
Abstract
Introduction
Informal carers provide essential support for people diagnosed with cancer, however, the demands of caregiving can negatively impact their psychological wellbeing. There is a need to examine psychological wellbeing among carers of First Nations cancer patients to understand the impacts of caregiving within cultural contexts. Therefore, this study aims to quantify carer psychological distress, burden, and quality of life (QoL) among carers of First Nations Australian cancer patients - key indicators of carer wellbeing that may have implications for both carers and patients.
Methods
This prospective cross-sectional study recruited adult (≥18 years) carers of First Nations Australians diagnosed with cancer across six Queensland hospitals (July 2021-December 2024). Of 221 eligible carers, 172 (78%) participated in the study. Logistic regression models assessed association between carer characteristics with high psychological distress (Distress Thermometer, score≥4) and significant carer burden (six-item Zarit Burden Interview, score≥6); linear models assessed associations with QoL (CarerQoL-7D).
Results
165 (96%) carers approached were included in the analysis, of which 67% (n=111) identified as First Nations. High distress was reported by 43% (95% CI:36%-51%), 44% reported significant carer burden (95%CI:37%-52%), and mean CarerQoL-7D score was 9.7 (95%CI:9.3-10.1). Only prevalence of high distress differed between First Nations and non-Indigenous carers. For all carers as well as First Nations carers, clinical diagnosis of anxiety and/or depression was associated with high distress, significant carer burden and lower QoL.
Conclusion
To our knowledge, this study is the first to quantify the psychological wellbeing of carers of First Nations cancer patients in Australia. We observed no associations typically expected for wellbeing and distress among carers, except for with clinical anxiety/depression, suggesting that existing measures may not fully capture carer’s experiences in this population. These findings highlight the need for culturally appropriate measures co-designed with Indigenous communities to better assess and support carer wellbeing.
Plain Language Summary
Keywords
Introduction
Carers are a critical source of support for people who are living with illness or disability. In Australia, there are approximately 3 million informal carers, defined as those who provide unpaid care for people living with illnesses or disability. 1 Informal carers are most often family members, friends, or other loved ones of the care recipient, who are often extensively involved in the daily routines of people living with cancer, such as assisting with household chores (e.g. shopping, cleaning), treatment (e.g. organising, transportation to appointments); and providing emotional support.2,3 The support provided by informal carers often replaces care that would otherwise been provided by health professionals. 4 Consequently, support from Australian informal carers provides a considerable benefit to the health system, saving approximately $80 billion per year. 4 With an aging population and increasing cancer incidence, the number of informal carers is expected to grow. 2 Despite their significant contributions to cancer care and the general wellbeing of patients, informal carers typically receive little formal support or training. 5 Inadequate support can lead to increased burden and poorer wellbeing, particularly among vulnerable populations such as carers of Indigenous people. 6
Indigenous people globally experience higher prevalence of cancer, and poorer cancer outcomes compared with non-Indigenous populations. 7 In Australia, Aboriginal and Torres Strait Islander people (hereafter respectfully referred to as First Nations peoples) experience 14% greater cancer incidence and 1.4 times higher mortality attributed to cancer than non-Indigenous Australians.8,9 These disparities are shaped by the ongoing impacts of colonisation, including intergenerational trauma, systemic racism, socioeconomic disadvantage, and experiences of discrimination within healthcare settings. 7 Such factors contribute to mistrust of health services, reduced engagement with screening and early diagnosis, and lower access to timely and culturally safe treatment.5,7 Geographical inequalities further exacerbate these challenges. An estimated 59% of First Nations peoples live in regional or remote areas of Australia, 10 compared with 27% of non-Indigenous Australians, which may limit access to specialist cancer care and supportive services. Together, these structural, social, and geographic factors increase the cancer burden among First Nations people and create additional demands on families and informal carers, who often provide substantial emotional, practical, and cultural support to patients.
Although caregiving can be a rewarding experience for some, strengthening relationships and fostering appreciation of life,2,11 it is widely recognised as a source of considerable physical and psychological burden.2,3 Evidence suggests that distress and unmet care needs reported by informal carers may be greater than those experienced by the patients themselves.3,12 A carer’s wellbeing is influenced by multiple factors, including balancing their role as a carer alongside work commitments and parenting responsibilities; changes to social and community engagement; and the emotional strain of supporting a loved one through their cancer care journey.2,3,13 Carers of Indigenous people are reported to experience similar challenges to other carers, but also experience additional stressors. These include unmet preferences for family-focused care, limited culturally competent health services, and overall poorer health compared with non-Indigenous carers. 6 A systematic review of carers of Indigenous cancer patients from Australia, Canada, New Zealand, and the United States highlighted further challenges, such as explaining cultural values and needs to treatment teams, coping with experiences of racism in the healthcare setting, and navigating a health system often viewed with caution or mistrust by First Nations people. 5
The wellbeing of carers is shaped by psychological, emotional, and functional aspects of health. Carers of First Nations peoples with cancer often have unmet mental and emotional support needs and may experience elevated levels of distress. 14 Psychological distress reflects acute emotional responses to caregiving demands, while caregiver burden captures the perceived strain associated with caregiving roles, including mental, emotional, and physical demands. Quality of life (QoL) measures enables the assessment of the broader impact of caregiving on physical, social, and financial wellbeing. Together, these constructs represent related but distinct and complementary dimensions of carer wellbeing and provide a comprehensive understanding of the impact of caregiving. 15 Although extensive research has assessed carer wellbeing in general cancer populations, the wellbeing of carers of First Nations cancer patients has not previously been quantified. There are several identified risk factors for poorer QoL among all carers such as sex, age, education level, and employment, however these factors have not been assessed for carers of First Nations cancer patients. 16 Consequently, it is essential to assess carer wellbeing in this context, in the interest of sustaining wellbeing of both the carer and cancer patient.
The aim of this study is to investigate carer distress, burden, and QoL among informal carers of First Nations Australian cancer patients and to assess the relationship between demographic and clinical characteristics with carer distress, burden and QoL. To our knowledge, our study provides the first estimates of these wellbeing measures for carers of First Nations Australians with cancer. The findings of this study may improve understanding of carers’ experiences, and inform the development of culturally safe services, policies or interventions that support the wellbeing of carers of First Nations people and the patients they care for.
Methods
Study Design & Setting
This prospective cross-sectional study utilised survey data collected from informal carers of First Nations Australian cancer survivors. Carers were recruited from cancer care units in six Queensland hospitals that serve a wide range of patients from metropolitan, regional, and remote communities. Study recruitment occurred between July 2021 and December 2024, with a pause from December 2021 to May 2023 due to the impact of COVID-19. This study is part of the broader Supporting Our Carers Study (SOCS) project (Project ID: IN180100047). The overarching aim of the SOCS Project is to understand and assess the psycho-social needs of First Nations Australian cancer patients and their informal carers. The project was led by a senior Aboriginal researcher (GG), with support from First Nations Australian staff and community members in the development of the project resources and outputs. No a priori sample size or power calculation was performed for this cross-sectional survey. All eligible participants with available data from the SOCS Project were included in the analysis.
Ethics Approval
This study as part of the broader SOCS project was conducted in accordance with the Declaration of Helsinki (revised 2024), 17 and has received approval from the following Ethics Committees:
The Northern Territory Department of Health and Menzies School of Health Research HREC (NTHREC; HREC ID: 2020-3790; 9th September 2020); The University of Queensland (UQ) HREC (HREC ID: 2021/HE002242; 30th September 2021) and the Queensland Government Metro South Hospital and Health Service HREC (HREC ID: HREC/2020/65533) on 10th December 2020, which cover the approved study sites. The participating site-specific approvals were obtained from relevant Research Governance Offices (RGOs) at Princess Alexandra Hospital (MSHHS RGO); Royal Brisbane and Women’s Hospital (Metro North HHS RGO); Ipswich Hospital (West Moreton HHS RGO); Bundaberg Hospital (Wide Bay HHS RGO); Townsville Hospital (Townsville HHS RGO); and Cairns Hospital (Cairns HHS RGO).
Participants
Informal carers (i.e., unpaid, non-professional) of First Nations people with a cancer diagnosis were eligible to participate in the study if they had cared for someone within the past 2 years, were aged 18 years or older, able to understand English, and physically and mentally capable of participating. Participants could either identify as non-Indigenous, or First Nations Australian, as long as they care for First Nations cancer survivors. The carer’s eligibility was not restricted by when caregiving occurred within the past two years, nor by caregiving duration or intensity, or by stage of recipient’s illness. Multiple carers could be recruited for an individual cancer survivor. Broad eligibility criteria and inclusion of all available eligible participants helped minimize selection bias.
Recruitment & Data Collection Procedure
Participants were recruited using a selective, purposive sampling approach. Informal carers were identified by the patient or onsite project coordinator. Onsite coordinators assessed carers for eligibility and collected contact information for each person nominated. If eligible, their details were given to the university research team who contacted them to provide a study information sheet and seek their interest in participating in the study, and if interested a day and time was agreed to complete the survey. Eligibility was re-confirmed, informed consent was obtained (written consent in person, informed verbal consent on the phone) and the study survey was completed by an interviewer- or was self-completed by the participant. Participants were provided with a $40 gift card to reimburse their time participating in the study and asked if they would like a summary of research finding at the end of the study. All participant data were de-identified prior to analysis. Identifiable information (including name, phone number, email address and residential address) was removed during data entry into a Microsoft Excel database, and each participant was assigned a unique study identification code. De-identified data were securely stored on the University of Queensland’s Research Data Manager (RDM) platform, a secure cloud-based storage system accessible only to the research team members responsible for data management and analysis.
Variables
Carers Characteristics Overall and by Indigenous Status

GI gastrointestinal.
*Highest level of education completed. Junior high school or below: did not complete primary school or had no formal schooling, primary school (Grade 1 to 6 in Queensland) or junior primary school (Grade 7 to 9 in Queensland). Senior high school: Grade 10 to 12 in Queensland. Trade diploma: trade or technical certificate or diploma. Degree: a tertiary degree (e.g., university, college).
@Current employment was reported by 162 (98%) carers (110 (99%) First Nations carers, 52 (96%) non-Indigenous carers).
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
§Modified Monash Model (MMM) of remoteness.
&Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
¥Cancer diagnosis was reported by 157 (95%) carers (103 (93%) First Nations carers, 54 (100%) non-Indigenous carers), who could report more than one cancer diagnosis.
+Other cancers included: skin, brain and central nervous system, head and neck, endocrine and gynaecological cancers.
∼p-value from Chi-squared tests for categorical measures, from an unpaired t-test for the mean age and Wilcoxon rank-sum test for median age row.
The Modified Monash Model (MMM) 18 was used to define residential area (metropolitan areas, regional, remote/rural) via participant’s suburb and postcode. Living in an area of disadvantage was based on the participant’s residential postcode and the Australian Bureau of Statistics Socio-Economic Indexes for Areas (SEIFA), 19 Index of Relative Socio-Economic Advantage and Disadvantage (IRSAD) state deciles, 19 with deciles classified as being disadvantaged (≤2nd decile, relative greater disadvantage and a lack of advantage) and not disadvantaged (3rd to 10th decile).
Measurements
Carer Psychological Distress
The Distress Thermometer (DT) was used to assess psychological distress amongst participants (see Supplemental Table 1). 20 The DT was selected due to its brevity, ease of administration, and widespread use as a validated screening tool for psychological distress in oncology settings. 21 It has been previously used to screen distress amongst First Nations Australian cancer survivors. 22 The DT is a single item visual ‘thermometer’ scale, ranging from zero (no distress) to 10 (extreme distress). Participants were asked to ‘indicate the number (0-10) that best describes how much distress you have been experiencing in the PAST WEEK including today.’ Distress was categorised into low distress (score<4) and high distress (score ≥4), informed by established recommended cutoff scores. 23
Carer Burden
Participants’ perceived carer burden was assessed using the 6-item Zarit Burden Interview (ZBI-6), a measure validated in informal caregiver populations, including those caring for people with cancer and chronic illness. 24 Whilst the ZBI-6 has not been validated for caregivers of First Nations Australian cancer patients, it was selected due to its established psychometric properties and relevance to key caregiving domains. The measure asks participants how they currently feel in relation to their caregiving experience, addressing key domains of: emotional strain; loss of control; social strain/isolation; and relationship strains. Response options are on a 5-point Likert scale (0= Never; 1= Rarely; 2= Sometimes; 3= Quite frequently; 4= Nearly always). Sum scores were calculated for each participant on a scale of 0-24. Caregiver burden was categorised into low burden (score<6) and significant caregiver burden (score≥6). 24
Carer Quality of Life (QoL)
Participants’ QoL was assessed using the CarerQoL-7D measure 25 to assess the impact caring has on them across seven areas: fulfilment; relational problems; mental health problems; physical health problems; problems combining care with daily activities; financial problems; and social support. The CarerQoL-7D includes both positive (items 1 and 6: fulfilment and social support) and negatively framed items (items 2-5, 7). Responses options were on a 3-point Likert scale, with positive items being scored as: 0= no; 1= some; 2= a lot of, and negative items having a reverse scoring. Sum scores out of the 7 items were calculated for each participant on a scale from 0 (poor QoL) to 14 (high QoL). The CarerQoL-7D is a validated measure of caregiver QoL for informal caregiver populations in cancer and palliative care settings; however it has not been validated for caregivers of First Nations Australians with cancer.26,27
Statistical Methods
Demographic and outcome measures were summarised for all carers and stratified by Indigenous status with these measures were compared using Chi-squared tests for categorical measures, and an unpaired t-test and Wilcoxon rank-sum test were used to compare the continuous measure of age. Association between demographic and health measures with each outcome was assessed using a regression framework. Logistic regression models were fit for the binary outcomes (carer distress, carer burden) and linear regression models for the continuous outcome (carer QoL) with robust errors to take into account the potential correlation between the outcomes of participants caring for the same First Nations cancer patient. Univariable regression models were first conducted to assess the association between each explanatory variable with each outcome. Variables were then simultaneously included in multivariable regression models to estimate adjusted associations. Participants were included in the analysis if they had complete data for the variables used in the model and at least one outcome. All analyses were performed using Stata 19.0. The reporting of this study follows the STROBE guidelines. 28
Results
Participants Characteristics
172 (78%) of 221 carers (First Nations and non-Indigenous) were approached to participate in the study (Figure 1). Of these, 165 (96%) carers had complete data for the measures used in the regression analysis and had at least one outcome. Of the carers, 67% were First Nations, 63% were aged 45 years and older, 77% were female, 64% were in a relationship, 56% were currently not working, and 26% self-reported having an anxiety and/or depression diagnosis (Table 1). Participant flow diagram
Comparison of First Nations and Non-indigenous Carers
First Nations (n=111) and non-Indigenous (n= 54) carers differed by age, marital status, relationship to patient and the remoteness of their residence (Table 1). 46% of First Nations carers were under 45 years of age compared to 19% of non-Indigenous carers. Around half of First Nations carers were in a relationship (partner/de facto/married) compared to 89% of non-Indigenous carers. Three quarters of non-Indigenous carers were carers for their wife/husband/partner compared to only 16% of First Nations carers. 19% of First Nations carers were living in metropolitan, and 69% in regional areas compared to 43%, and 50% of non-Indigenous carers. First Nations and non-Indigenous carers were comparable for sex, level of education, employment status, number of medical conditions, anxiety and/or depression, and living in a disadvantage area.
Carer Distress, Burden, and QoL
Outcomes Overall and by Indigenous Status

+Distress thermometer (on a scale of 0-10): low distress score<4, high distress score ≥4.
#6-item Zarit Burden Interview (ZBI-6, on a scale of 0-24): low caregiver burden <6, significant caregiver burden ≥6.
&CarerQol-7D on a scale of 0 (low QoL) to 14 (high QoL).
¥p-value from an unpaired t-test.
Associations Between Sociodemographic and Clinical Characteristics of all Carers With Psychological distress + (n=164)
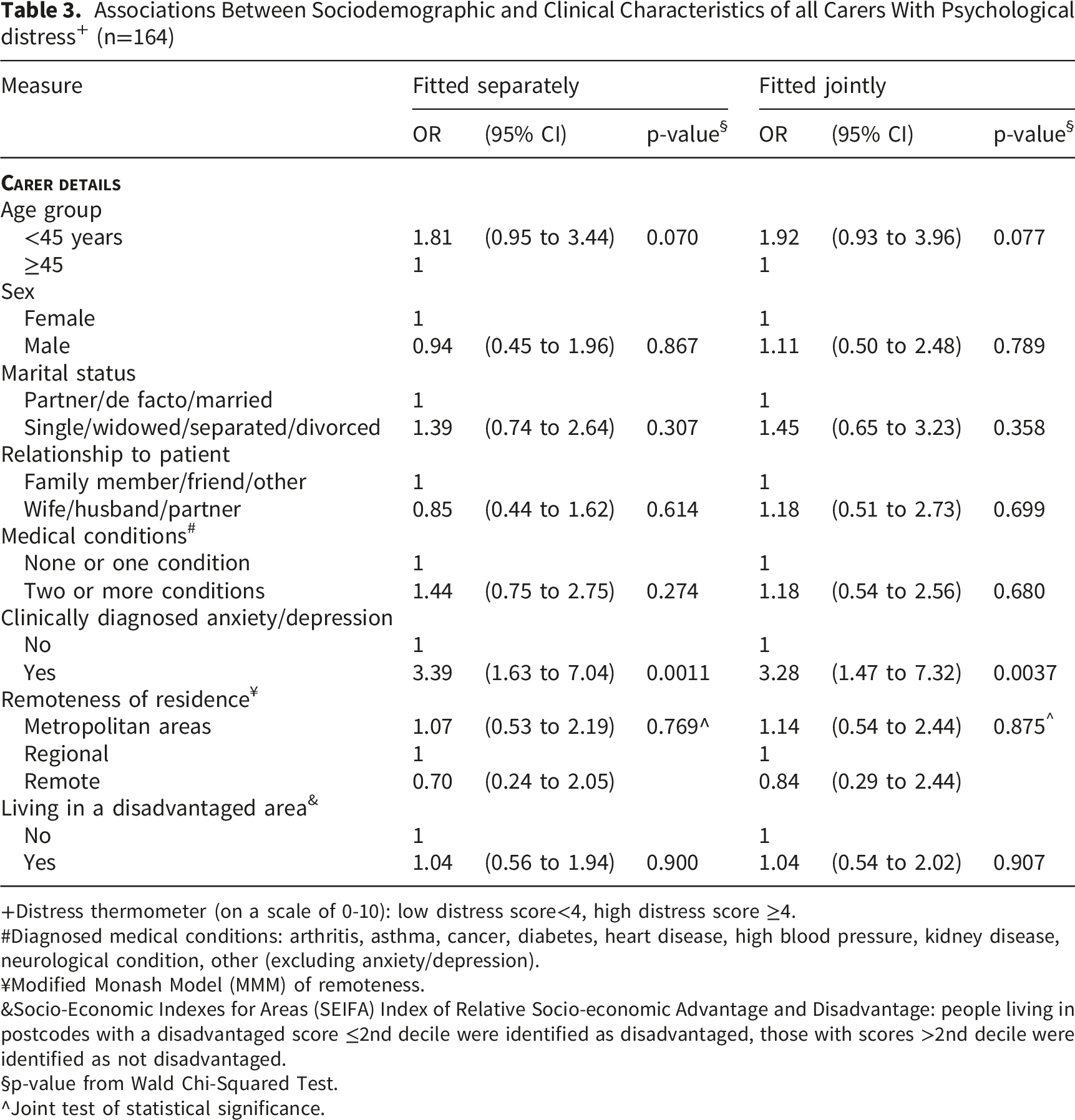
+Distress thermometer (on a scale of 0-10): low distress score<4, high distress score ≥4.
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
¥Modified Monash Model (MMM) of remoteness.
&Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
§p-value from Wald Chi-Squared Test.
^Joint test of statistical significance.
Associations Between Sociodemographic and Clinical Characteristics of all Carers With Carer Burden + (n=165)
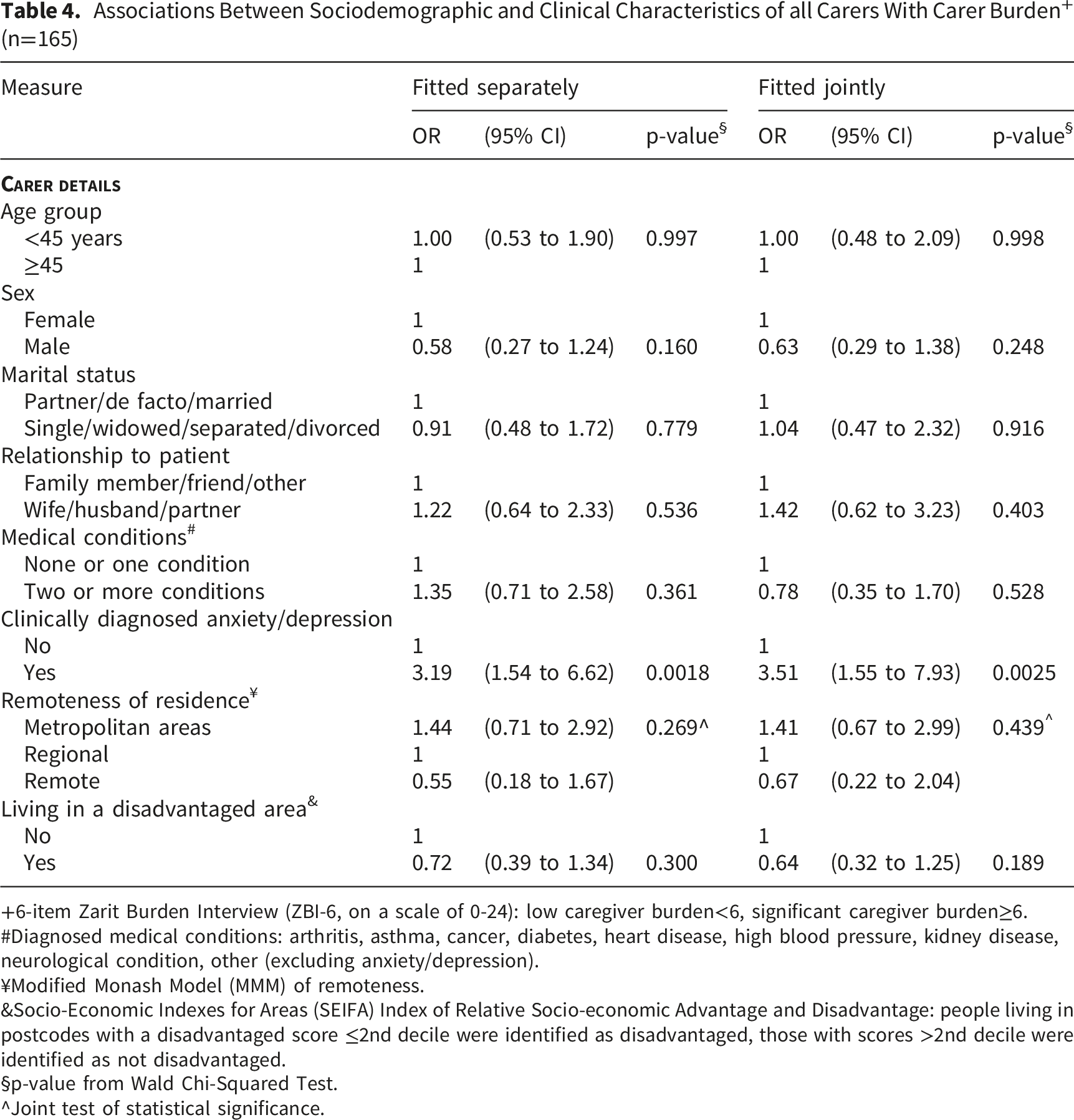
+6-item Zarit Burden Interview (ZBI-6, on a scale of 0-24): low caregiver burden<6, significant caregiver burden≥6.
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
¥Modified Monash Model (MMM) of remoteness.
&Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
§p-value from Wald Chi-Squared Test.
^Joint test of statistical significance.
Associations Between Sociodemographic and Clinical Characteristics of all Carers With QoL + (n=165)
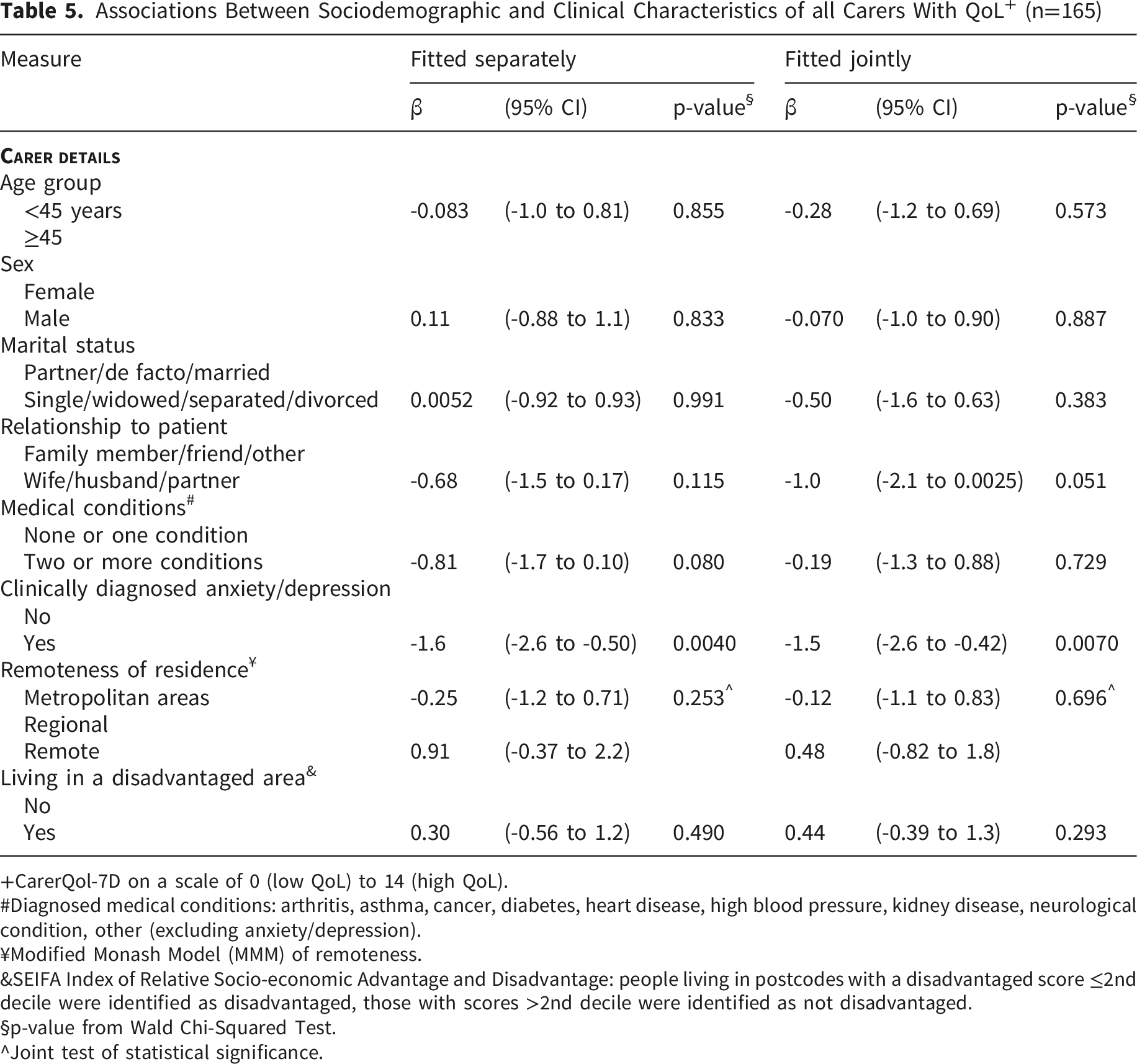
+CarerQol-7D on a scale of 0 (low QoL) to 14 (high QoL).
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
¥Modified Monash Model (MMM) of remoteness.
&SEIFA Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
§p-value from Wald Chi-Squared Test.
^Joint test of statistical significance.
Associations Between Sociodemographic and Clinical Characteristics of First Nations Carers With Psychological distress + (n=110)
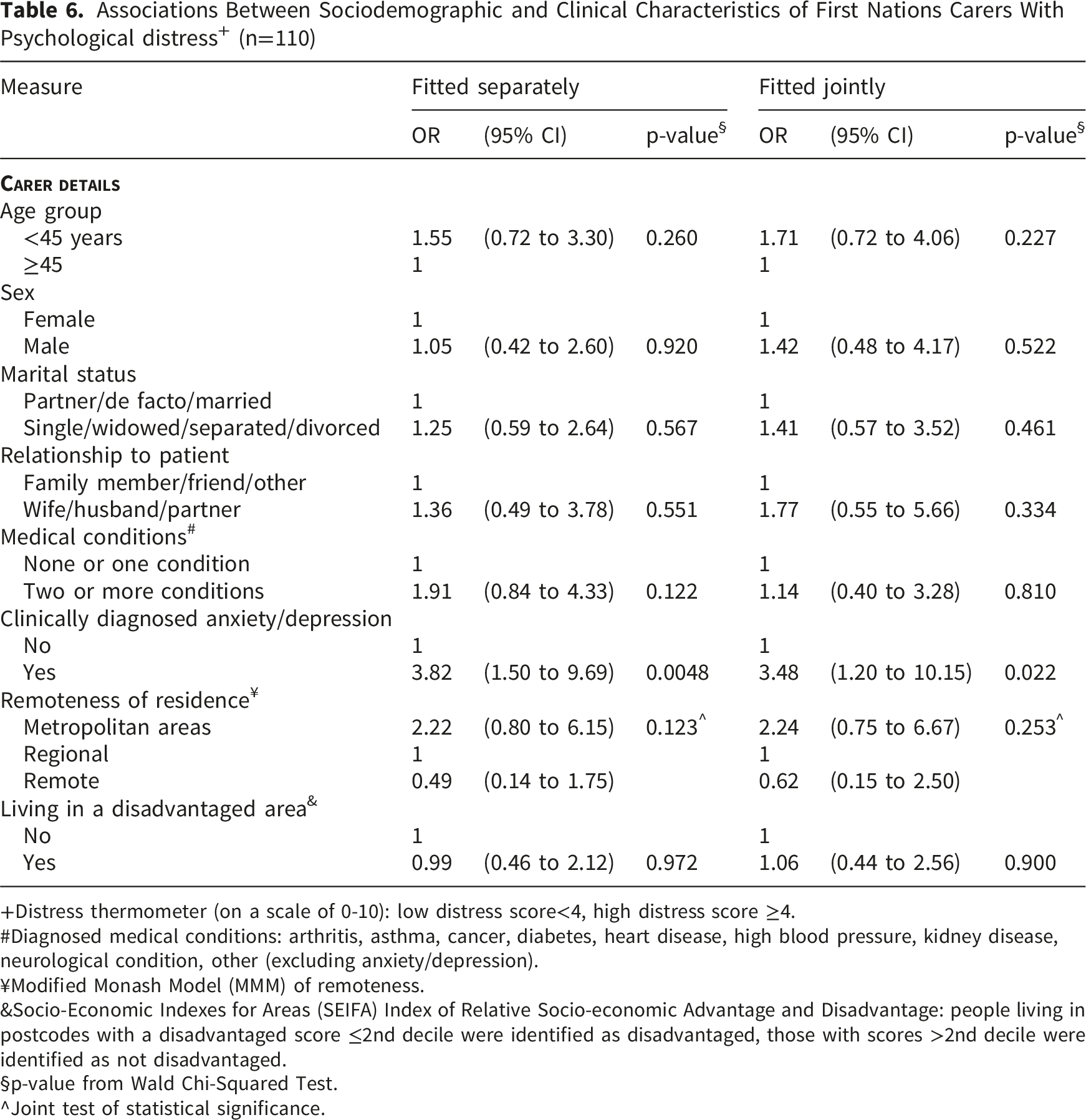
+Distress thermometer (on a scale of 0-10): low distress score<4, high distress score ≥4.
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
¥Modified Monash Model (MMM) of remoteness.
&Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
§p-value from Wald Chi-Squared Test.
^Joint test of statistical significance.
Associations Between Sociodemographic and Clinical Characteristics of First Nations Carers With Carer Burden + (n=111)
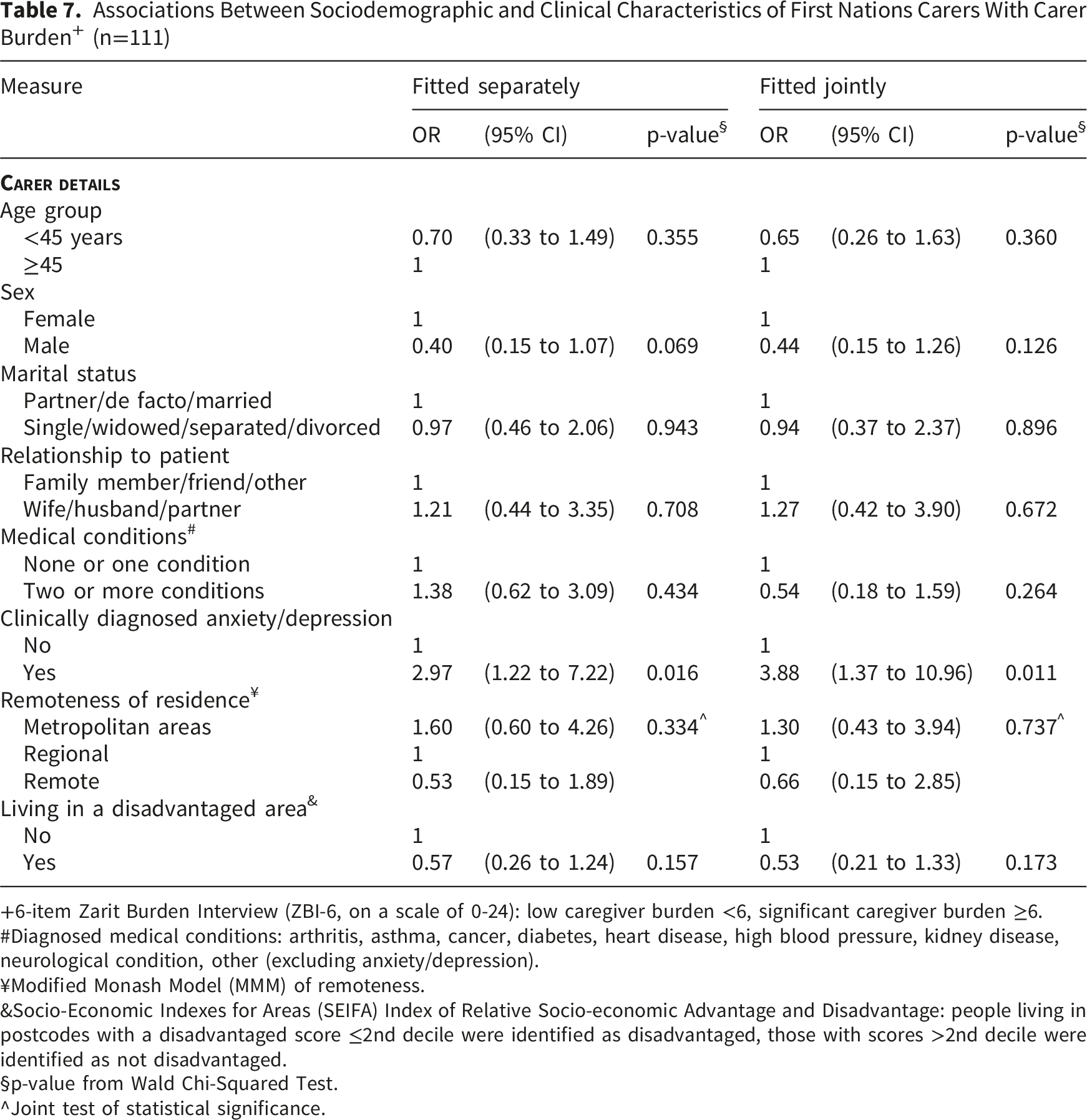
+6-item Zarit Burden Interview (ZBI-6, on a scale of 0-24): low caregiver burden <6, significant caregiver burden ≥6.
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
¥Modified Monash Model (MMM) of remoteness.
&Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
§p-value from Wald Chi-Squared Test.
^Joint test of statistical significance.
Associations Between Sociodemographic and Clinical Characteristics of First Nations Carers With QoL + (n=111)
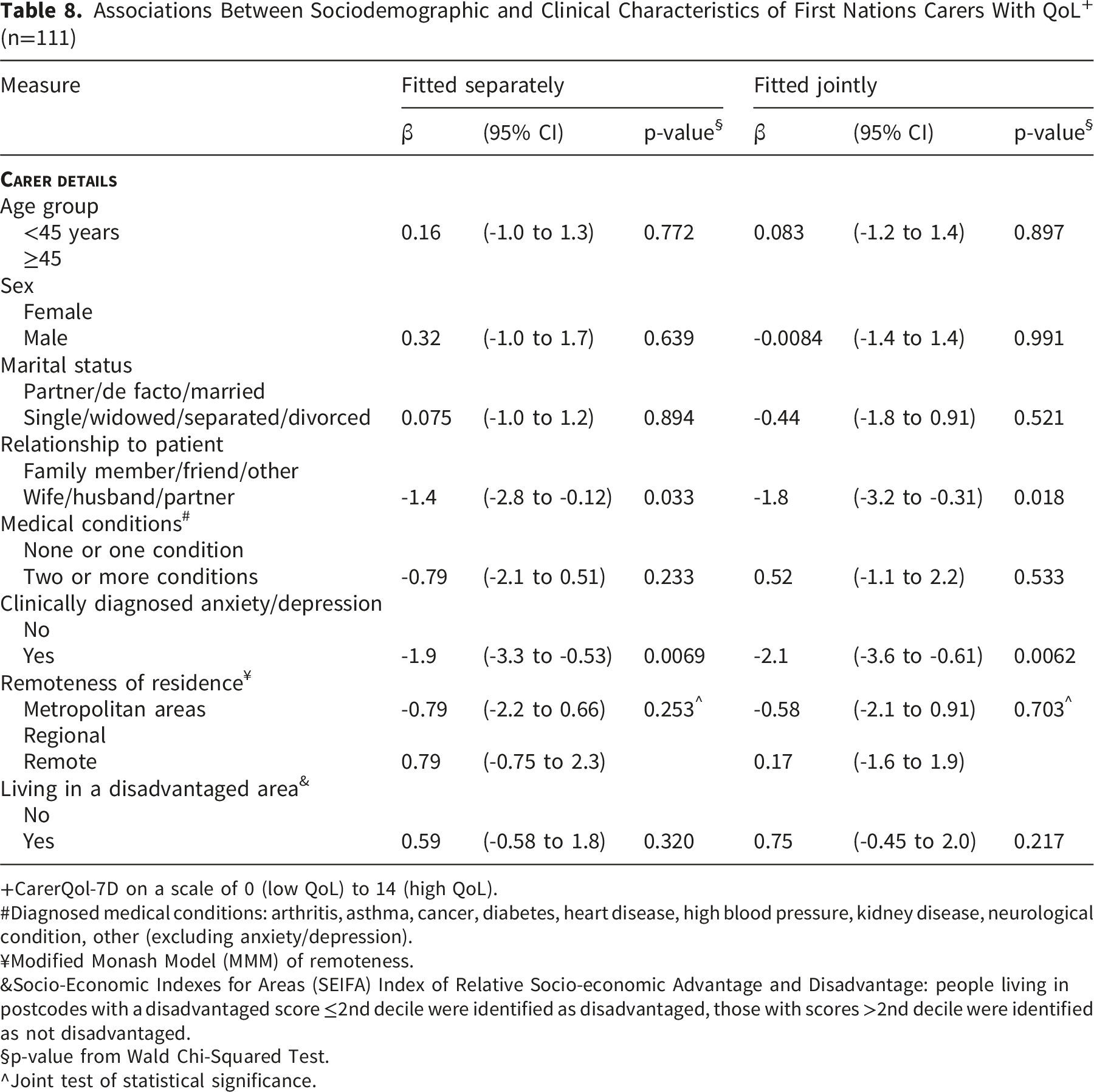
+CarerQol-7D on a scale of 0 (low QoL) to 14 (high QoL).
#Diagnosed medical conditions: arthritis, asthma, cancer, diabetes, heart disease, high blood pressure, kidney disease, neurological condition, other (excluding anxiety/depression).
¥Modified Monash Model (MMM) of remoteness.
&Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Advantage and Disadvantage: people living in postcodes with a disadvantaged score ≤2nd decile were identified as disadvantaged, those with scores >2nd decile were identified as not disadvantaged.
§p-value from Wald Chi-Squared Test.
^Joint test of statistical significance.
Discussion
To our knowledge, this is the first study to quantitatively assess distress, caregiver burden, and QoL among carers of Australian First Nations cancer patients, and to examine factors associated with these outcomes. In this study, 43% of carers reported high distress, 44% experienced significant caregiver burden, and the average QoL score was 9.7. Multiple factors, including sociodemographic characteristics, employment, remoteness, and number of medical conditions, were assessed for associations with these outcomes. Carers with anxiety or depression were more likely to report distress, higher caregiver burden, and lower QoL, and carers providing care for a partner/spouse had lower QoL. This suggests that, for First Nations carers, mental health—specifically anxiety and depression—plays a central role in their distress, caregiver burden, and QoL, whereas other sociodemographic or health-related characteristics appear less influential.
In our study, carers with anxiety or depression were more likely to report distress, caregiver burden, and lower QoL. These associations with anxiety and depression were observed both in the overall carer sample and specifically among First Nations carers, highlighting the consistent impact of mental health on carer outcomes Anxiety and depression have previously been described as key factors associated with the wellbeing of carers, particularly among female carers,29,30 and are associated with unmet needs and poorer psychological outcomes and wellbeing.26,30 A 2012 review have confirmed the relationship between carer distress and anxiety and depression. 29 Anxiety, depression, and other mental health conditions have been previously recognised as a support need among carers of First Nations Australians with cancer. 31 Our findings indicate that anxiety and depression are key contributors to the wellbeing of carers of First Nations cancer patients. Support services should therefore prioritise mental health, including routine screening for distress, anxiety, and depression, and access to culturally appropriate psychological support. Integrating carer-focused support within cancer care services and community-based programs may help address the high levels of distress and burden identified in this study.
While anxiety and depression were strongly associated with carer outcomes in our study, other factors typically linked to carer distress, burden and QoL were not significant among carers of First Nations people with cancer.2,16 Although caring for a partner showed a marginal association with lower QoL, no other sociodemographic or health-related factors were associated with the outcomes. This may partly reflect limitations of the instruments used in this study. Distress was assessed over the past week to capture current psychological wellbeing, which may be influenced by both ongoing caregiving and prior caregiving experiences within the preceding two years. For example, the Distress Thermometer (DT) has demonstrated limitations in capturing distress in this population, as previous research by Garvey et al. similarly observed lower than expected levels of clinically significant distress reported among the First Nations using the DT, and raised questions on its validity in this context. 22 Notable concerns with the DT include its simplicity not permitting a more accurate representation of the issues which lead to distress, and respondent confusion related to the definition of the concept of ‘distress’. 32 Additionally, the established cutoff score of four may not be optimal, with recent revisions suggesting a reduced cutoff score of three for assessing distress levels within one month of cancer diagnosis.22,33,34
The measures of wellbeing observed in this study are constructed with values aligned with Western biomedical framework and may not fully capture Indigenous concept of wellbeing, which encompass the physical, cultural, spiritual, and social constructs being represented, alongside connection with land or Country. 35 A recent systematic review of quality-of-life measures among Indigenous people globally identified that though there are some measures which have demonstrated validity in this population, few had been adequately translated into the local Indigenous context. 36 The review suggested that Western measures for wellbeing may be used in Indigenous populations, but should be interpreted with caution due to the absence of relevant domains. 36
Our findings highlight the need for the development of a culturally appropriate tool to assess the wellbeing and unmet needs of carers of First Nations patients. First Nations Australians are a population with distinct cultural needs which must be considered when measuring wellbeing. Existing measures that meet the specific needs of First Nations people and their carers is limited. 37 Future measures should be developed using codesign principles in collaboration with First Nations communities and carers, ensuring that the domains and constructs reflect culturally relevant aspects of wellbeing, including physical, emotional, social, and spiritual dimensions.
Although the high number of First Nations carers included in this study may provide some information on wellbeing outcomes, the low number of non-First Nations caregivers may limit the generalisability of the findings. Our study reports analyses of survey data collected prospectively from eligible participants within the SOCS project, and power calculations were not performed prior to analysis. The sample size for some subgroups may have been insufficient to detect significant associations for certain sociodemographic and health-related factors. Consequently, the non-significant findings for some predictors may reflect limited statistical power rather than a true absence of association. All demographic and health-related information was self-reported, which may be subject to recall bias or misclassification. The timing of diagnosis of anxiety and/or depression relative to the caregiving role, as well as treatment status, was not available, limiting interpretation of temporal relationships. Our study did not assess the influence of being responsible for providing care for more than one person, which may be a limitation. Family and community are a key component of wellbeing for First Nations people, with many carers of First Nations people also providing care for others with illness or disability. It has been suggested that the strong community and family values may present an opportunity for sharing the burden of care with others, although hesitancy to seek support due to silence on cancer may be a barrier.5,6,38
Conclusion
Informal carers of First Nations cancer patients play a crucial role in supporting their loved ones, but caregiving may negatively affect their wellbeing. In this study, carers with anxiety or depression were more likely to report higher level of distress, greater carer burden, and lower QoL. QoL was reported to be lower among those who were providing care for their partners. No other factors examined were significantly associated with wellbeing outcomes. They highlight the need for culturally tailored measures, developed in collaboration with First Nations communities and carers to more accurately reflect the carer’s wellbeing and guide the development of appropriate support services.
Supplemental Material
Supplemental material - Psychological Distress, Caregiver Burden and Quality of Life Among Informal Carers of First Nations Australians Diagnosed With Cancer: A Cross-Sectional Study
Supplemental material for Psychological Distress, Caregiver Burden and Quality of Life Among Informal Carers of First Nations Australians Diagnosed With Cancer: A Cross-Sectional Study by Idin Panahi, Helena Romaniuk, Shafkat Jahan, Kenneth Carter, Jacinta Elston, Gail Garvey in Cancer Control
Footnotes
Acknowledgments
We acknowledge Rachael Jaenke, who provided project management and support for this project. We also gratefully acknowledge the study site coordinators at the Princess Alexandra Hospital, Royal Brisbane and Women’s Hospital, Ipswich Hospital, Bundaberg Hospital, Townsville University Hospital, and Cairns Hospital for their support with participant recruitment. We also acknowledge the extended SOCS research team who supported the project through participant recruitment, data collection, and data management.
Ethical Considerations
This study was undertaken in accordance with the NHMRC Guidelines for the ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities and in accordance with the Declaration of Helsinki (revised 2024). Ethics approval was received from the following Committees: the Northern Territory Department of Health and Menzies School of Health Research HREC (NTHREC; HREC ID: 2020-3790; 9th September 2020); The University of Queensland, HREC (UQ HREC; 2021/HE002242; 30th September 2021); and the Metro South Hospital and Health Service HREC (MSHHS; HREC/2020/QMS/65533; 10th December 2020) which covered the approved study sites.
Consent to Participate
Informed written or verbal consent (depending on in-person or phone call survey) was obtained from all participants included in the study.
Author Contributions
• Conceptualisation: GG, HR.
• Methodology: KC, HR, SJ, GG.
• Data curation: HR, KC.
• Formal analysis: HR.
• Writing- original draft: IP, HR, SJ, KC.
• Writing- review & editing: IP, HR, SJ, KC, JE, GG.
• Supervision: GG, JE.
• Funding acquisition: GG.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Australian Research Council (ARC) Discovery Indigenous Scheme, under the project title: Assessing supportive care needs of Indigenous cancer survivors’ caregivers (Project ID: IN180100047) and a National Health and Medical Research Council (NHMRC) Centre of Research Excellence in Targeted Approaches To Improve Cancer Services for Aboriginal and Torres Strait Islander Australians (TACTICS; GNT1153027). GG was supported by an NHMRC Investigator grant (GNT2034453).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article is not available due to ethical and privacy restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.