
Abstract
Introduction
The Lessening the Impact of Financial Toxicity (LIFT) intervention—a financial navigation intervention—demonstrated preliminary effectiveness. Scaling LIFT to an eight-site single-arm trial, however, posed implementation challenges that were not present in the single-site pilot study. Here, we analyze factors influencing LIFT implementation.
Methods
We used a deductive-inductive hybrid qualitative approach to analyze transcribed meeting recordings from 55 technical assistance (TA) and 23 peer support (PS) calls with financial navigators (FN). First, we deductively coded all implementation-relevant content into the five domains of the Consolidated Framework for Implementation Research (CFIR). We then inductively generated themes and sub-themes within each of the CFIR domains. Coder reliability was assessed at multiple points during coding via coder consensus.
Results
The qualitative analysis of nearly 78 h of TA and PS calls with FNs resulted in 18 themes and 91 sub-themes across the six CFIR domains. Outer setting themes (7 themes, 37 sub-themes) included institutional workforce problems, limited organizational resources for specific needs, and the unpredictability of external resource application success. Determinants in the inner setting (3 themes, 18 sub-themes) included existing clinical infrastructure and navigators’ competing responsibilities in the clinic. Determinants in the individual domain (2 themes, 11 sub-themes) were the navigator workload and the patient motivation to engage in LIFT. Determinants in the innovation domain (2 themes, 5 sub-themes) were the intervention structure (ie, sequence and timing of LIFT activities). The most common implementation strategies (ie, process; 4 themes, 23 sub-themes) were pacing intervention content to meet patient needs, reframing the study to appeal to patients, and changing intervention delivery (eg, allowing phone visits).
Conclusions
This analysis highlights the challenges of implementing FN across multiple oncology sites, with workforce and administrative barriers being key challenges. Operational process data such as TA and PS calls can provide valuable information to guide implementation.
Plain Language Summary
Cancer-related financial hardship is common, and financial navigation (FN) interventions such as the Lessening the Impact of Financial Toxicity (LIFT) program aim to mitigate financial hardship. While LIFT demonstrated preliminary effectiveness in a single-site pilot, scaling to eight oncology sites introduced new implementation challenges. This study examined factors influencing LIFT implementation across sites using qualitative analysis of 78 hours of transcribed recordings from 55 technical assistance and 23 peer support calls with financial navigators. Guided by the Consolidated Framework for Implementation Research (CFIR), we identified determinants across five domains: Outer setting, inner setting, individuals, process, and innovation. Eighteen themes and 91 sub-themes emerged. Outer setting factors included workforce shortages, limited institutional resources for patient needs (eg, housing), and the unpredictability of external financial aid. Inner setting factors involved existing clinical infrastructure and navigators’ competing clinical responsibilities. Individual-level factors included navigator workload and patient motivation to engage. Innovation-related factors centered on the structure and timing of LIFT activities, while process-related determinants included pacing intervention delivery, reframing LIFT to align with patient needs, and adapting delivery methods (eg, phone visits during COVID-19). Overall, findings highlight the breadth of implementation challenges when implementing financial navigation across multiple sites. Routine analysis of operational data can inform ongoing program tailoring and enhance financial navigation implementation in oncology care.
Introduction
As a result of high cancer care costs and a growing share of costs being shifted to patients and families, a substantial portion of cancer survivors report financial hardship (50%-70%).1,2 The consequences of high out-of-pocket costs are often discussed in relation to three domains of financial hardship, each representing a unique impact on the well-being of survivors: material (eg, out-of-pocket costs, inability to pay bills), psychological (eg, stress or worry about being able to pay bills), and behavioral (eg, cost-related delayed or foregone care). 1 Beyond reducing access to care and causing financial stress, financial hardship among cancer survivors has also been associated with worse mental health outcomes, increased symptom burden, and an increased risk of mortality.3,4,5,6
In a recent scoping review, approaches to addressing financial hardship were categorized into two categories: real-world programs (eg, pharmacy-based medication assistance) and research-based interventions (eg, financial navigation). Across approaches, interventions and programs showed promise in decreasing overall financial hardship, decreasing appointment no-shows, and increasing enrollment in clinical trials. 7 One such research intervention was the Lessening the Impact of Financial Toxicity (LIFT) study—a single arm financial navigation trial conducted by the authors of this manuscript. 8 In its pilot, LIFT was implemented at one institution and demonstrated promising preliminary effectiveness, significantly reducing financial hardship from pre-to post-navigation. 8 The larger LIFT trial was a Type II implementation-effectiveness hybrid design implemented across eight sites in North Carolina. 9 Due to the increased complexity of implementing across eight clinical sites, a priori implementation strategies were deployed alongside LIFT, including training, mapping workflows, and hosting technical assistance (TA) and peer support (PS) calls with financial navigators. TA and PS calls were meant to be used to address implementation barriers at specific sites and then share strategies for addressing challenges with other site financial navigators.
The purpose of this qualitative analysis was to leverage existing operational process data collected throughout the LIFT Hybrid II Trial (ie, recordings of TA and PS calls with financial navigators) to describe common implementation determinants of the LIFT intervention across eight sites in North Carolina. This study provides important insight into the implementation of financial navigation—crucial for moving towards sustainable and scalable financial navigation in oncology clinics.
Methods
Lessening the Impact of Financial Toxicity (LIFT) Intervention
Site Characteristics of Oncology Practices That Implemented the LIFT Intervention (N = 8)
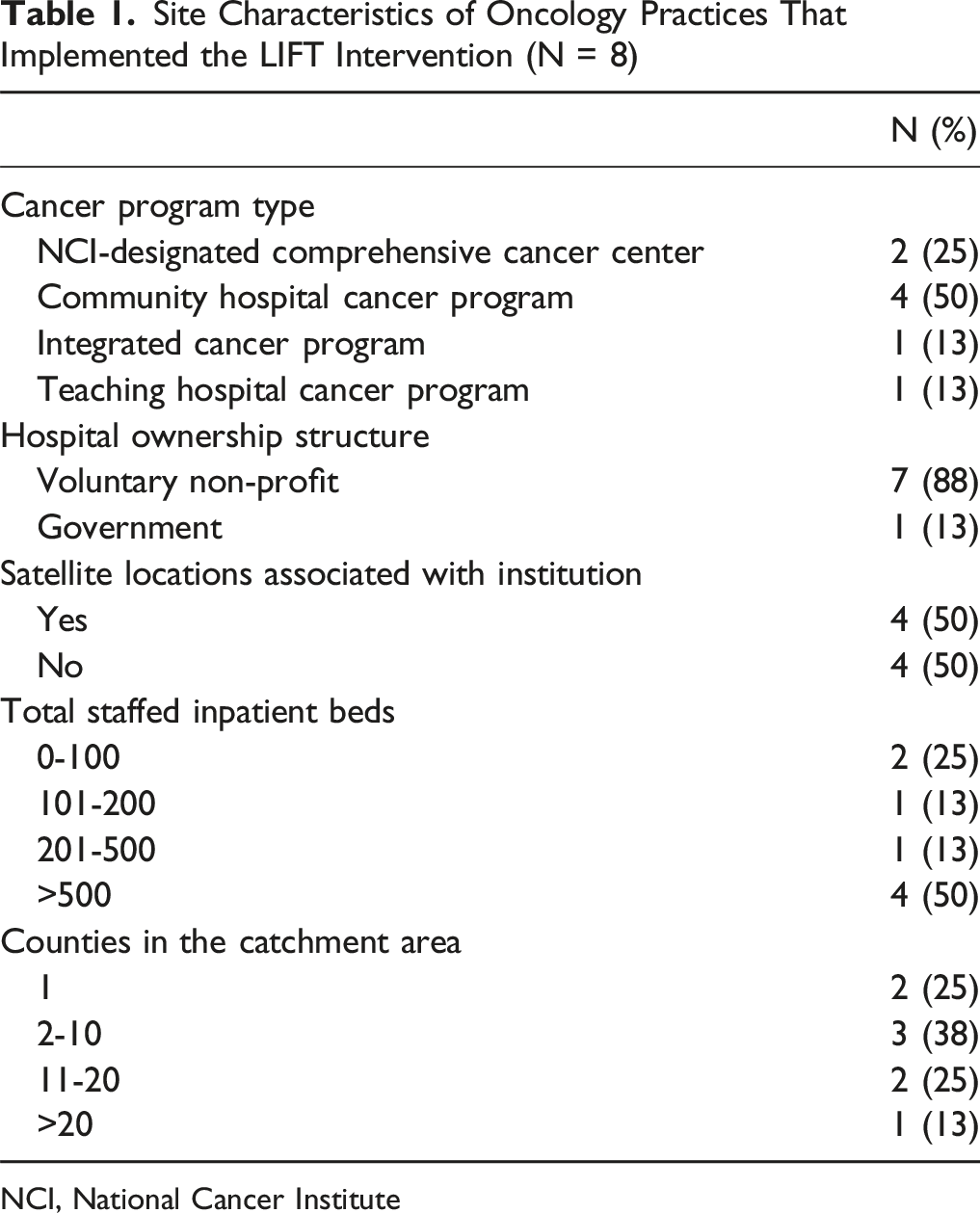
NCI, National Cancer Institute
The LIFT intervention consisted of two primary functions: (1) Systematically assessing patient-reported cost-barriers and (2) Addressing patient-reported cost barriers through allocation of resources and application assistance. Patients were eligible for LIFT if they were at least 18 years of age, had received a cancer diagnosis or disease progression within the last five years and/or living with advanced disease, spoke English, and reported financial toxicity. Financial toxicity was measured using the COmprehensive Score for financial Toxicity (COST), which consists of 11 Likert scale questions and yields scores ranging from 0-44, with lower scores indicating worse financial toxicity. Participants with a COST score ≤22 (indicating moderate-to-severe FT) at consent were eligible for LIFT.10,11 A detailed study protocol has been published elsewhere. 9
Each LIFT site dedicated at least a 0.5 full-time equivalent (FTE) of 1-2 existing employees to be trained as LIFT FNs. Existing employee roles included nurse navigators, patient navigators, and social workers. FNs received 17 h of training on both identifying and addressing cost barriers as well as study protocols. Training was provided by external organizations (eg, Association of Cancer Care Centers Financial Advocacy Boot Camp) as well as LIFT study team members. As part of LIFT, FNs received access to a comprehensive case management system built in REDCap that was used to conduct a comprehensive in-take, track patients throughout the navigation process, and administer pre- and post-surveys.
Data Collection
Throughout the trial, the LIFT study team consistently met with FNs from each site. Two types of meetings were conducted (a priori implementation strategies) including (1) Technical Assistance (TA) meetings and (2) Peer Support (PS) meetings. TA calls included LIFT study team members and FNs from one site per call. The purpose of the TA calls was to provide site-specific updates and discuss the details of specific implementation challenges and engage in collaborative problem-solving. PS meetings included LIFT study team members and all FNs from sites that were preparing to or already recruiting patients into the trial. The purpose of the PS meetings was to share best practices/lessons learned, discuss common implementation barriers and solutions (often from TA calls) in an open forum, and create community among LIFT FNs. Over the course of the trial, 78 implementation meetings with FNs occurred (TA: N = 55, 70.5%; PS: N = 23, 29.5%) totaling just under 78 hours of meeting content. All TA and PS calls were recorded and transcribed (either live via Zoom transcription or by a third-party transcription service [eTranscription Solutions]). TA and PS calls were not originally recorded with the intent of analyzing the meeting content, therefore financial navigators were not consented. However, the overall implementation evaluation of LIFT was approved by the University of North Carolina Institutional Review Board (#20-1997). In order to protect the privacy and confidentiality of the navigators, quotes were not provided in this manuscript.
Theoretical Grounding and Qualitative Analysis
A deductive-inductive hybrid qualitative analysis was conducted on all 78 transcripts from both TA and PS calls. 12 Content analysis was conducted by the analytical team (ARW, MM, CRM, KP) and was guided by the Consolidated Framework for Implementation Research (CFIR) 2.0. 13 Two cycles of qualitative coding were used to first deductively sort content into the five domains of CFIR (ie, outer setting, inner setting, individuals, innovation, and process). We then inductively analyzed the content within each domain.
First-cycle coding began with data immersion and CFIR training led by ARW and guided by SBW. Each member of the analytic team read through at least five meeting transcripts and familiarized themselves with CFIR. The analytic team then co-created a visual codebook of how the five domains of CFIR were being conceptualized in the context of LIFT (Figure 1). Each member of the analytic team then coded four transcripts into the five domains of CFIR in Dedoose. During the deductive coding, the analytic team met to discuss how codes were being applied and reviewed every code applied to the initial 20 transcripts (25.6% of transcripts) to maximize inter-coder reliability.14,15 During the process of reviewing code applications, the codebook was refined and consensus on how codes were being applied was achieved. Analytic decision points were documented throughout consensus meetings. The remaining transcripts were then divided amongst the analytic team and coded into the five CFIR domains. Visual codebook for deductive coding of technical assistance and peer support calls from the implementation of an eight site financial navigation intervention—LIFT
An inductive thematic approach was taken during second-cycle coding to account for themes not represented within CFIR domain constructs. The analytic team conducted an inductive content analysis creating themes within each CFIR domain. To begin the process, the analytic team read through all excerpts coded into a CFIR domain and formulated preliminary themes. Up to 20% of excerpts coded into the CFIR domain were coded into the newly generated themes by an analytic team member.14,15 Application of codes was reviewed by the analytic team, and themes and definitions were refined during study meetings. Once coder consensus was reached on how theme codes were being applied, the remaining excerpts were divided amongst the analytic team to be coded. 15 This process was repeated for each CFIR domain. The findings were then summarized by the study team focusing on both the most frequently coded domains and themes as well as the themes that were deemed important by the study team based on the content of the excerpts. To maximize the applicability of the findings of this study on future implementation of financial navigation, during the analytic process study, specific themes pertaining only to the research study itself (eg, IRB delays) were excluded from the findings reported here.
Once all excerpts were coded, frequencies tables for each theme and sub-theme were generated, and trend lines were fit for frequency of sub-themes by months since site-specific and overall LIFT initiation. Frequency and linear trends were also calculated for the number of TA calls by months since LIFT initiation.
Data were quantified due to the high volume of implementation-related discussions across the implementation of LIFT and the tendency for important or hard to address implementation challenges to be discussed at multiple meetings across time. 16 Quantification of big qualitative data has shown to minimize researcher bias when dealing with a larger number of concepts or themes, however such methods are not often applied in the implementation science setting. 16 Furthermore, the purpose of the TA and PS calls was to assess the current implementation challenges of LIFT rather than probe FNs about their experiences implementing LIFT—resulting in frequencies of each theme and sub-theme that proxies qualitative strength (ie, intensity or importance).
Results
A total of 78 implementation meetings occurred with LIFT FNs. The number of TA and PS meetings attended was dependent on the date of initiation for each site, which occurred from November 2021 to September 2023. There were, on average, two TA calls per month and one PS call every other month.
Consolidated Framework for Implementation Research (CFIR) Domains, Themes, Sub-Themes, and Themes of Implementing LIFT in Eight Oncology Sites

Themes and sub-theme percentages were calculated with respect to the total number of codes in that CFIR domain. CFIR domain percentages were calculated with respect to the total number of codes.
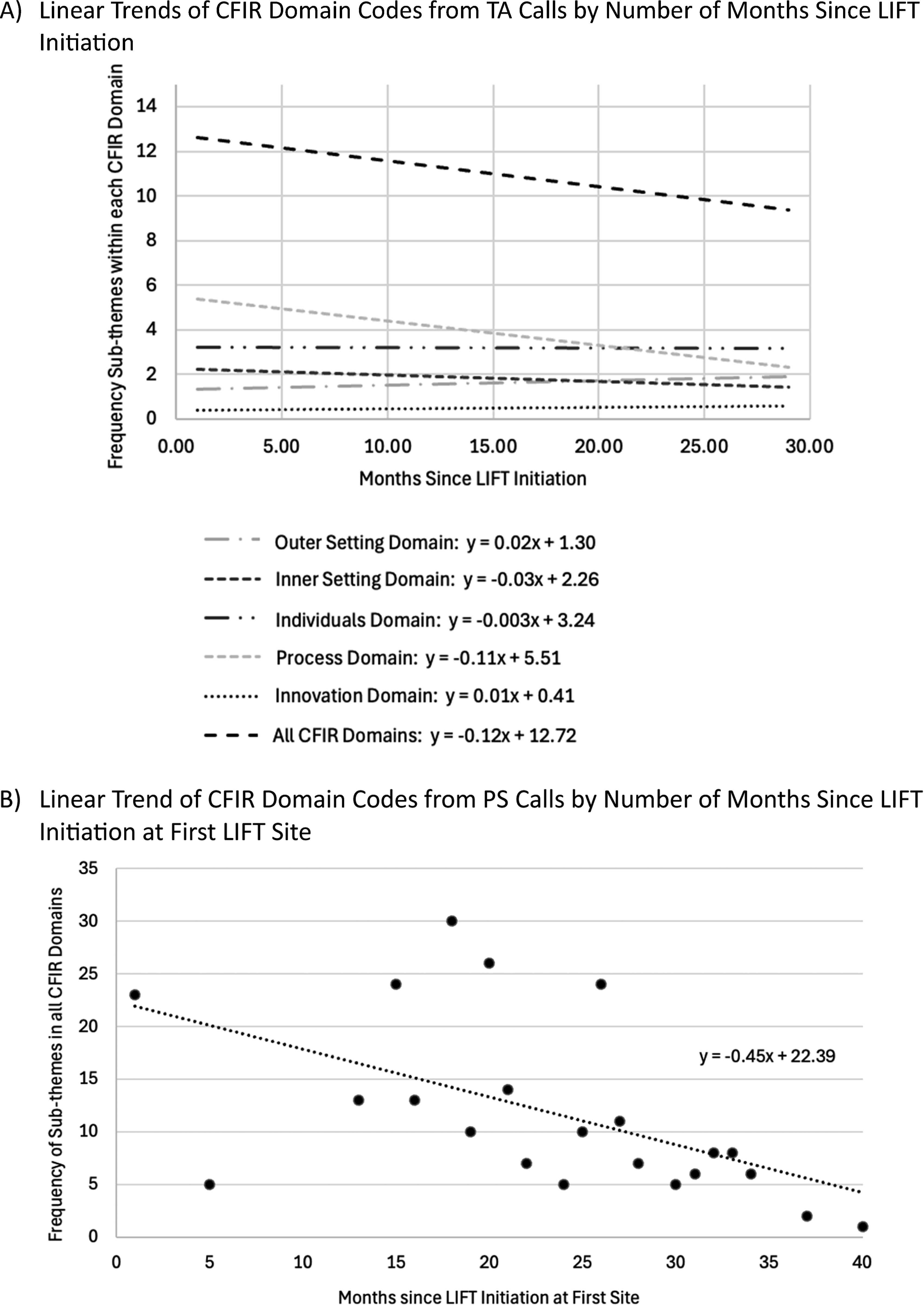
Linear trends of implementation determinant sub-themes from technical assistance (TA) and peer support (PS) calls for the implementation of LIFT
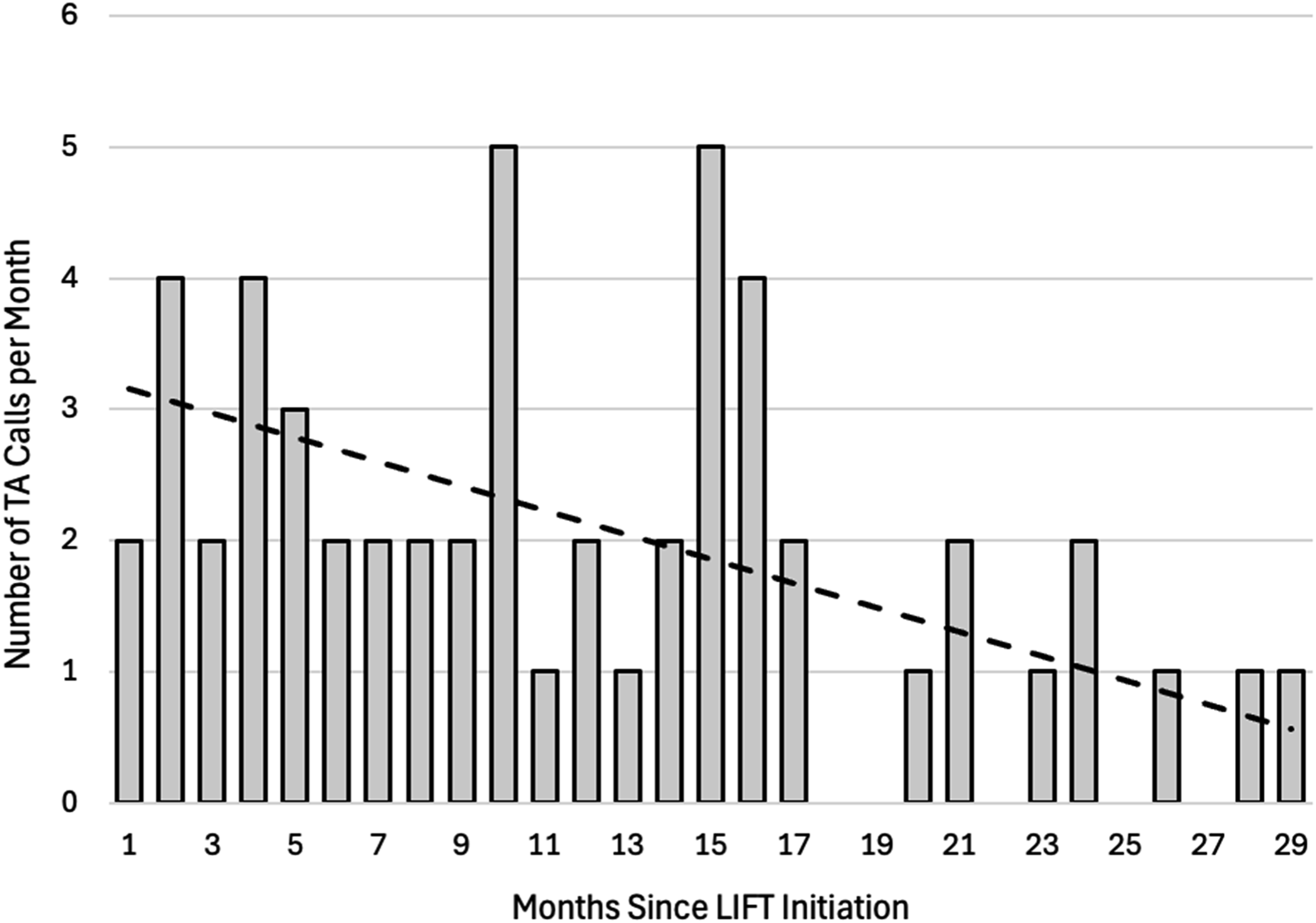
Frequency of technical assistance calls by months since LIFT initiation and freq
Outer Setting
Consolidated Framework for Implementation Research Domains, Themes, Sub-Themes, and Frequencies of Implementing Financial Navigation in Eight Oncology Sites

Themes and sub-theme percentages were calculated with respect to the total number of codes in that CFIR domain. CFIR domain percentages were calculated with respect to the total number of codes.
Within the theme of accessing and navigating financial aid and health insurance, FNs frequently discussed the challenges associated with the variability of wait times for benefit determination. Such variability in wait times made it difficult to implement LIFT as FNs were unable to give patients a timeframe of when to expect aid. Within the health systems theme, FNs most frequently discussed labor shortages within their systems, including high rates of turnover, and COVID-19-related hiring freezes and restrictions on volunteer interactions with patients. The workforce issues in this category were viewed by FNs as a health system issue that hindered implementation—including health systems not prioritizing the role of social work or restricting hiring. Within the limited financial aid and complex systems themes, FNs frequently discussed a dearth of resources for specific needs (eg, housing) that limited their ability to help some patients. Across the outer setting domain, themes and sub-themes most were described by FNs as barriers to implementation, with the exception of Medicaid expansion in North Carolina and the presence of institutional resources, which were both viewed as facilitators of implementation.
Inner Setting
Three themes and 18 sub-themes were created for implementation determinants in the inner setting (Table 3). FNs most frequently discussed determinants revolving around financial navigation as a clinical role (42.5% of inner setting codes). Within the clinical role theme, FNs commonly discussed the implementation of LIFT being challenging in the context of competing responsibilities—FNs in LIFT were only 0.5 FTE on the study but often continued to be responsible for their prior full-time responsibilities. Furthermore, FNs discussed how social work team structures both facilitated implementation (eg, systems to work with patients on social needs) and were a barrier to implementation (eg, understaffing). FNs discussed the two other themes at roughly the same frequency, including the fit and prioritization of financial navigation in the clinic (28.4%) and clinical systems that impact the implementation of LIFT (29.3%). When discussing the fit and prioritization of financial navigation, FNs commonly discussed financial navigation as a good fit with the clinical structures and how they interact with patients; however, FNs did share that they felt that there was a lack of awareness among providers and other staff in their clinics about LIFT and the services they could provide. In the context of clinical systems that impacted LIFT, FNs frequently shared existing clinical systems that facilitated the implementation of LIFT including support groups, lists of uninsured patients to approach, newsletters, and distress screening. Less commonly discussed, but important to the implementation of LIFT, FNs also discussed instances where LIFT did not align well with existing financial assistance and charity care programs within their system as well as challenges surrounding fitting LIFT into the clinic flow (eg, when to approach patients and where).
Individual
Two themes and 11 sub-themes were created within the individual CFIR domain (Table 3), one theme for each of the primary roles involved in the implementation of LIFT—the FNs and the patients. Of all codes, 26.0% were coded into the individual CFIR domain, with most (64.9% of individual codes) focused on the patients receiving LIFT. Within the theme focused on patients, FNs most discussed the need for LIFT by discussing the financial needs of patients and their motivation to engage with LIFT. FNs also frequently discussed patients feeling overwhelmed or overloaded with information near diagnosis and expressed concern that approaching them to discuss LIFT added to that feeling of overwhelm. The FN intervention required information sharing about patients’ personal finances, and FNs reported that some patients felt uncomfortable sharing financial information, citing distrust of the government or not wanting “a handout.” Within the theme focused on the FNs themselves, FNs often discussed having a tremendous workload with LIFT and their other job responsibilities. However, FNs typically discussed their workload in the context of their capability and motivation to engage with patients about their financial needs.
Innovation
Within the innovation CFIR domain two themes and five sub-themes were created (Table 3). Discussion of LIFT itself was the least frequently discussed CFIR domain (5.3% of all codes) and encompassed two themes. The first theme focused on how to refer patients to the Patient Advocate Foundation (PAF) if LIFT FNs could not address the needs of the patient. The second theme focused on the structure of LIFT itself, most commonly FNs discussed the structured nature of LIFT facilitating the implementation and providing suggestions to improve the implementation of LIFT (eg, proposing the study as session-based or time-limited to patients).
Process
The process CFIR domain was the most frequently discussed domain (41.0% of all codes), consisting of 4 themes, 23 sub-themes. The process domain focused broadly on what the FNs and LIFT study team were actively doing to address the implementation challenges that they faced throughout the study period. The most frequently discussed process CFIR domain themes were tailoring and adapting delivery of LIFT (41.4% of process codes) and building FN capacity (25.1%).
When discussing tailoring and adapting the delivery of LIFT, FNs often discussed changes in delivery mode to facilitate meeting patients “where they were” emotionally or physically. Specifically, this entailed changes in delivery mode from in-person to phone-based or via videoconferencing—either in response to patient need (eg, patient felt ill or overwhelmed) or in response to health system mandates amid the COVID-19 Public Health Emergency. FNs also frequently discussed changes to how the intervention was paced, mostly focused on asking patients to complete only the portions of the study (eg, consent, screening, financial intake, pre-questionnaires) they were feeling up to in the moment. While less frequently, FNs also discussed aligning LIFT follow-ups with clinical schedules and providing general education and support to patients (though complementary, these were not explicitly part of the intervention).
When discussing building FN capacity, FNs frequently discussed their use of the tracking and data management systems. These discussions often centered on their experiences using the system and providing tips and tricks to other FNs. Some FNs also discussed the need for technology training to increase their comfort with using the REDCap tracking system. Less frequent process CFIR domain themes included integrating and adapting LIFT into clinics and attempting to adjust to policy and organizations. When discussing fitting LIFT into their clinics, FNs often discussed aligning their adaptations (eg, mode of delivery, pacing of intervention) to LIFT to the clinic workflow. These adaptations worked in harmony with the adaptations that were carried out to meet the needs of the patients. Importantly, FNs also shared that implementation barriers were reduced when engaging with other internal financial assistance providers such as charity care and copay assistance in the pharmacy. In the context of attempting to adjust LIFT to policy and organizations, FNs often discussed reframing the study components (eg, consent language) when communicating with patients to ensure that it was clear LIFT would be able to assist them and would not share identifiable information with the external individuals or organizations. FNs also discussed challenges trying to adapt the intervention in the context of long benefit determination wait times (eg, Medicaid) and building relationships with external financial aid organizations to streamline aid/benefit determination.
Discussion
Findings from this qualitative analysis highlight the variety of implementation determinants associated with conducting a large financial navigation trial (ie, LIFT) across eight sites. While we were unable to fully disentangle determinants driven by study procedures vs financial navigation itself (for example, the administrative burden imposed on site staff associated with IRB approval), study-specific determinants were excluded from this manuscript—thus, this manuscript highlights only those determinants relevant to the real-world implementation of financial navigation in diverse oncology settings. Applying CFIR, our findings showed that the outer setting contained the highest variety of determinants, while determinants within the individual and process domains were the most frequently discussed during TA and PS calls. Common themes in the individual and process domains included themes focused on the patient, the financial navigator, tailoring delivery of LIFT, and building financial navigator capacity. Recognizing and addressing the challenges and successes identified by financial navigators in real-time throughout implementation vs retrospectively is a crucial step toward the scalability and sustainability of future financial navigation efforts.
The breadth of the determinants discussed during TA and PS calls throughout the implementation of LIFT is generally more expansive than what has been reported in the financial navigation implementation literature previously. 17 This finding in context suggests that TA and PS meetings serve an important role in identifying and addressing implementation challenges in real-time and serve as an innovative data source. While this study did not seek to directly assess the effectiveness of TA and PS calls, a recent scoping review revealed that most studies that measured the impact of TA on implementation reported a positive association between assistance provided and implementation success. 18 While unintentional, LIFT site initiation was staggered over time, however, the linear trends findings of consistent decrease in CFIR determinants discussed over time suggests that PS calls may serve as an effective mechanism to share successful implementation strategies developed on TA calls with new sites. Overall, the findings of this study suggest that using operational process data could be an effective way to contribute to the understanding of implementation when paired with quantifiable implementation outcomes and retrospective qualitative data collected with the purpose of understanding implementation. Quantifying operations data has the potential to highlight commonly discussed implementation challenges even when those challenges are not necessarily the challenges that stick out as important to implementers.16,19
Workforce-related issues were identified across multiple CFIR domains, creating a consistent thread throughout the TA and PS calls. Reported concerns included understaffing, competing responsibilities, and hiring restrictions. These issues are not unique to the LIFT implementation, however, are reflective of broader concerns related to behavioral workforce shortages. 20 Calls to address these concerns have centered on an alignment of training, regulation, and payment policies, but progress in this regard is often incremental and heavily influenced by funding allocations and political consideration. 21 Although there have been promising developments in policy (eg, allowing Medicare reimbursement of navigation in patients with serious illness), targeted navigation programs like LIFT would be ineligible for these payment policies and thus must rely on alternative sources of support. 22 This finding suggests a need for cost-effectiveness analyses and other business case analysis for financial navigation.
Within the individual, outer setting, and inner setting domains, findings from this analysis reinforce recent work to illustrate the profound complexity of the financial aspects of healthcare system and the resulting administrative burden. In this analysis, FNs reported unpredictable benefits, lengthy and detailed applications for assistance, and limited available resources, mirroring the harmful impact of fragmented health systems on patients. 23 Recent literature has demonstrated that patient administrative burdens (eg, finding in-network providers, prior authorization, and paying bills) are associated with delayed or foregone care and non-adherence with prescription medications.24,25 These findings suggest that a major function of financial navigation is not only reducing cost-related barriers to care but also minimizing the financial-related administrative burden shouldered by patients. Future inquiry should assess the impact of financial navigation on patient and caregiver administrative burden.
Finally, the findings of this analysis suggest several potential recommendations for implementing financial navigation into the oncology setting. First, throughout the initiation of the LIFT trial we assessed the clinical context, workflows, and organizational readiness.26,27 This pre-implementation work facilitated a site-specific implementation that was continuously tailored throughout the trial. Continuous context-specific adaptation and tailoring is crucial for the development and implementation of responsive and scalable financial navigation programs. Finally, consistent engagement with financial navigators to reassess and address implementation barriers is a crucial component of multi-site oncology financial navigation.
Limitations
This study should be interpreted in the context of certain limitations. First, TA and PS calls focused on the implementation challenges brought up by the FNs and study team throughout the implementation of LIFT but were not structured to elicit discussion on any specific topic or CFIR domain. Furthermore, the nature of TA and PS calls, focusing on addressing implementation challenges, likely led to more discussion of process in comparison to other CFIR domains. The ability to attend TA and PS calls relied on not being too overloaded and therefore this analysis likely underestimates some workforce and role clarity challenges. While discussing implementation, FNs often talked about LIFT as both the financial navigation intervention and study-related tasks that influenced implementation—which were unable to be completely separated for analysis.
Conclusions
Overall, the findings from this analysis highlights the complexity of implementing FN into oncology care—particularly across multiple sites. During TA and PS calls, there was a large breadth of implementation topics discussed within each CFIR domain. However, overall, the frequency of implementation discussions during calls decreased over time. Our findings highlight major workforce and administrative barriers faced by FNs while implementing LIFT. Finally, operational process data may serve as an innovative and important source of implementation data when paired with quantifiable implementation outcomes and retrospective qualitative interviews/focus groups focused on implementation.
Footnotes
Ethical Considerations
Analysis of operations data reported in this study were approved by the University of North Carolina Institutional Review Board (#20-1997).
Consent to Participate
Financial navigators did not consent to participate as meeting recordings were not originally intended for research purposes.
Author Contributions
Conceptualization: ARW, SBW; Methodology: ARW, SAB, SBW; Validation: ARW, MLM, CRW, SBW; Formal analysis: ARW, MLM, CRW, KP; Data curation: MLM; Writing – original draft: ARW, MLM, CRW, BT; Writing – review & editing: ARW, MLM, CRW, BT, KP, AMP, MG, NP, SAB, DLR, SBW; Visualization: ARW; Supervision: SAB, DLR, SBW; Project administration; MLM, MG, NP; Funding acquisition: DLR, SBW.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health, National Cancer Institute under the award numbers R01CA240092 (PIs: Wheeler, Rosenstein), T32CA092203, and T32CA116339.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analyzed in this study may be available from the corresponding author upon reasonable request.
Disclaimer
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.