded by a 6 × 6 inch black border and was studied for 15 seconds and immediately drawn from memory in a 6 × 6 inch response square. Example drawings by a patient and her two matched control participants are displayed in the middle and left panels. In both control participants’ drawings, more background is clearly depicted than was present in the original stimuli. This represents greater boundary extension and was quantified in terms of a percentage area decrease in object size (calculated by tracing along the outer borders of the objects using Adobe Photoshop CS4 and measuring the area in pixels) in the remembered relative to the original object size. (B) Overall, patients showed significantly less boundary extension than control participants. *P < .05. From Mullally and others (2012). © 2012 Current Biology Elsevier. Reproduced by permission.
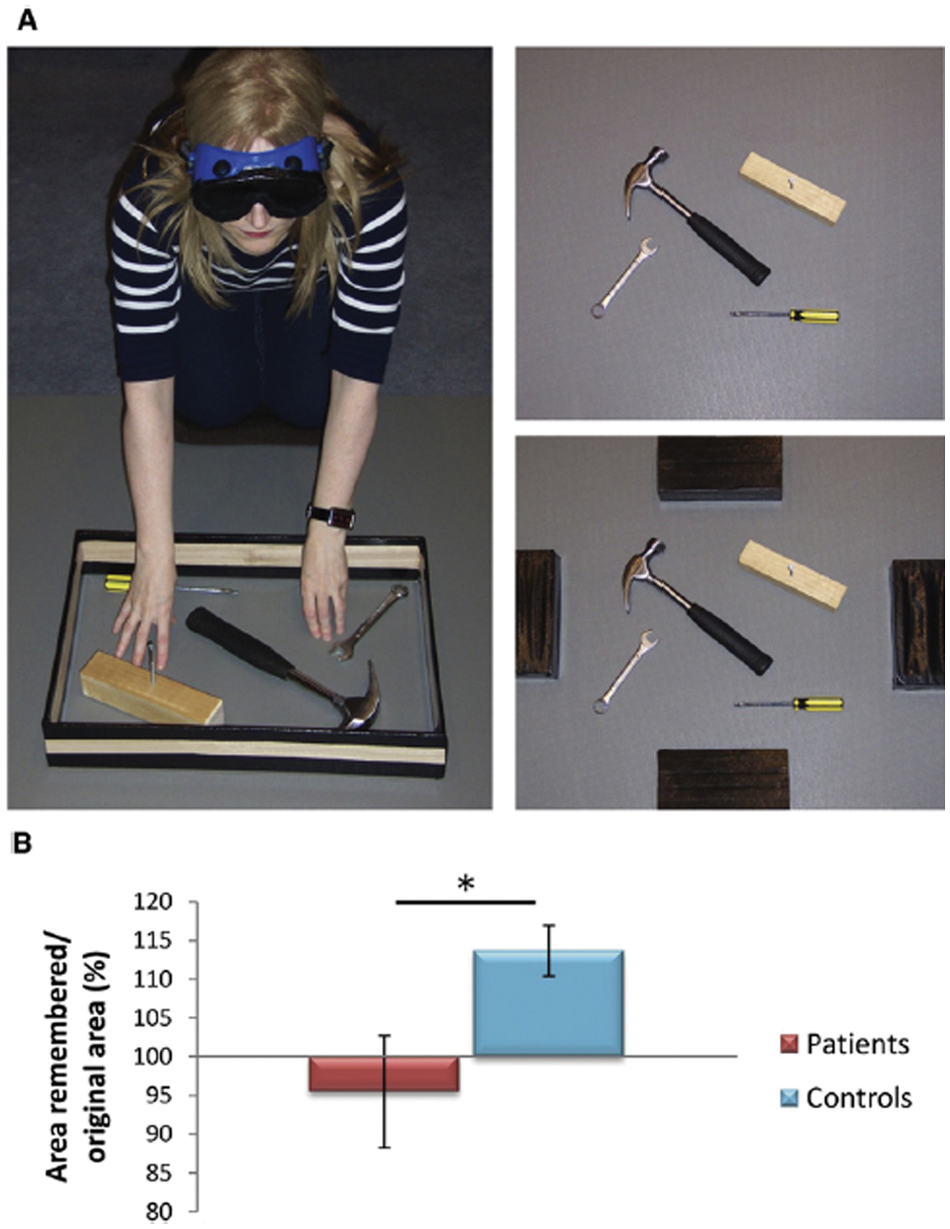
Haptic boundary extension task. (A) Participants explored three distinct scenes, each presented within a wooden border (left panel), for 30 seconds using touch alone. The border was then removed (upper right panel) and participants (still blindfolded) were asked to indicate the original location of each border using large markers (right lower panel). (B) Boundary extension was defined in terms of an increase in the reconstructed scene area relative to the original scene’s size. Compared with the control group, patients showed significantly less boundary extension. *P < .05. From Mullally and others (2012). © 2012 Current Biology Elsevier. Reproduced by permission.
In addition, a reduced susceptibility to make false positive responses to associates of target items (“lures”) has been noted in patients with amnesia (Schacter 1996) and those with Alzheimer’s disease (Hudon and others 2006). In a learning task where it pays to forget irrelevant associations from earlier trials, patients with amnesia may indeed do this and thus perform better than controls (Myers and others 2003). Where explicit and implicit memory mechanisms compete, and implicit mechanisms underpin correct responses, then having impaired explicit memory—as in the case of amnesia—may result in better-than-normal performance (Cermak and others 1997; Musen and others 1990). Enhanced performance in problem-solving tasks has also been reported in a few studies of patients with frontal lobe lesions (Reverberi and others 2005) and more successful risk-taking behavior in patients with lesions of the amygdala or orbitofrontal cortex (Shiv and others 2005).
Where a Second Brain Lesion Helps (“Double-Hit Recovery”)
In films and cartoons (see Baxendale 2004), it is not uncommon for somebody to become densely amnesic following a bang to the head, only to recover miraculously after a second bump. Although this effect is fictional, there are a few well-documented cases where a subsequent lesion may ameliorate deficits caused by the first.
In cats, Sprague (1966) produced inattention to the left side of space, “left-sided visual neglect,” following ablation of the right posterior neocortex. When this lesion was followed by another, this time to the left superior colliculus, much of this neglect and related visual deficits disappeared. Subsequent studies (summarized in Sprague 1996 and in Ogourtsova and others 2010) have confirmed the effect and have also extended it to the field of auditory function (Lomber and others 2007).
Weddell (2004) reported the first clinical case study documenting a human analogue of the Sprague effect. A patient with a midbrain tumor developed left-sided neglect as the result of subsequent right frontal damage. When the midbrain tumor progressed to involve the left superior colliculus, bilateral visual orientation returned (though subsequent right-sided visual neglect developed after further progression of the tumor, with probable additional damage to the right superior colliculus). Vuilleumier and others (1996) found that left-sided neglect following a right parietal infarct disappeared after subsequent left frontal infarction. Related to this observation are studies that have employed left hemisphere transcranial magnetic stimulation to alleviate left-sided neglect (Lim and others 2010; Shindo and others 2006).
In the field of movement disorders, a second lesion superimposed on existing pathology may restore a degree of balance to a system and thus result in alleviation of motor symptoms. For example, Probst-Cousin and others (2003) and Choi and others (2008) have reported that thalamic stroke can lead to the alleviation of tremor caused by Parkinson’s disease.
Paradoxical Positive Outcomes in Neurological Disorders
Traumatic brain injury (TBI) generally results in impaired functioning in cognition, emotion, and behavior. The traumatic event itself can often have negative connotations and, in some patients, posttraumatic stress disorder (PTSD) is a major residual disability. PTSD involves intrusive thoughts related to the event, including nightmares, distress on exposure to trauma-related cues, anxiety and avoidance behavior, and general cognitive and somatic symptoms associated with hyperarousal. In TBI, especially following blunt head injury with concussion, there is usually amnesia for the event. Drawing on earlier clinical observations (Adler 1943; O’Brien 1993), several studies have reported that some patients with TBI have a lower incidence of PTSD. Gil and others (2005) reported that the less patients recalled of the event associated with their head injury, the less they developed PTSD. Subsequently, Bryant and others (2009) noted that longer periods of posttraumatic amnesia seemed to protect against the occurrence of severe intrusive memories. Other studies have, however, not found such a protective effect (e.g., Greenspan and others 2006). Harvey and others (2003) have noted that some of these differences may in part be related to ambiguity in the criteria for diagnosing PTSD and that TBI patients may perhaps have PTSD symptoms, but that the symptoms differ in content from that of other PTSD patients.
Although insight and an accurate awareness of one’s deficit in TBI are important for a good outcome, a few anomalies in this relationship have been noted. Thus, Herbert and Powell (1989) reported that clients with TBI who over-rated their abilities did better following rehabilitation than clients who were more realistic or underconfident (though see Malia and others 1993). More recently, Cooper-Evans and others (2008) noted that those with TBI who were more impaired cognitively and/or less aware of their deficits reported higher-self esteem than other TBI survivors. Recently, there has also been an increased focus on positive changes seen in some who survive a brain injury or brain illness—“posttraumatic growth.” Such observations in neurological conditions are surprising given the generally negative expectations after an insult to the brain. Both McGrath and Linley (2006) and Powell and others (2007) noted that in a group with TBI, posttraumatic growth appeared to increase with time. Hawley and Joseph (2008) followed up cases for an average of 11 years after TBI and found that around half of their participants showed evidence of posttraumatic growth on a structured questionnaire, responding positively to items such as—“I value my relationships much more now.”
Researchers who have investigated people’s experience of locked-in-syndrome have found a significant number who maintain a good quality of life and one which is often in the same range as age-matched healthy individuals (Lulé and others 2009). In that study, depression was not predicted by physical state; rather, having a successful psychological adjustment to the disease was related to problem-oriented coping strategies, like seeking information, and emotional coping strategies. The strongest predictor of psychosocial adjustment was, in turn, perceived social support. Interestingly, Lulé and others (2009) also found evidence that significant others, like primary caregivers or spouses, rated locked-in-syndrome patients’ quality of life significantly lower than the patients themselves rated their quality of life.
These examples echo the work of the German neurologist Kurt Goldstein, based on his observations on soldiers with brain injury after World War I (Goldstein 1935/1995). He described how some people have a capacity to actively adapt and adjust to catastrophic losses. He suggested that this involved, among other things, withdrawal to a more limited range of functioning and expectations, which could, in turn, be managed by a redistribution of reduced energies, thus reclaiming as much wholeness and “meaning” as their new circumstances allow. This often involved a transformation of identity and a willingness to accept change, to become “all that one can become.” He described how, using this mental framework, success arose through a focus on residual strengths rather than on any negative consequences of pathology. In this sense, psychological flexibility (or an ability to continually adapt one’s thinking, emotions, and behavior) has been put forward as an essential buffer throughout life’s “ups and downs” (e.g., Kashdan and Rottenberg 2010).
Enhanced Function Associated with Sensory Loss
It is hardly conceivable that losing or lacking a sensory modality would not, in some fashion, alter the capacities of processing, understanding, or interacting with the world. Therefore, if lack or loss of a sensory modality leads to a compensatory enhancement of other senses, resulting in minimal loss or even functional gains, these would represent instances of paradoxical functional facilitation. Enhancement of functioning in people with chronic or recent sensory loss has been widely studied. Individuals with visual loss have been found to show enhanced sensory performance in other domains. Similarly, long-term auditory loss has been associated with enhanced cognitive performance in tactile and visual tasks. Functional brain imaging and transcranial magnetic stimulation studies have pointed to a major reorganization of cerebral function in blind or deaf individuals, and these plastic changes are associated with functional adaptations and gains.
Loss of Vision
Individuals with visual loss have been found to show enhanced auditory function, tactile function and even verbal memory performance (Amedi and others 2003; Collignon and others 2006; Forster and others 2007; Kupers and Ptito 2011). Rosenbluth and others (2000) and, more recently, Cuevas and others (2009) found that children with early-onset or congenital blindness perform better than sighted children at labeling common odors. Beaulieu-Lefebvre and others (2011) showed that blind individuals had significantly lower odor detection thresholds than sighted individuals, and a study from the same group (Kupers and others, 2011) showed stronger blood oxygen level–dependent responses in the occipital cortex when blind participants were performing an odor detection task. Hugdahl and others (2004) found that blind subjects are better than sighted subjects at repeating spoken syllables.
Gougoux and others (2004) also reported better pitch discrimination in early-blind, but not late-blind, subjects. Along with many others, Fieger and others (2006) reported that blind individuals are also better than sighted individuals in the localization of sounds, particularly those coming from the periphery. Collignon and others (2006) reported shorter reaction times in auditory and tactile spatial attention tasks in the early blind, who also show better divided attention in tests where both tactile and auditory modalities are used. In addition, Stevens and Weaver (2005) have found that early-blind subjects have lower temporal order judgment thresholds than sighted subjects in auditory tasks. Recent evidence further suggests that enhanced auditory capabilities may facilitate faster emotional discrimination in blind individuals than controls (Klinge and others 2010).
In the case of haptic sensitivity, Van Boven and others (2000) and Goldreich and Kanics (2003) have found that early-blind subjects show enhanced tactile discrimination in a gratings orientation task. This task evaluates an individual’s tactile discrimination ability in judging fine orientation differences between objects. Blind subjects also demonstrated lower thresholds on an angle discrimination task compared with sighted subjects, providing further evidence of a heightened sensitivity to tactile inputs (Alary and others 2008). Forster and others (2007) found that the blind respond faster and are more accurate than sighted subjects in a difficult tactile spatial selection task. Röder and others (2004) noted better tactile temporal order judgments in the congenitally blind (Occelli and others 2008; Wan and others 2009). Enhanced performance by blind subjects in detecting Braille characters has been noted in a number of studies—for example, Bliss and others (2004) reported that in a tactile n-back task (in which people are asked to judge whether a current stimulus differs from that presented 1, 2, . . ., n trials previously), blind subjects outperformed their sighted counterparts. Blind individuals also show greater accuracy than sighted individuals in bimanual tactile estimations of object size with familiar objects (Smith and others 2005). Champoux and others (2011) found that blind individuals were less susceptible to the parchment-skin illusion, in which the sound generated by hands rubbing together results in a change in how dry or moist the palms feel, depending on how the original sound is altered (e.g., change in frequency). It seemed that blind individuals are better at ignoring auditory stimuli while completing a tactile task. Interestingly, enhanced tactile abilities do not appear to be limited to the fingers used for Braille; some reports have also found greater tactile discrimination ability in the tongue in blind individuals (Chebat and others 2007), though others have reported enhancement effects on the fingers but not on the lips (Wong and others 2011), suggesting that it is training experience rather than visual deprivation that may be the key factor (Voss, 2011). However, not all aspects of haptic processing are enhanced in the blind—for example, tactile spatial judgment may be comparable in performance to that of healthy individuals (Sathian and Stilla 2010).
There is also evidence for enhanced memory functioning in blind individuals. People who are blind have been reported to outperform the sighted in auditory–verbal recognition (Röder and others 2001), recall (Amedi and others 2003), and memory for the ordering of a heard list (Raz and others 2007). In all domains, however, the specifics of the task appear to determine whether functional gains will be observed (Alary and others 2009). Recent data suggest that the advantage in blind individuals stems from better stimulus encoding rather than enhancements in later stages of processing (Rokem and Ahissar 2009).
Since ancient times, people who are blind have been taught to sing, and anecdotes abound about disproportionate numbers having musical talent. Examining one aspect of musicality, the ability to precisely name a heard note (“absolute pitch”), Hamilton and others (2004) found that 57.1% of blind musicians possessed this talent. In contrast, the highest reported rates among sighted Caucasian musicians is 18%. Since all the blind musicians in the study were rendered blind by peripheral causes after birth, this heightened prevalence appears related to the consequences, rather than the causes, of sight loss. There are intriguing suggestions that the acquisition and mechanisms of absolute pitch may differ in blind musicians. First, the age of initial music exposure among the blind (average 8.45 years; range = 3-24 years) was significantly later than that among sighted, absolute pitch musicians (average = 5.06 years; range = 3-7 years). Second, in brain imaging studies, blind musicians with absolute pitch did not show the same exaggerated planum temporale asymmetry as was observed on the brain imaging in their sighted counterparts.
Valentine Haüy, known as the “father and apostle of the blind,” and many subsequent educators have argued for an enhanced ability among blind children to learn music and this ability, in addition to barriers in other professions, may account for the prevalence of piano-tuners in this community. It is worth noting, however, that the idea that blind people are obliged to learn lengthy sections of music “by ear” is wrong; Louis Braille, himself an accomplished musician, adapted his punctographic system to musical notation.
Loss of Hearing
Paradoxical phenomena have also been shown in the domain of auditory loss. Levanen and Hamdorf (2001) reported that congenitally deaf subjects show enhanced tactile sensitivity, in terms of tactile change detection, compared with controls, and Bottari and others (2010) have recently reported enhanced reactivity to visual stimuli in deaf individuals. Bavelier and others (2006) reviewed research pointing to enhancement in visual processing in the deaf. Deaf signers are better at distributing attention toward the visual periphery during certain visual perception tasks than both sighted–hearing controls and hearing signers (Bavelier and others 2000; Bosworth and Dobkins 2002; Neville and Lawson 1987; Proksch and Bavelier 2002; Rettenbach and others 1999; Stevens and Neville 2006). Further studies have shown enhancements, particularly lateralized to the right visual field, in visual motion detection thresholds in deaf signers as compared with hearing subjects (Finney and others 2003). Dye and others (2007) also reported enhancement of peripheral attention mechanisms in deaf subjects (as manifest in greater interference from peripheral flankers), and Dye and others (2009) also demonstrated enhanced visual selective attention within the peripheral visual field. In terms of mechanisms that may underlie enhanced visual function in the deaf, a recent report (Codina and others 2011) has pointed to unique retinal changes in deaf individuals that were not found in hearing subjects. In a systematic study of the effects of long-term hearing loss, and also the ability to use sign language, Cattani and others (2007) reported that experience in sign language use was a key mechanism underlying the enhancement of visual abilities found in deaf subjects. In fact, different neural substrates may support the perception of American Sign Language compared with other actions (Corina and others 2007). Additionally, Rouger and others (2007) found better lip-reading performance in deaf subjects, and also the enhanced ability to integrate visual and degraded speech cues during lip-reading. Deaf subjects demonstrate superior performance in detecting emotional expression and local facial features and discriminating between different faces (Arnold and Murray 1998; Bettger and others 1997; McCullough and Emmorey 1997) and show preserved or even enhanced ability for temporal processing and temporal order judgments (Nava and others 2008). However, as in the case of blindness, not all aspects of non-hearing sensory processing are enhanced or even maintained in deaf individuals, with impairments evident in some aspects of temporal attention (Dye and Bavelier 2010).
Creativity in Neurodegenerative Disease
Unexpectedly, new or preserved musical or visual artistic abilities have been described mainly in the setting of frontotemporal dementia, which causes progressive atrophy of frontal and anterior temporal lobes (Miller and others 1996; Miller and others 1998; Miller and others 2000), though occasionally in other settings (Schott 2012; Chakravarty 2011). Examples of such artistic productivity are shown in Figures 4 and 5.
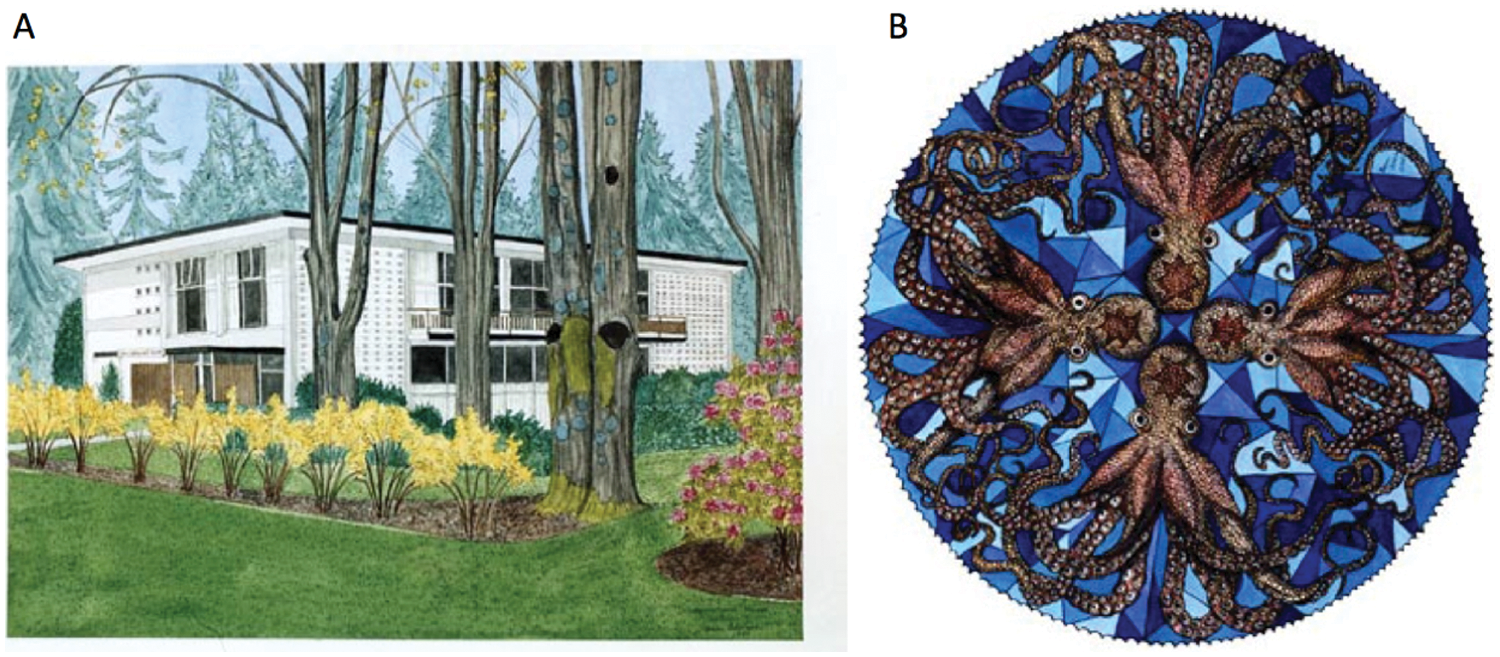
Evolution of artwork in a patient with progressive non-fluent aphasia. A was painted in 1990, whereas B was painted in 2000 and demonstrates a move away from realistic depictions and toward more abstract art. The patient began showing symptoms in the late 1990s. Reprinted with the family’s permission.

Sculpture by a patient with frontotemporal dementia, 2 years after diagnosis. This patient showed no interest in art prior to the onset of his disease and with disease progression became more and more obsessed with art creation. Reprinted with the family’s permission.
Given the putative role of the frontal lobes in creativity, it is not surprising that the emergence of these abilities is more often linked to degeneration of the anterior temporal lobe, particularly in the left hemisphere, and that artistic creativity may be at the cost of some impairments in cognition. These patients may show progressive loss of conceptual knowledge, and their creative output tends to be devoid of verbal or symbolic content (Miller and others 2000); patients paint realistic landscapes, animals, or detailed geometric designs devoid of meaning beyond the literal. Musicians continue to perform music but, even with popular songs, pay less attention to the words. One individual did not notice when the words of a famous folk song, My Bonny Lies Over the Ocean, were altered to the point of being incomprehensible during a sing-a-long (Sacks 2007). In our experience, much of the work created by these patients contains some recollections from the past; though, as mentioned above, they tend to avoid verbal or symbolic representations. Not surprisingly, then, a recent study restricted to patients with the frontal variant of frontotemporal lobar degeneration demonstrated a marked impairment on the Torrance Test of Creative Thinking in this patient group, compared with healthy controls and patients with Parkinson’s disease (de Souza and others 2010).
Despite progressive neurodegeneration, these artistic patients share many features with great creative minds from history. They can show increasing interest and/or preoccupation with their subjects, neglect social and occupational responsibilities in favour of their art, and they continue to produce work even in the absence of any encouragement or support from others (Miller and others 1998). It is likely that within their artistic context, they are able to achieve a “rewarding state of flow.” “Flow” was first defined by Mihalji Csikszentmihalyi (1991) to characterize those moments where an individual is so productively involved in an activity that he or she is almost in a meditative state and does not notice the passing of time—the individual is absorbed in and enjoys something to such an extent that he or she becomes less distractible and more effective. As suggested earlier, patients with emergence of new or preservation of old artistic skills do not show extensive frontal lobe degeneration (Miller and others 2000). This fits with a wealth of research on creativity in neurologically intact individuals, which suggests that certain components of frontal lobe function are critical (Chavez-Eakle and others 2007).
While exploring the connection between anterior temporal lobe degeneration and visual art, Rankin and colleagues (2007) used standardized tests to probe creative cognition and novel tests of visual art creation. Patients with both the frontal and temporal variants of frontotemporal dementia produced artwork that was rated as more bizarre and distorted than patients with Alzheimer’s disease and healthy age-matched controls. Notably, however, in the verbal tests of creative cognition, patients with semantic dementia (anterior temporal lobe damage) showed decreased fluency, originality, and elaboration in concert with a tendency toward ending the test prematurely. On standardized visuospatial creativity testing, which involved creating drawings based on incomplete meaningless doodles, these patients were more likely than participants from any of the other groups to produce drawings devoid of meaning, and to choose conventional or obvious markings, such as closing an open-ended figure. In contrast, their paintings, and other artwork were striking in the aesthetic dimension, characterized by the unorthodox use of vivid and unconventional colors, intricate and repetitive geometrical designs, underscoring the unique perception and also the obsessive nature of their work. One caveat when interpreting this work is that though the patients’ drawings might be hailed as more creative by the artistic community, the brain networks underlying this may not be the same as that used by healthy artists; it is one thing to be able to represent an object realistically and then steer away from this for artistic effect, quite another to be no longer able to hold accurate representations. The enhancements in creativity with a particular degenerative pattern may also be domain specific. Skills in one domain, for example, music, may improve creative output in that domain but not necessarily transfer to other artistic realms, so too might the paradoxical facilitation of creativity with neurological disease remain tied to a single output.
The dominance of the visual, and the perseverative or obsessive behaviors characteristic of semantic dementia, is reflected in the large proportion (~25%) of these patients for whom jigsaw puzzles become important, or even the primary activity of daily living (Green and Patterson 2009), suggesting they are able to achieve “flow” during working on these puzzles. In a controlled study, Green and Patterson (2009) found that semantic dementia patients have above average jigsaw skills, especially in “reality-disrupted” puzzles, in which expectations of the real world can interfere with puzzle completion, and in “grain” jigsaw puzzles, characterized by the fact that conceptual knowledge does not benefit performance. Encouragingly, from a clinical standpoint, semantic dementia patients, who often exhibit flat affect and demeanor in social situations, displayed pleasure and pride during the completion of jigsaw puzzles suggesting that this might be a good candidate for enabling flow in many patients with semantic dementia.
In a comprehensive case study, Seeley and others (2008) described a visual artist, Anne Adams, with progressive non-fluent aphasia (PNFA). Though she had painted as a hobby throughout her life, with disease progression painting became progressively more important, until it became her primary daily activity. Note that she might have chosen any number of hobbies that were less complex, or related to her profession (she was a biologist), and yet she, and other similar patients, chose visual art. Likewise, another semantic dementia patient who was a lawyer by profession and a musician by avocation also chose to produce visual art when he became ill, rather than resorting to music or other hobbies (Miller and others 1998). Anne’s most stunning works were produced at a time when the disease was already progressing. In PNFA, the main site of atrophy is the left fronto-opercular cortex, leaving patients with effortful, non-fluent, and apractic speech (Gorno-Tempini and others 2004), together with difficulties with grammar and articulation. In an interesting twist of fate, Anne created an elaborate painting inspired by Maurice Ravel’s (1875–1937) famous “Bolero” (Seeley and others 2008). Ravel himself suffered from a progressive aphasia, and composed this, set to the rhythms of the Moorish-Spanish dance, in the early stages of his disease, at age 53. The piece is a study of compulsions and perseverations (Amaducci and others 2002), with the repetition of a simple melodic theme, accompanied by an extraordinarily repetitive and simple bass line. Interestingly, Ravel considered the Bolero as a rather trivial work, describing it once as “a piece for orchestra without music.” “I’m going to try and repeat [the theme] a number of times without any development, gradually increasing the orchestra as best I can” (Orenstein, 1991). After writing Bolero, Ravel’s illness gradually progressed until he died 8 years later, of iatrogenic complications. Unaware of Ravel’s illness, Anne Adams painted her Bolero, in a precise and compulsive fashion, with the height of each of her rows signifying the increasing texture and volume of the orchestra. Although her PNFA may have reduced social interaction, she was evidently still able to transfer descriptive content from one medium to another.
Structural and functional imaging demonstrated enhanced gray matter and activation in heteromodal associative (intraparietal sulcus/superior parietal lobule) and polymodal (superior temporal sulcus) neocortex in Anne’s right hemisphere (Seeley and others 2008). These areas are involved in visuomotor search and attentional control (Corbetta and Shulman 2002; Seeley and others 2007) and sensory transcoding, necessary for sight-reading music (Schon and others 2002; Sergent and others 1992). Voxel-based morphometry (VBM) has also demonstrated enhancement in these same regions in professional musicians (Gaser and Schlaug 2003).
Given that patients with semantic dementia seem to prefer tasks that engage their visual processing skills, such as jigsaw puzzles, gardening, playing solitaire, and other activities, Viskontas and others (2007) wondered whether they experience the visual world differently as their disease progresses. In a preliminary investigation of what aspects of the visual field draw their attention, the authors tracked eye movements in healthy age-matched controls, patients with Alzheimer’s disease, frontal variant frontotemporal dementia, as well as semantic dementia as they freely observed images of various objects, landscapes, and artwork. To interpret the eye movement data, heat-map density plots from each patient group were compared with maps from healthy control participants. There was very little overlap between where the semantic dementia patients spend their time looking and what draws the attention of healthy participants, and other patient groups. These findings suggested that these patients do indeed pay attention to aspects of the visual field that are largely ignored by healthy people.
Viskontas and others (2011) have recently completed a study of dementia patients that found enhanced visual search in patients with semantic dementia, which in turn correlated with greater grey matter in the right superior parietal lobe in both patients and controls when measured with VBM (Figures 6 and 7). That is to say, the more grey matter found in this region, the better the performance in conjunction search.
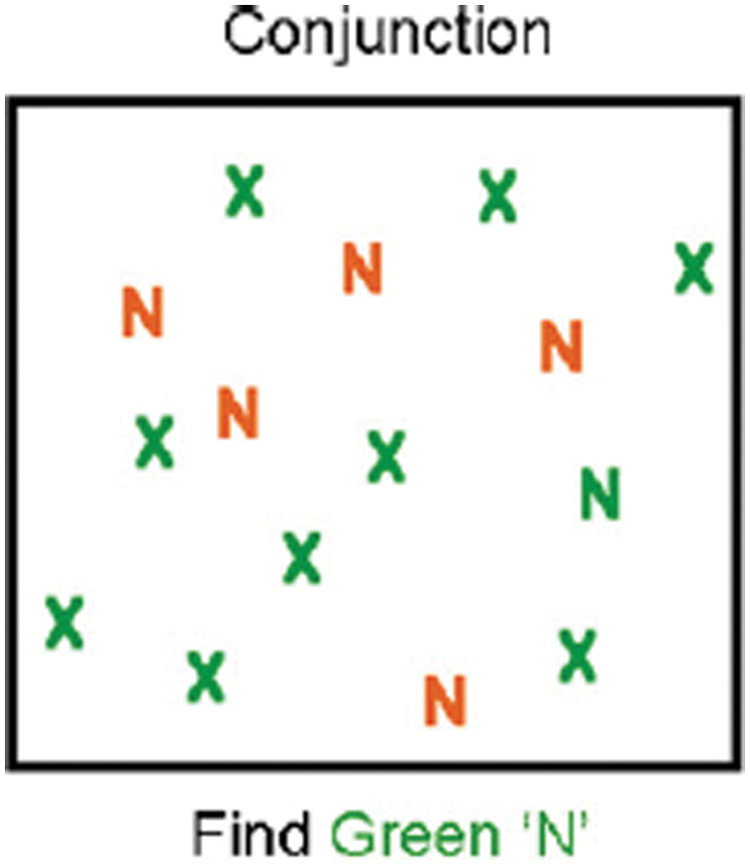
Sample trial for conjunction search task used by Viskontas and others (2011). Instructions were to indicate whether there is a green “N” in the display. Note that serial search of each item is required to complete the task.
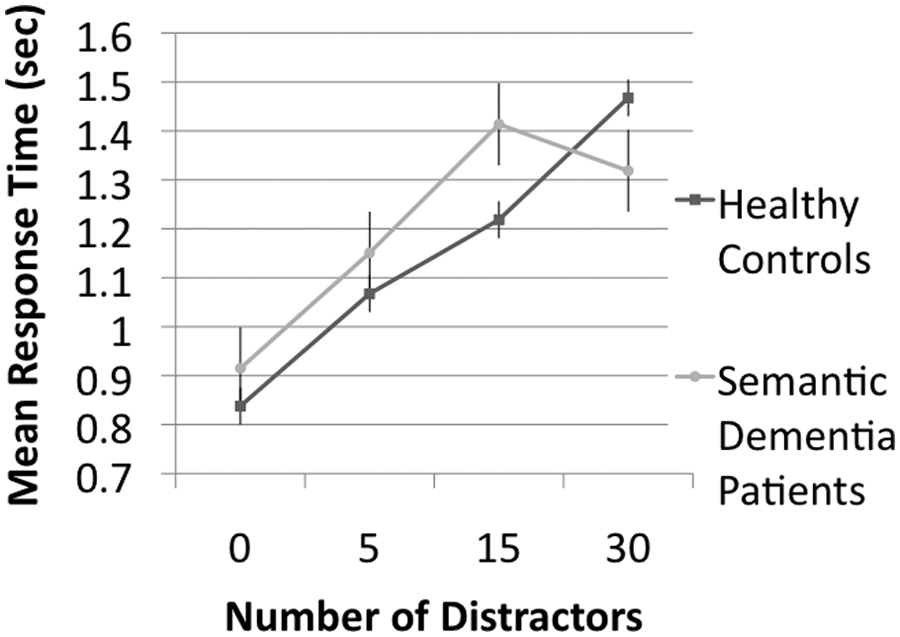
Mean response time performance on conjunction search task by healthy controls and patients with semantic dementia. Error bars represent standard error of the mean. Note that semantic dementia patients were faster than control participants in the most difficult condition (target embedded among 30 distractors).
In addition, Gansler and others (2011) have reported VBM data from the figural subtest of the Torrance Test of Creative Thinking, showing that an increase in gray matter in a region of the right parietal lobe correlates with divergent reasoning and visuospatial processing. The enhancement of function in the right posterior brain may account for the increase in focused visuospatially based activities in these patients, whether in jigsaw puzzles, the design of beautiful gardens, or the creation of visual art. This alteration in visual search may be one mechanism by which patients with semantic dementia create paintings with vivid and repetitive geometric patterns.
Positive Aspects of Cognitive Aging
On 15 January 2009, Captain Chesley Sullenberger successfully landed an engineless plane in the Hudson River, New York and in doing so saved the lives of all 154 people aboard the plane (Figure 8). Similar dramatic rescues of crippled aircraft have occurred over the years and most of these events have had one thing in common: A highly experienced pilot was flying the plane. There was a general consensus among professional pilots that it was the training and experience of the pilots in these incidents that enabled them to respond correctly to the extreme challenges that they encountered. Each of these pilots, like Captain Chesley Sullenberger, was close to 60 years old, an age at which airline pilots prior to 2007 were required to retire in the United States, and an age that the cognitive gerontology literature might classify as “old.”
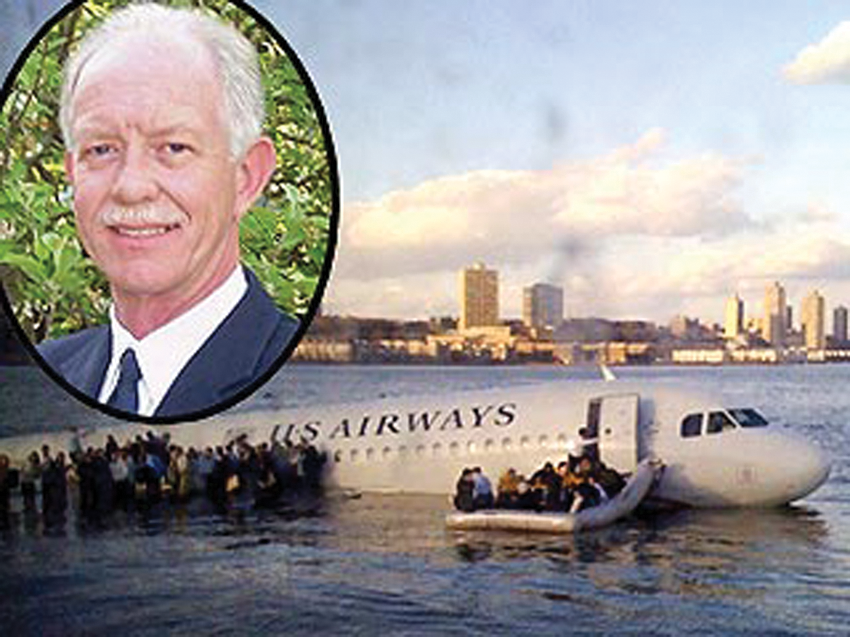
Captain Chesley Sullenberger and the downed US Airways plane in Hudson River, New York. Reproduced by permission.
How are we to reconcile the dramatic skills of airline pilots such as these with a behavioral and neuropsychological literature reporting declines in cognitive functioning? To address this question, we review paradoxical evidence showing that, relative to young adults, older adults show spared (and occasionally even superior) cognitive functioning.
Memory Functioning
Although complaints about failing memory skills are widespread among older adults, and empirical work supports these observations (see Balota and others 2000; Craik 2002 for reviews), not all memory functions are impaired or, at least, not all are equally impaired. For example, impairments are typically greater in recall tasks than in recognition tasks (e.g., Craik and McDowd 1987; Nyberg and others 2003; Schonfield and Robertson 1966). And although memory for specific events may decline whenever recall is required, semantic memory remains intact or even improves with age across the adult lifespan, likely reflecting accumulated knowledge about words, facts and events (Goldberg 2005; Nyberg and others 2003).
Furthermore, unintentional or implicit memory (when retrieval is triggered by a cue without one’s knowledge or awareness) also shows quite a different pattern from intentional recall, with older adults usually showing preserved performance (see Ballesteros and others 2009; Jennings and Jacoby 1993; Light and others 2000). In fact, if anything, older adults tend to rely on implicit memory or contextually driven, automatic retrieval (e.g., Spieler and others 2006). For example, Rowe and others (2006) showed that older adults implicitly acquire information in one situation and tacitly use it in another, resulting in superior performance in the second situation by older, as compared with younger, adults (see also Kim and Hasher 2005). Recent work suggests that healthy older adults learn from and use distraction from one situation to aid their performance in other situations, including those that involve reducing and eliminating forgetting (Biss and others, in press; Campbell and others 2010). These spared implicit memory and tacit learning processes may enable older adults to perform well on such complex tasks as emotional regulation and decision making.
Emotional Regulation
Older adults tend to outperform young adults in emotional regulation (Charles and Carstensen 2010). Compared with younger adults, older adults report being less likely to engage in negative conflict with others (Birditt and Fingerman 2005) and they show greater wisdom when presented with interpersonal and international conflict scenarios (Grossmann and others 2010). They are also more effective at solving hypothetical interpersonal problems (see Blanchard-Fields and others 2007; see also the wisdom work of Baltes and colleagues, e.g., Baltes and Smith 2008). Indeed, across all education, social class, and IQ levels (in a US sample), greater age is associated with greater wisdom in both interpersonal and societal conflict domains (Grossmann and others 2010). Still another facet of the social and affective wisdom of older adults can be seen in story telling situations in which older adults tend to be more responsive to their audiences, whether young children (Adams and others 2002) or other older adults (Sullivan and others 2010) than are young adults.
Problem Solving and Decision Making
Whatever declines there may be in memory performance with age do not translate directly into impairments in everyday problem solving (e.g., Healey and Hasher 2009). Indeed, there are a number of findings showing preserved or enhanced decision-making abilities (Worthy and others 2011). For example, older adults seem to be less susceptible to classic decision biases than younger adults. Consider the “sunk-cost fallacy,” or the tendency to continue with an action once an investment has been made, whether in time or money. This has been widely reported among young adults but is far less prevalent among older adults (see Strough and others 2008). There is also evidence of older adults making reliably more rational choices compared to college students (Kim and Hasher 2005; Tentori and others 2001). As well, older adults appear to use all the information occurring in one situation—whether relevant or not—to solve problems in another situation (Kim and others 2007). Younger adults, by contrast, seem only to have access to the initially relevant information, leaving them impaired should initially irrelevant information become useful (Healey and others 2008).
The greater problem solving and decision making skills of older adults may stem from a number of different factors including of course greater accumulated knowledge. They are also likely to have greater knowledge about their own goals, values, and priorities (see Kim and others 2008). Alternatively, or in addition, older adults’ reliance on automatic, intuitive processes may enable them to succeed whenever intuitive or heuristic processing yields effective solutions (e.g., Gigerenzer and Selten 2001).
Conclusions
Contemporary neuroscience sees the brain as a non-linear device, which relies on dynamic synchrony and balance between neural systems. Damage to the brain may upset this dynamic state, and repair may often entail interventions that restore a degree of synchrony and balance. Without playing down the very real losses that often arise, the paradoxical enhancements noted in this article emphasize the importance of looking at change rather than simply focusing on deficit. This focus echoes a broader approach seen in the fields of positive psychology and positive clinical psychology that places emphasis on dispositional optimism, flourishing, resilience, and functional reserve in coping with impairment (Seligman and Csikszentmihalyi 2000; Wood and Tarrier 2010). The emerging fields of “positive neurology” and “positive neuropsychology” have a similar focus, with concepts such as resilience having a greater focus over the past few years (see http://www.posneuroscience.org). These fields point to a greater emphasis on intact skills, on past strengths and interests, and on how both rehabilitation efforts and domestic, social and work environments can be altered to take these skills and talents into account. Our approach is, in parallel, seeking out examples where function of itself may be improved after brain lesions. These paradoxical phenomena may not only open up novel ways of assisting patients but also provide fresh insights into the functioning of the normal human brain (Kapur 2011).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Indre Viskontas acknowledges funding support from the McBean Family Foundation, and Professor Lynn Hasher’s work was supported by the Canadian Institutes of Health Research, Grant Number MOP89769.