
Abstract
Introduction
Cancer-related financial hardship is pervasive, impacting both patients and caregivers, making it crucial to address financial hardship at the household level. The CREDIT (S1912CD) study was designed to enroll and randomize cancer patients and spousal caregivers as dyads to proactive financial navigation compared to usual care. The study faced several challenges to recruitment. This paper discusses the changes made to successfully complete the study.
Methods
The study took place among NCI Community Oncology Research Program (NCORP) sites and allowed several venues for protocol feedback, including SWOG group meetings, NCORP administrator meetings, and individual calls with recruiting sites. A patient advocate worked with the study team to review and update documents to ensure the study was relevant and accessible to potential participants.
Results
Several barriers were identified including sites facing challenges in enrolling patient-spouse dyads, multiple financial navigation partners causing confusion and delays in delivery of the intervention, eligibility criteria concerns, and participant discomfort with providing social security numbers. Several modifications were made to address these obstacles during a study restructure, including making caregiver participation optional, streamlining intervention delivery, and modifying eligibility criteria to allow more time between diagnosis and enrollment. Changes from the restructure resulted, on average, in a 9.5 patient per month increase in accrual (4.1 to 13.6) and has enabled the study to reach overall accrual within the study timeline. Importantly, the study maintained diverse accrual and continued to accrue willing caregivers to enable exploratory analysis of caregiver outcomes.
Conclusion
Interventions examining how to mitigate financial hardship for cancer patients and those affected by cancer, must be pragmatic in order to be translated into sustainable programs in real world settings. Providing recruiting sites an avenue for feedback ensured that the study team could adjust the protocol to meet site needs and successfully complete this financial navigation study.
Keywords
Introduction
At least 30-50% of cancer patients in the United States face major financial hardship as a consequence of treatment, adversely impacting their quality of life and survival.1-3 Spouse and partner caregivers of cancer patients, in addition to sharing in the increased medical costs that come with treatment, also report lost income due to time taken off of work to help perform caregiving duties.4-9 Spousal caregivers are particularly vulnerable to financial hardship given that they typically share household income, assets and expenses with patients.10,11 A recent systematic review has shown a body of growing evidence supporting financial navigation as a tool to mitigate financial hardship and improve patient and caregiver outcomes. 12 Given the impact of cancer-related financial hardship at the household level it is critical to develop and test interventions targeted at reducing household financial hardship.
The CREDIT study (A Randomized Trial Addressing Cancer-Related Financial Hardship Through Delivery of a Proactive Financial Navigation Intervention; S1912CD) was activated on July 26, 2021. This prospective randomized controlled trial was designed to evaluate whether a proactive financial navigation program helps cancer patients, and their spousal caregivers understand and manage the financial aspects of cancer care to avoid financial hardship and downstream adverse effects on health and well-being. The study was initially designed to enroll cancer patient/spouse caregiver dyads to receive either financial literacy training alone (control) or financial literacy training alongside financial counseling from two partner organizations (intervention).
Despite the importance of designing and evaluating trials aimed at improving financial well-being for both cancer patients and their spousal caregivers, recruitment was initially very slow. The study team pivoted by implementing necessary changes to successfully meet accrual goals. This paper describes the process of soliciting feedback from study collaborators, implementing study changes, and the impact of these changes on the scientific endpoints and enrollment to the study. We believe that our experience will help to inform other researchers embarking on similar studies, particularly those involved in research aimed at addressing healthcare-related financial hardship.
Methods
Study Setting
The CREDIT study setting was the National Cancer Institute Community Oncology Research Program (NCORP) which brings cancer care delivery research to community oncology clinics across the US. The NCORP network is comprised of 7 research bases and 46 community sites, 14 of which are designated as Minority/Underserved (M/U) community sites. 13 NCORP is an ideal setting for a financial navigation study as the diverse populations and range of clinical settings make findings highly generalizable. The SWOG cancer research center oversees recruitment and data collection for the study.
Initial Study Design
CREDIT was designed as a dyadic prospective randomized controlled trial of cancer patients and their spousal caregivers. While the study team acknowledged that non-spousal caregivers may also face financial hardship following a patient’s cancer diagnosis, a decision was made in the initial study design to focus on spousal caregivers due to evidence that spouses of cancer patients can experience poorer quality of life, depression, and high caregiver burden as compared to non-spousal caregivers,14,15 and due to the unique financial interconnectedness between patients and their spouses. Additionally, dyadic involvement may facilitate joint learning and use of the navigation and financial literacy materials. The study team hypothesized that successful interventions implemented at the household level may result in improvement in financial, psychosocial, and clinical outcomes for both patients and their spouses, a two-for-one benefit.
Cancer patients were eligible if they were within 120 days of a diagnosis of a metastatic solid tumor or hematologic malignancy and were receiving or planning to receive anti-cancer treatment. In addition, patients were required to provide their social security number (SSN) at registration (to access credit reports for the study outcomes) and to provide a phone number or email address so that our financial navigation partner organizations could contact participants. Spousal caregivers were required to live in the same household as the patients and be legally married or in a common law marriage. Caregivers were also required to provide a SSN and contact information. All participants were required to speak either English or Spanish.
Financial Literacy Video Topics.
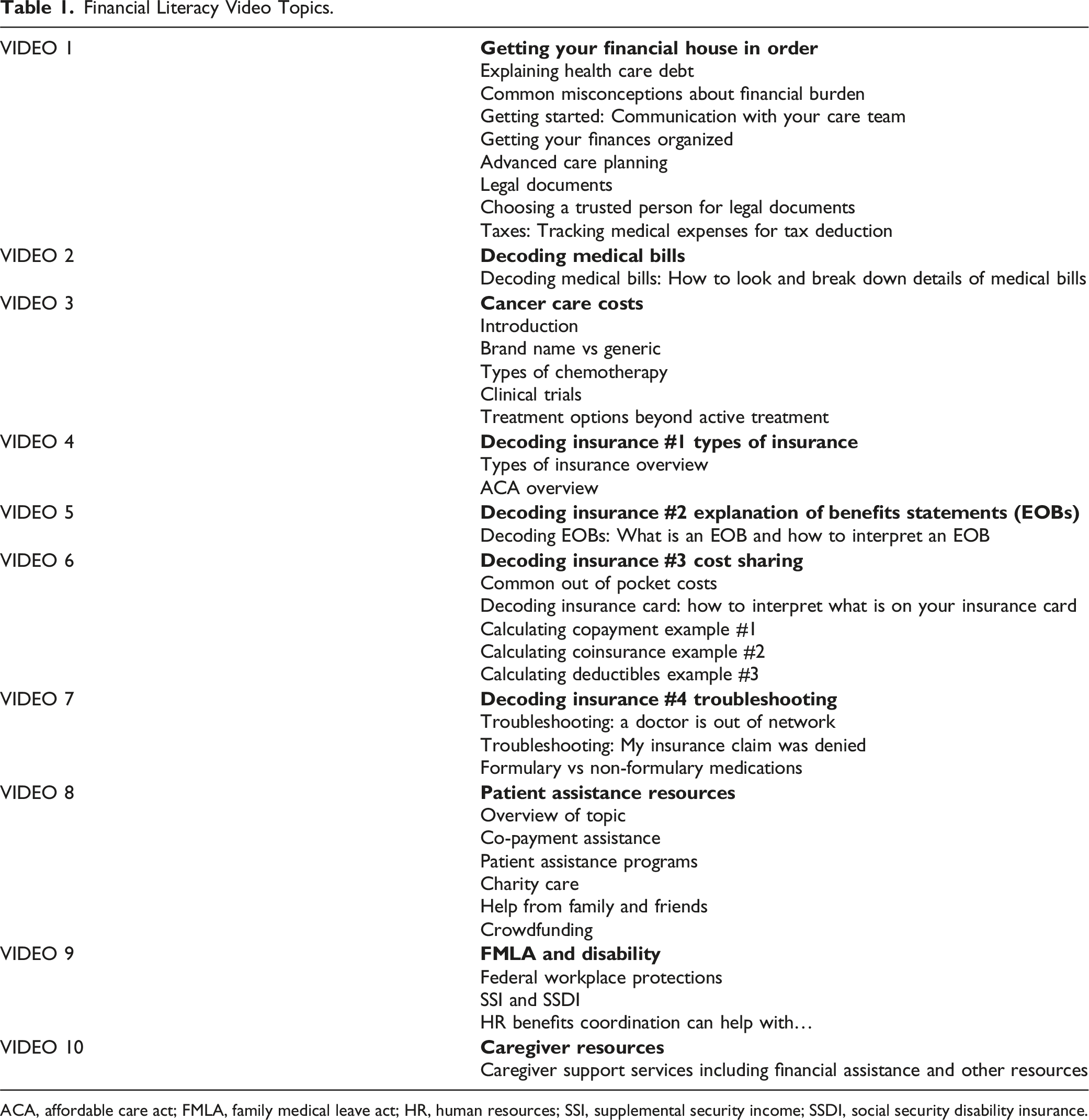
ACA, affordable care act; FMLA, family medical leave act; HR, human resources; SSI, supplemental security income; SSDI, social security disability insurance.
Financial Navigation Program Components.

CENTS, consumer education and training services; OOP, out of pocket; PAF, patient advocate foundation; VA, veterans affairs.
Intervention arm dyads participated in monthly sessions with CENTS and PAF for 6 months. Both patient and spousal caregiver were expected to participate together in the initial and final session with each organization. Attendance from both partners for the other monthly sessions was up to their discretion. All sessions could be completed over phone or videoconference. After the initial session, financial navigation could also occur over email. The study aimed to enroll 536 patient/spouse dyads over 2.5 years and targeted a 40% relative reduction in household financial hardship from 30% down to 18%. Household financial hardship was defined as one or more of the following from the patient’s and/or spouse’s credit report within 12 months: any new loans (bank or home equity); exhausting lines of credit by reaching limits on credit cards and home equity loans; credit or other payment delinquencies; becoming subject to a lien, judgment, or other collection process; personal bankruptcy filings. Credit reports have been used in past financial hardship studies, 18 and were chosen to measure the primary outcome as they provide objective and reproducible measures of financial hardship.
Soliciting Protocol Feedback
NCORP sites were encouraged to provide feedback to the study team on barriers to implementation of the CREDIT study. These were done through one-on-one calls with participating sites, the bi-annual SWOG group meeting through study-specific meetings and the Cancer Care Delivery (CCD) Committee meeting, monthly CCD calls, and NCORP administrator webinars. Feedback was documented and discussed by the larger study team and changes were implemented to the protocol to ensure sites, particularly M/U NCORP sites, were able to participate in the study. Additionally, the study had a patient advocate who worked with the study team to review documents, ensure the study was meaningful for patients, craft language on how to discuss the study with potential participants, and identify potential modifications alongside the study team to ensure study success.
Results
Identified Barriers
Sites identified several barriers to CREDIT study enrollment, primarily the ability to identify and enroll dyads. Other challenges sites identified included: confusion and delays with multiple financial navigation partners; restrictive eligibility criteria; and the need to collect a SSN.
Dyadic Enrollment
Sites reported numerous challenges with identifying and enrolling dyads to the study, particularly dyads that needed to be legally married and/or filing taxes jointly. There is no systematic way to screen marital status through the electronic health record, which made the screening process time-intensive and led to site staff having to conduct uncomfortable conversations with patients regarding partner status to see if they met eligibility criteria. In addition, M/U NCORP sites reported that many patients are not in traditional marriage/spousal relationships. Lastly, the patient may be interested in the study, but the partner may not be and thus this dyad was ineligible.
Intervention Delivery
After consent, delays occurred in starting the financial navigation, with some participants reporting confusion due to working with two separate financial navigation partners (CENTS and PAF). Both sites and our financial navigation partners reported that dyads were unable to start the financial navigation in a timely matter as it was challenging to find times that both the patient and spouse were available for initial calls or videoconferences with the partners. It was also time-consuming to participants to have to speak to multiple organizations. Additionally, participants were confused about being contacted by two different organizations and did not understand the difference between them.
Eligibility Criteria
Two challenges were identified with the cancer eligibility criteria. The first challenge related to the allowed time from diagnosis (120 days). Clinical research associates at several sites reported that patients within 120 days of a metastatic diagnosis were still overwhelmed with issues related to their disease and treatment and therefore not open to participating in non-treatment trials. Additionally, due to the broad cancer eligibility criteria, sites reported discrepancy among disease group enrollments, with some groups aware of the study and actively recruiting while other groups were not. Recruitment often relied on a disease group having a “study champion” who highlighted the study in their disease group research meetings.
Data Collection
Another challenge identified by sites, particularly rural sites, was the need to ask participants for a SSN. Sites reported that participants felt a general distrust in providing their SSN and concern that their data could be compromised. Additionally, collecting SSN excluded many undocumented patients from minority groups from participating, a significant demographic of some of our minority/underserved sites.
Solutions Implemented
Dyadic Enrollment
In response to concerns over dyadic enrollment, our team initially amended the protocol in July 2022 to allow for non-spouse but live-in significant other/partners to be eligible, but still required that both parties enroll as a dyad. While this improved enrollment to a small extent, sites still had challenges in enrolling dyads.
Eligibility Criteria Changes.

Intervention Delivery
An additional change implemented in the restructure was to reduce our financial navigation partners from two to one, and to relax requirements for participation in the monthly sessions. After the restructure, PAF became the sole organization to deliver the financial navigation intervention and expanded their services to include financial literacy and social needs navigation, which were previously being delivered by CENTS. PAF was able to consult with CENTS as needed if pertinent for specific participants. Additionally, the protocol dropped the requirement that dyads participate in any calls together- allowing flexibility for patients and caregivers to participate when available and most convenient in their schedule(s). PAF tracked who was engaged in monthly navigation sessions, topics discussed, and any outcomes.
Eligibility Criteria
A protocol modification was developed to change the window of time from diagnosis from 120 days to 180 days. This allowed sites more flexibility in approaching patients for this study when they were further out from diagnosis and more receptive to participation in a financial study. One participating site (University of New Mexico Comprehensive Cancer Center (UNM)) addressed the issue of broad eligibility criteria by identifying study champions in each of the multiple disease groups to broaden awareness and enrollment of this trial across their cancer center. UNM presented changes made to their study approach at multiple NCORP forums including the SWOG group meeting and NCORP administrative staff meeting, allowing other sites to learn best practices from a high performing M/U NCORP site that was able to increase their CREDIT enrollment.
Data Collection
Given that the primary endpoint for the CREDIT study is tied to credit reports, the study team has been unable to change the requirement of study participants to provide SSNs. To address participant concerns, the study team did acquire a letter from the credit reporting agency (TransUnion) that explains credit pulls for the purpose of the study are soft credit pulls that do not impact participant’s credit scores in any way. The letter is available in English and Spanish for sites to provide to study participants (Supplemental File 1).
Impact of Changes
Impact on Scientific Endpoints, Sample Size, and Accrual Goals
The restructure of the study changed our primary endpoint from household financial hardship to patient financial hardship using credit report data. In the original study design, the study targeted a 40% relative reduction in household financial hardship from 30% down to 18%. With the modified eligibility criteria allowing enrollment of single patients who, due to lack of caregiver support, may derive an even greater benefit from proactive financial navigation, the target reduction in financial hardship was from 30% to 15%, a 50% relative reduction. This change impacted the overall sample size, which changed from 536 dyads to 326 patients. Target accrual completion in the restructure was moved from July 31, 2023 to March 31, 2025.
Because of the randomized study design, changes to the eligibility criteria were not felt to contribute to imbalance in patient characteristics between study arms. However, given the possibility that eliminating the requirement for a spouse caregiver (and caregiver participation) may result in a study population with less family support and potentially lower adherence to the study intervention and follow-up assessments, the study team plans to evaluate adherence to and effect of the intervention in patients with vs without a caregiver.
Caregiver analyses were moved to an exploratory analysis. At the end of the study period, correlative analyses will be conducted to examine the extent to which the patient credit report is sufficient to represent financial status and hardship at the household level.
Impact on Enrollment
In February of 2023, prior to the study restructure, the study had only enrolled 62 patient-spouse/partner dyads (11% of the target accrual, approximately 75% behind the target accrual set initially in the grant). The study restructure was implemented among accruing sites in July 2023, and enrollment to the study increased from an average of 4.1 patients per month to 13.6 patients per month (Figure 1). The study closed to accrual on December 15, 2024, 3.5 months ahead of the restructure timeline, with 331 patients and 139 spouse or partner caregivers. The study has diverse representation with 13% of patients identifying as Black or African American and 9% of patients identifying as Hispanic/Latino. Patient Registration by 3-Month Intervals. *Reflects Enrollment From October 1, 2024-December 15, 2024.
Changes to the study protocol through the NCI restructure were particularly impactful for M/U NCORP sites, who reported challenges in enrollment particularly due to dyadic enrollment requirements. For example, one specific M/U NCORP site, UNM, noted that prior to the restructure 59.1% of its trial screen failures were attributed to either the patient not having a partner or the patient’s partner not being interested in participating. Despite great efforts to enroll participants, between July 2022 (when the study opened at UNM) and July 2023 (when the restructure amendment went into effect), UNM was only able to accrue two patient/caregiver dyads to the study, an average monthly accrual rate of 0.15. Between August 2023-December 2024 (study closure), UNM was able to accrue 28 participants to the study, an average monthly accrual rate of 1.5. Importantly, this site has been able to accrue a diverse population, with 46% of their study enrollees identifying as Hispanic, 7.7% as Black or African American and 3.8% as American Indian or Alaska Native.
Discussion
We activated a first of its kind randomized controlled trial of financial navigation to address financial hardship among cancer patients and their spouse-caregivers. Due to the novelty and complexity of the study in addressing financial hardship, the study faced several barriers to recruitment in the initial study design. Through solicitation of feedback, the study team was able to restructure the project in a way that facilitated successful accrual while maintaining scientific integrity. To be able to successfully evaluate financial interventions in cancer populations, study teams should be pragmatic in their approach and allow venues for accrual sites to vocalize barriers and solutions early and often, to ensure study success. This openness to feedback will also likely be relevant to other treatment and non-treatment trials.
While recognizing the importance of studying the financial burden of a cancer diagnosis on both patients and their caregivers, and the merits of dyadic research, we learned that study designs requiring dyadic participation are not always feasible. In this study, requirement of a spouse or partner caregiver was a particular challenge as sites did not have a systematic way to screen for this and felt it was an uncomfortable conversation to have with patients. Additionally, many patients did not have a spouse/partner caregiver leaving them unable to benefit from this important intervention. Ultimately, requiring dyadic enrollment proved to be too big of a barrier to recruitment, and the study was forced to make a pragmatic decision by adjusting to make caregiver enrollment optional. While we acknowledge the challenge of requiring dyadic enrollment, the experience of the patient/caregiver dyad remains important to explore and may be necessary in specific study designs. For example, an underexplored area in dyadic financial toxicity research is cultural differences in financial management for couples. Future studies may wish to explore how cultural differences in dyads impact financial navigation interventions. In our study, allowing sites to continue to optionally accrue caregivers will provide preliminary data on important caregiver outcomes such as caregiver quality of life and care burden. Caregiver enrollment will also allow us to conduct preliminary correlative analyses to explore the extent to which the patient credit report is sufficient to represent financial status and hardship at the household level. For example, if caregivers are consistently bearing more of the financial burden and credit strain on behalf of patients, then the primary outcome (patient financial hardship based on credit reports) may underestimate the true financial impact of cancer. Alternatively, if the patient credit report alone is a reasonable surrogate, this could have implications for future trial designs in this research setting.
Additionally, understanding how an intervention to mitigate financial hardship is received by participants is critical to understand in order to develop programs that are sustainable and accessible to cancer patients and their caregivers. Understanding when to approach cancer patients, particularly those with a later stage diagnosis, in their treatment trajectory with financial navigation is crucial to ensure patients can obtain the most benefit. The study team was able to react to feedback that a 120 day from diagnosis window was too early for this intervention and adjust that window to 180 days, with feedback that patients were much more receptive to financial conversations when they were further out from their initial diagnosis. After learning that interaction with multiple financial navigation partners and requirements that dyads be present together on financial navigation calls was infeasible for this patient population, we adjusted our intervention to only include one financial navigation partner and to loosen requirements for dyadic participation in calls. This allowed for a more streamlined intervention, taking up less of the participant’s time and minimizing confusion about which organization could provide what service. Particularly for later-stage cancer patients, who are juggling many priorities and have limited time, streamlining services to one point of contact provides a much more sustainable approach to navigation.
These findings have several implications for future research in this area. Having a pragmatic approach to research to mitigate financial hardship allows for interventions that can successfully be completed, analyzed, and translated into sustainable programs in real world settings. When considering involvement of caregivers in financial hardship research, designing studies that allow for caregiver involvement to be optional rather than a hard eligibility requirement may provide a better avenue to completing recruitment while still enabling exploratory analysis of caregiver/dyad outcomes. Thinking through and being nimble in changing how financial hardship interventions are delivered (e.g., who delivers, at what time points and how long the intervention takes) is key in ensuring participants can receive the intervention.
There has been a call to combine financial navigation studies with implementation frameworks in order to better move from research to standard practice. 19 This study can serve as a model for broader implementation science (IS) considerations when considering how to deal with practical changes in real-time in order to successfully enroll participants and complete large-scale studies. While this study does not use an IS theory or method, future studies could evaluate their modifications using IS methods such as Framework for Reporting Adaptations and Modifications to Evidence-based Implementation Strategies (FRAME-IS) 20 to help support the reasoning behind and assess the impact of their modifications.
Finally, when designing and managing financial navigation or financial hardship studies, it is critically important to give accruing sites a venue for feedback. Study teams should provide an “open door” policy via multiple avenues (emails, calls, group meetings, etc.,) to allow for sites to vocalize barriers to recruitment as well as provide opportunities for sites to learn best practices in recruitment from each other as well as patient partners. While it is not always possible to react and change study designs in response to site feedback, some changes can provide major impacts on the ability to complete a study successfully.
Supplemental Material
Supplemental Material - Addressing Challenges in Research Aimed at Reducing Financial Toxicity Among Cancer Patients and Caregivers: An Example From the CREDIT Study (SWOG S1912CD)
Supplemental Material for Addressing Challenges in Research Aimed at Reducing Financial Toxicity Among Cancer Patients and Caregivers: An Example From the CREDIT Study (SWOG S1912CD) by Ari Bell-Brown, Bernard Tawfik, Babara Segarra-Vazquez, Talor Hopkins, Kate Watabayashi, Patricia O’Kane, Ruth C. Carlos, Shelby L. Langer, Joseph M. Unger, Amy K. Darke, Dawn L. Hershman, Scott D. Ramsey, and Veena Shankaran in Cancer Control
Footnotes
Acknowledgements
We would like to acknowledge all of the enrolling sites who provided feedback on the protocol.
Ethical Statement
Author Contributions
ABB: Writing- Original Draft, Project administration, Resources; BT: Investigation; Writing- Review & Editing; BSV: Resources, Writing- Review & Editing; TH: Project administration, Writing- Review & Editing; KW: Project administration, Writing- Review & Editing; POK: Project administration, Writing- Review & Editing; RCC: Investigation, Writing – Review & Editing; SLL: Investigation, Writing – Review & Editing; JMU: Investigation, Writing- Review & Editing; AKD: Investigation, Writing- Review & Editing; DLH: Investigation, Writing- Review & Editing; SDR: Investigation, Writing- Review & Editing; VS: Investigation, Writing- Review & Editing, Supervision, Methodology, Conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers R01CA248656, UG1CA189974, and UG1CA189856.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.