
Abstract
Introduction
While race/ethnicity are established factors of risk and outcomes for multiple cancers in women, nativity may more precisely estimate cancer risk and survival. The role of nativity in choriocarcinoma, a form of gestational trophoblastic neoplasia arising from the placenta, is unexplored. Our objective was to examine how race, ethnicity, and nativity influence disease presentation and survival in women with choriocarcinoma in Florida.
Methods
Using the Florida Cancer Data System (FCDS), we identified women diagnosed with choriocarcinoma from 1981-2020. Clinicodemographic data were extracted, including nativity (US-born/Non-US-born). Statistical analyses included chi-square, Cox proportional hazards models, and Kaplan-Meier method, with significance set at P < 0.05.
Results
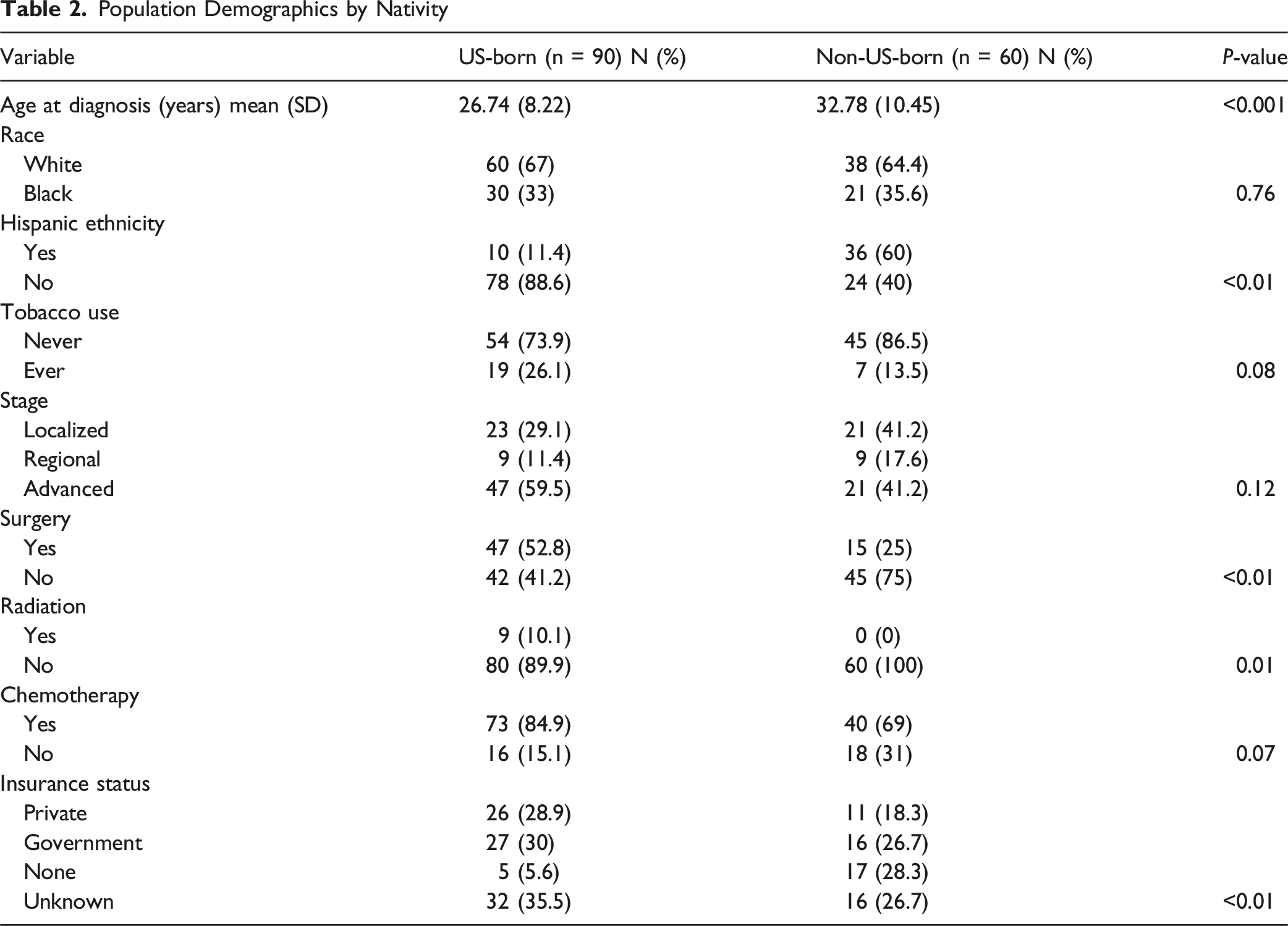
262 eligible patients were included. Black women more frequently presented with distant disease vs White women (63.8% vs 46.2%, P = 0.05). Non-US-Born women were older at diagnosis than US-born (32.8 vs 26.7 years, P < 0.01) and received fewer surgical and radiation treatments (P < 0.05). Nativity, ethnicity, and race were not associated with overall survival (OS) (all P > 0.05). Multivariable analyses adjusted for race and birthplace showed increasing age (HR 1.05 [1.02-1.09], P = 0.023) and surgical treatment (HR 0.28 [0.09-0.79], P = 0.016) were associated with OS. Despite favorable OS, survival curves diverged after initial treatment, favoring White over Black patients, and Hispanic over Non-Hispanic patients, though neither were statistically significant (P > 0.05).
Conclusion
Race and nativity are associated with variations in choriocarcinoma presentation and treatment course but do not affect survival. Race and ethnicity may predict post-treatment, long-term survival, though whether this reflects choriocarcinoma biology or broader disparities remain unclear.
Introduction
Choriocarcinoma is the most common histologic type of gestational trophoblastic neoplasia (GTN), a rare malignancy originating from the placenta, with an incidence of 3/100,000 deliveries in the US and Europe annually. 1 It represents only 1% of gynecologic cancers, and with a greater cure rate in metastatic disease compared to other gynecologic malignancies.1,2 Given the rarity of this tumor type, however, the influence of sociodemographic factors on outcome measures has been difficult to study.
The current population in the Western Hemisphere, inclusive of Central and South America and the Caribbean, represents centuries of admixture of Native Americans, Europeans, and Africans. The unique geography of the region and patterns of migration, creating pockets of isolation and genetic drift, have resulted in populations with unique genetic compositions and cultural practices. These unique subpopulations have variable risks for hereditary cancers, demonstrate differences in cancer presentation and distribution, and experience unique cancer survival outcomes. For example, in a large population of Caribbean women with breast and ovarian cancer, George et al 3 reported on substantial variation in the proportion of patients with mutations in BRCA genes by nativity. Variation in risk has also been demonstrated in Caribbean, South/Central American, and US-born women with endometrial cancer4,5 and ovarian cancers, 6 while overall survival is associated with both country and region of birth for women with breast 7 and endometrial cancers. 8 These studies demonstrate that thorough cancer epidemiologic evaluations require a consideration of nativity in addition to standard demographic assessments like race and ethnicity, which aggregate dissimilar populations and thus may not reflect true estimates of cancer risk and outcomes.
Because choriocarcinoma is a rare tumor, few studies have evaluated the role of race in patients with this disease, and there are no data on nativity. Of the few in which the influence of race was explored, non-Hispanic Black (NHB) women were the only group to have a higher risk of death compared to non-Hispanic Whites (NHW), and were diagnosed at the youngest ages. 2 Subsequent investigators have reported that Black women with low-risk GTN have similar rates of chemosensitive disease compared to NHW women, suggesting that factors beyond treatment approaches influence outcomes. 9 Given the emerging findings on the importance of nativity as a mitigating factor in generating risk estimates, identifying variations in disease presentation, and characterizing disparities in outcome, and the lack of such data in patients with GTN, our objective was to investigate the implications that race (group sharing based on physical characteristics such as skin color), ethnicity (cultural identity), and nativity (country or region of birth) have on distribution of disease and survival outcomes specifically in patients with choriocarcinoma. Given the substantial contribution of immigrants from the Caribbean and Central/South America in Florida, evaluating this population may provide insight on the role of nativity in this disease.
Materials and Methods
Data Sources
Data were abstracted from the Florida Cancer Data System (FCDS) to perform the analyses. The FCDS is an obligatory, population-based registry which has collected statewide cancer data on all reportable cases since its inception in 1981. As part of the Centers for Disease Control’s National Program of Cancer Registries (NAACR), the FCDS meets national standards for data quality. At the time of analysis v.25 of the NAACR data dictionary was used.
Ethics Approval
Review and analysis of the FCDS was approved by the State of Florida Department of Health Institutional Review Board. Informed consent was waved by the Florida Department of Health as all patient information is de-identified and non-discoverable.
Study Design
This study utilizes a retrospective cohort design.
Study Cohort
Cases were selected utilizing the International Classification of Diseases for Oncology, 3rd edition, ICD-O-3 codes C589 (primary site: placenta) and 9100/3 (histologic subtype: choriocarcinoma). A date range of January 1st, 1981, through December 31st, 2020, was used to capture the latest available data. Women were included who self-identified as either White or Black. All other races were excluded due to insufficient sample sizes.
Data Collection
Abstracted variables included: age at diagnosis (in years), country of birth (US-born vs Non-US-Born), self-identified race (White, Black), ethnicity (Hispanic, non-Hispanic), stage of disease (local, regional, advanced), type of insurance (private, government, other, unknown), tobacco use (never vs ever), surgery (yes/no), radiation (yes/no), and chemotherapy (yes/no). Overall survival was defined as time from diagnosis to date of death (all-cause). Country of birth was classified as either US-born or Non-US-Born. Women born outside of the US were from the Caribbean, South America, or Central America, and were analyzed collectively as a single group.
Statistical Analysis
Statistical analyses were performed using STATA/BE 18.5 (StataCorp, College Station, TX). All patients were included in the analyses, even when missing specific data points. Summary statistics were used to describe the cohort. The Student t-test and Wilcoxon Rank Sum test were used to analyze continuous variables. Chi-square (or Fisher exact, if appropriate) was used to determine associations between categorical variables. Univariable and multivariable Cox proportional hazards models were conducted to assess factors associated with overall survival (OS). Multivariable models were generated including covariates with P-values ≤ 0.05 from the univariate analyses. Because race and nativity were specific outcomes of interest, multivariable models were adjusted for both. Survival curves were generated and analyzed using the Kaplan-Meier method and log-rank test, respectively. All tests were two-sided with significance set at P < 0.05.
Results
Of the 317 patients identified with cancers originating from the placenta during the interval of interest, 262 were eligible for inclusion (Figure 1). A comparison of demographic characteristics between Black and White patients is shown in Table 1. There was no significant difference in mean age at diagnosis by race (P = 0.69). A significantly higher percentage of self-identified White women were Hispanic compared to those who self-identified as Black (37.5% vs 1.2%, P < 0.01), consistent with the demographics of Florida. Black women were more likely to have advanced stage or distant disease at the time of diagnosis compared to White women (63.8% vs 46.2%, P = 0.05). There was no significant difference in the prevalence of smokers between Black and White women (P = 0.28). There were no statistical differences between races for those who received chemotherapy, surgery or radiation. Though not statistically significant, a higher proportion of White women (26.8%) had private insurance compared to Black women (14.5%, P = 0.06). CONSORT diagram for population Population Demographics by Race

Population Demographics by Nativity
Cox Proportional Hazards Models for Overall Survival

*HR (hazard ratio), CI (confidence interval).
There was no difference in the Kaplan-Meier curves for OS by race (P = 0.15) or ethnicity (P = 0.39) (Figure 2). However, while the overall survival for the entire population was favorable, once outside of the initial diagnostic/treatment window, there was a divergence of the survival curves favoring White (vs Black) patients (25th percentile for OS White 243.6 months [95% CI 95.8-376.9] vs Black 55.3 months [95% CI 11.4-353.3]), though not statistically significant. Among Hispanic patients, there was also a divergence in the curves early on, favoring Hispanic patients, though this did not translate into a statistically significant OS improvement. Evaluation of nativity among White, Black, and Hispanic patients revealed no impacts on OS (Figure 3). Overall survival assessments Overall survival relative to nativity. Nativity is not associated with overall survival when race (3A-Black, log-rank P = 0.63; 3B-white, log-rank, P = 0.67) or ethnicity (3C-Hispanic, log-rank P = 0.74) are considered

Discussion
In this population of patients with choriocarcinoma in Florida, while Non-US-Born nativity was associated with an older age at diagnosis and less utilization of care, it did not impact overall survival. Black patients presented with more advanced stage disease. While survival immediately post-diagnosis was similar across race and ethnicity, variable, though nonsignificant, long-term survival differed by demographics.
Choriocarcinoma as a disease varies in several ways from other gynecologic cancers. First, most common gynecologic cancers (ovarian, endometrial) arise as women age, which allows for the accumulation of exposures, epigenetic changes, and somatic mutations in tissues. 10 Conversely, choriocarcinoma is driven by aberrant chromosomes in the placenta, which occur spontaneously when sperm and ovum interact, so the pathway by which malignancy arises differs. 11 Because this happens immediately upon conception, the chronicity of exposure associated with other cancers of adulthood, and specifically the social/biologic stressors associated with race or immigrant status, does not occur. Furthermore, because choriocarcinoma follows an antecedent pregnancy and pregnancy-related care in Florida is covered through both state and federal health insurance plans, 12 women are more likely to have already engaged in health care seeking recently related to their pregnancies and thus have an established provider. 1
Race and ethnicity are established prognostic factors for many gynecologic cancers. Beyond these social constructs, however, specific country of birth and nativity have been shown to more precisely estimate both cancer risk and survival. Jeudin et al. 13 reported that cervical cancer survival outcomes differ between Black and White women based on Caribbean nativity, with worse survival outcomes in US-born Black women. Schlumbrecht et al. reported that there was significant variation in endometrial cancer risk among subpopulations of Hispanic women with type II endometrial cancer when evaluated by region of birth, and that Hispanic ethnicity among Caribbean women was significantly associated with improved ovarian cancer survival relative to their US-born counterparts.5,6 Further disaggregation within the Caribbean region demonstrated that specific country of birth was also associated with survival in endometrial cancer. Mercadel et al 8 showed that among women with high-grade histologies, those from Haiti had a shorter overall survival than those born in Jamaica.
Our analysis found that Black women had a higher disease stage at the time of diagnosis compared to their White counterparts. This trend is well described in the literature and holds true for gynecologic 14 and breast cancers. 15 Numerous factors have been implicated in this phenomenon including lower socio-economic status, delayed health care access, perceived discrimination/medical mistrust, and prolonged symptom duration prior to diagnosis.16-18 Additionally, misconceptions around abnormal vaginal bleeding, often the harbinger of most uterine cancers, have been implicated in a delay in health care seeking among Black women with endometrial cancer. 19 Though abnormal vaginal bleeding can be a presenting sign of choriocarcinoma, it remains unclear if similar misconceptions apply to Black women with choriocarcinoma leading to delays in health care seeking. Given that choriocarcinoma follows an antecedent gestation, it is significant to note that substantial racial and ethnic disparities exist in the post-partum period with respect to losing insurance (Medicaid specifically) or being uninsured. The loss of insurance in this population may lead to delays in care seeking for racial and ethnic minority women after pregnancy.20-22
Our analysis revealed poorer overall survival for Black women beyond the initial treatment. Similar trends exist in other cancer types with high cure rates. For example, long term breast cancer survivorship is poorer for Black women with early stage disease.23,24 Other research has reported that NHB women have significantly shorter survival than NHW women with endometrial cancer with low risk features (stage I/II disease or low-grade).25,26 Similarly, though 5 years overall survival from thyroid cancer remains high, Black patients have lower survival than their White counterparts.27,28 Interestingly, our survival data are similar to those reported by Tarney et al, 2 who published the largest series on choriocarcinoma to date (n = 947) utilizing SEER. While the population demographics included in our investigation differed from that study, with a higher proportion of Black patients (31.7% vs 18.8%), the survival curves were similar. Specifically, the immediate post-diagnosis survival was similar to other races, but there was also a prolonged trend towards worse survival many years after diagnosis that was not reflected in other races or ethnicities. In the context of choriocarcinoma, this trend likely suggests a more systemic problem about chronic retention in the healthcare system with ongoing access but underscores the need to both explore biologic drivers of survival while developing a robust survivorship pathway for women with choriocarcinoma at long-term risk for adverse outcomes.
Women with choriocarcinoma born outside of the US had differences in disease presentation, being diagnosed at an older age. This pattern has been previously reported. Among cervical cancer patients similar patterns were appreciated, with both Black and White Caribbean-born women receiving cancer diagnoses older than women born in the US. 13 Caribbean-born ovarian cancer patients are also diagnosed at an older age than their US-born counterparts. 6 These findings, however, are not universal. Barreto-Coelho, et al 29 noted that among women with breast cancer, Black Caribbean-born immigrants were diagnosed two years earlier than those born in the US. Age of diagnosis is likely influenced by multiple factors, including genetic, environmental, and epigenetic changes, and the etiology of the older age at diagnosis in our Non-US-Born cohort is unclear. However, understanding that reproductive factors are very influential in this tumor, age of diagnosis may be reflective of personal obstetric history.
Utilization of healthcare services also varied by nativity in this cohort, with Non-US-Born women undergoing less radiation and surgery. Access to cancer care among immigrant populations in Florida is variable. Jacobs et al 30 noted that among patients with early lung cancer, while NHW patients had higher rates of curative intent surgery than Black patients, immigrants from the Caribbean more often had surgery than US-born Blacks. In fact, US-born Blacks had the lowest rate of broader curative-intent treatment. In another study of ovarian cancer patients, chemotherapy and surgery delivery did not differ by nativity, but maximal surgical effort favored women born in the US. 6 For patients with endometrial cancer, no variations in cancer treatment modality use by nativity have been reported. 31 Access to cancer services is complicated and more likely due to social and economic factors than biological ones. A recent policy report cites undocumented status, Medicaid expansion variability, and access to emergency services as barriers to sufficient cancer care coverage, 32 but reliance on traditional medicine 33 and hesitancy to engage the healthcare system 34 also likely contribute to these findings.
Strengths and Limitations
Our study has several limitations. The FCDS is uniquely positioned to capture differences in nativity based on Florida’s diverse patient population due to immigration patterns from the nearby Caribbean and Central/South American regions. The uniqueness of this database may limit the generalizability of these data for the remainder of the country. However, given current trends in the racial and ethnic evolution of the United States, 35 these data find relevance. Given the limited sample size, we did not evaluate patients by specific country of birth or region, which would be of value since specific geographic locations have been associated with variable risks and outcomes in other disease sites. Our analyses also excluded women of Asian race due to low numbers, which is reflective of the small Asian population in Florida (6%). 36 Choriocarcinoma and GTN have been shown to have a higher incidence in Asian women, 37 so further studies evaluating nativity should focus on populations with higher Asian representation. Additionally, the FCDS is limited as individual-level data points, including medical comorbidities, treatment plans, treatment complications, time in the United States (as a measure of acculturation), and disease-specific survival, are not included. Choriocarcinoma is a rare tumor, so the sample size is admittedly small, and thus we are likely underpowered to detect subtle differences between groups. Larger datasets, or combinations of datasets for this rare tumor, would be better able to validate our findings. Despite the long interval of study, we have little concern about the role of temporal bias as treatment algorithms for choriocarcinoma have not substantially changed in decades. Further, statistically significant associations between overall survival and both increasing age and receipt of surgery were noted in this cohort. These are known mediators of outcome, and consistent with prior literature, 2 and argue for the validity of this dataset. Despite the study’s limitations, because nativity data is captured in Florida, and not in other large national databases such as SEER, our analysis - as the first to explore nativity for this disease - provides at least some preliminary context to the role nativity plays in choriocarcinoma presentation and survival.
Conclusion
There are variations in choriocarcinoma presentation and care access by race and nativity in this population. Nativity failed to demonstrate significant influence on overall survival. Though not statistically significant in this study, our data suggest that Black race and Hispanic ethnicity may be predictive factors in long-term overall survival among women with this disease. Whether this is mediated by the biology of choriocarcinoma itself or reflective of disparities in other domains of influence is unclear. Future research with larger cohorts, likely requiring combined datasets, is needed to further investigate how race, ethnicity, and nativity influence cancer risk and development, and mediate outcomes long into the survivorship period. However, awareness of the differences in long-term overall survival suggests potential opportunities for intervention, including more intensive efforts to ensure women with this disease and at risk for disparate outcomes are retained in the healthcare system following choriocarcinoma treatment and throughout the survivorship continuum.
Footnotes
Acknowledgements
The Florida cancer incidence data used in this report were collected by the Florida Cancer Data System under contract with the Florida Department of Health (DOH). The views expressed herein are those of the authors, and do not necessarily reflect those of the contractor or DOH.
Ethical Considerations
Review and analysis of the FCDS was approved by the State of Florida Department of Health Institutional Review Board. Informed consent was waved by the Florida Department of Health as all patient information is de-identified and non-discoverable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Sylvester Comprehensive Cancer Center and the National Cancer Institute of the NIH under award number P30CA240139.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.