
Abstract
Background
Pancreatic cancer (PC) is one of the most lethal cancers around the world. A high body mass index (BMI) is recognized as a significant and modifiable risk factor for this disease.
Methods
Data were obtained from the Global Burden of Disease (GBD) 2021 study. We used joinpoint regression and age-period-cohort (APC) models for trend analysis, and the Autoregressive Integrated Moving Average (ARIMA) model to forecast the burden of high BMI-related PC in 2022-2041. In addition, we used decomposition and health inequality analyses to examine causes and regional inequalities in the burden of high BMI-related PC.
Results
From 1990 to 2021, the total number of deaths from high BMI-related PC increased nearly tenfold. In the last 30 years, females consistently bore a greater burden of BMI-related PC, whereas the increase among males was more substantial. Deaths from high BMI-related PC escalated by 7 to 12 times in the 20-49 age group and by over sevenfold in low social development index (SDI) regions, reflecting increasing risk in younger populations and worsening global health inequalities. Furthermore, we predict that the global age-standardized mortality rate (ASMR) will continue to increase over the next 20 years.
Conclusion
Our findings generally revealed a sharply increased trend for the global burden of PC associated with high BMI during the past 30 years, as well as pronounced disparities by sex, age, and region. Hence, countries and nations should urgently advocate targeted public health initiatives in the future, especially in high-burden regions and populations.
Plain Language Summary
Background: Pancreatic cancer (PC) is one of the most lethal cancers around the world. A high body mass index (BMI) is recognized as a significant and modifiable risk factor for this disease. Methods: Data were obtained from the Global Burden of Disease (GBD) 2021 study. We used joinpoint regression and age-period-cohort (APC) models for trend analysis, and the Autoregressive Integrated Moving Average (ARIMA) model to forecast the burden of high BMI-related PC in 2022–2041. In addition, we used decomposition and health inequality analyses to examine causes and regional inequalities in the burden of high BMI-related PC. Results: From 1990 to 2021, the total number of deaths from high BMI-related PC increased nearly tenfold. In the last 30 years, females consistently bore a greater burden of BMI-related PC, whereas the increase among males was more substantial. Deaths from high BMI-related PC escalated by 7 to 12 times in the 20–49 age group and by over sevenfold in low social development index (SDI) regions, reflecting increasing risk in younger populations and worsening global health inequalities. Furthermore, we predict that the global age-standardized mortality rate (ASMR) will continue to increase over the next 20 years. Conclusion: Our findings generally revealed a sharply increased trend for the global burden of PC associated with high BMI during the past 30 years, as well as pronounced disparities by sex, age, and region. Hence, countries and nations should urgently advocate targeted public health initiatives in the future, especially in high-burden regions and populations.
Introduction
Pancreatic cancer (PC) is one of the deadliest malignant tumors in the world and is the seventh most common cancer-related cause of death.1-3 It is mainly categorized into two types: pancreatic adenocarcinoma and pancreatic neuroendocrine tumors, of which the former accounts for about 85% of all cases.4,5 In clinical practice, PC is typically staged from I to IV: stage I (resectable, no metastasis), stage II (local or borderline resectable), stage III (locally advanced or unresectable), and stage IV (metastatic). Because early symptoms are vague and diagnosis is challenging, most of the patients are diagnosed at stage III or IV, which has a poor prognosis. 2 As an important physiological endocrine and digestive organ, the pancreas plays a vital role in human health. PC is extremely aggressive and is one of the leading causes of cancer fatalities and the increased global disease burden.6-8 Incidence and mortality of PC have seen a steady rise over the last decade, and in the year 2017, it resulted in more than 9.1 million disability-adjusted life years (DALYs) worldwide. The related deaths from PC grew by 332,949 cases between 1990 and 2019.1,9,10 Several studies have determined some risk factors for PC, of which high body mass index (BMI) is a prominent contributor.11-13 For individuals aged 20 or above, a high BMI is a BMI of ≥25 kg/m2, and an optimal range (lowest risk) is considered a BMI between 20-25 kg/m2. 14 A high BMI represents a risk factor for various types of cancer, with around 13% of global cancer cases associated with high BMI. In recent years, the global average BMI has risen by almost half a unit per decade, leading to over 600 million adults worldwide with a BMI of ≥30 kg/m2, most prevalent in the US. 11 Studies suggest that mice fed high-fat, high-caloric diets develop obesity and chronic inflammation due to elevated blood lipids and visceral fatty tissue accumulation that promotes pancreatic tumor advancement.15-17 Weight management through exercise can reduce the risk of PC. 18 In addition, KRAS oncogene mutations are closely linked to pancreatic ductal adenocarcinoma (PDAC). Experimental studies have uncovered that obesity-induced activation of KRAS downstream signaling pathways can accelerate the progression of PDAC.15,19-21
Several pieces of evidence have signified higher BMI with the development and progression of PC. As a modifiable risk factor, obesity should deserve greater public health focus. Despite growing evidence linking high BMI to pancreatic cancer, few studies have systematically quantified its global burden, particularly in relation to sex, age, and socioeconomic development levels. Moreover, the degree to which health inequalities shape this burden across regions remains underexplored. Therefore, we conducted a study to shed light on the impact of the PC attribute on high BMI and to characterize its distribution according to SDI regions, sex, age, and 204 countries, to inform policies oriented towards prevention, diagnosis, and treatment at a global level.
Methods
Data Sources
We obtained data from the Global Burden of Disease (GBD) 2021 database, developed by the Institute for Health Metrics and Evaluation (IHME), the preeminent platform for epidemiology research globally. Our analysis focused on pancreatic cancer (PC) attributable to high body mass index (BMI), using the GBD comparative risk assessment framework. The specific methods are as follows: GBD Estimates were categorized under “Risk factor,” “Measure”denoting “Deaths” and “DALYs (Disability-Adjusted Life Years),” “Metric” representing “Number” and “Rate,” “Risk” defined as “High body mass index (BMI),” “Cause” as “Pancreatic cancer,” “Location” encompassing “all countries and territories,” “High SDI(Socio-demographic Index),” “High-middle SDI,” “Middle SDI,” “Low-middle SDI,” “Low SDI,” and “global,” “Sex” as “Male,” “Female,” and “Both,” “Age” including “All ages,” “Age-standardized,” and “0-100 years,” and “Year” covering the full range from 1990 to 2021. All data are publicly available at https://vizhub.healthdata.org/gbd-results/.
Socio-demographic Index (SDI)
The Socio-demographic Index (SDI) is an aggregated index applied to measure the level of socioeconomic progress of a country. It is generated from country-level per capita income, average educational attainment, and total fertility rate (TFR). Higher scores mean more socioeconomic development. Countries were divided into five quintiles for the GBD Study of 2021, including high SDI (>0.81), high-middle SDI (0.70-0.81), middle (0.61-0.69), low-middle SDI (0.46-0.60), and low SDI (<0.46).
Statistical Analysis
To assess the temporal trends in age-standardized mortality rates (ASMR) and age-standardized disability-adjusted life years (ASDR) of PC attributable to high BMI from 1990 to 2021, we employed two approaches to calculate the estimated annual percentage change (EAPC). Initially, we conducted a primary estimation using a log-linear regression model, formulated as follows:
To predict future trends about the ASMR in PC related to high BMI from 2022 to 2041, we utilized an autoregressive integrated moving average (ARIMA). The model parameters (p, d, q) were optimized automatically using the auto. arima() function, and goodness of fit was assessed via AIC, BIC, and residual autocorrelation. We used varied relevant tests to evaluate model accuracy. Residual analysis revealed no significant autocorrelation, hence affirming the model’s resilience. Full estimation results and diagnostic graphs are presented in the Appendix. All statistical analyses and visualizations were conducted using R software (version 4.5.0).
Ethical Statement
This study complies with the GATHER guidelines. 22 The data employed in this study are aggregated, ensuring that no information of individual patients or public personnel is directly implicated.
Results
Global Burden and Trends of PC Attributable to High BMI
Figure 1 illustrates a worrying global trend in the ASMR and ASDR of PC attributed to high BMI-related PC from 1990 to 2021. This trend is similar in the increasing number of deaths and DALYs (Fgure.2). As shown in Table 1, the number of deaths attributable to high BMI-related PC increased from 954.64 (95% UI: −2011.36 to 5926.31) in 1990 to 9215.35 (95% UI: −23,773.4 to 26,607.43) in 2021. DALYs also rose substantially, from 21,952.36 (95% UI: −49,858.62 to 141,074.63) to 223,367.68 (95% UI: −47,781.52 to 626,549.71), both representing an approximate ten-fold increase. These findings indicate a continuously rising burden of high BMI-related PC at the global level. Global Trends in Age-Standardized Mortality Rates(ASMR) and Age-Standardized DALY Rates (ASDR) Related to Pancreatic Cancer Attributable to High BMI, 1990-2021. The Blue and Red Lines Respectively Represent the Trend in ASMR and ASDR, While the Dots Indicate the Corresponding Values for Each Year. Both ASDR and ASMR Exhibited an Upward Trend Change in Mortality and DALYs for Pancreatic Cancer Attributable to High BMI Around the World, 1990-2021 Age-standardized rate(ASR): Age-standardized rates per 100,000; ASMR: Age-standardized mortality rate; ASDR: Age-standardized disability-adjusted life years rate; DALYs: disability-adjusted life years; EAPC: Estimated annual percentage change; TPC: Total percentage change.

Table 1 and Figure 2 present an interesting phenomenon in 5SDI regions: in 1990, the number of deaths and DALYs attributable to high BMI-related PC was greatest in high SDI regions, followed by high-middle SDI regions. In contrast, the Middle SDI, Low-middle SDI, and Low SDI regions exhibited negative values for both deaths and DALYs, indicating the lack of a attributable burden of high BMI on PC in these regions. By 2021, however, this pattern had changed. In the Middle SDI and Low-middle SDI regions, the number of deaths attributable to high BMI-related PC reached 1147.38 (95% UI: −677.54 to 4003.97) and 449.24 (95% UI: −132.64 to 1369.32) (Table 1), respectively, suggesting that high BMI-related PC poses a growing public health burden in these regions. Although low SDI regions lack statistically significant burden estimates, their upward trajectory in DALYs suggests a transition toward measurable disease burden. Trends in Deaths, ASMR, DALYs, and ASDR Related to Pancreatic Cancer Associated With High BMI Around the World From 1990 to 2021, Differentiated by SDI. (A) Deaths and ASMR; (B) DALYs and ASDR. Bars Represent the Absolute Number of Deaths or DALYs; lines Indicate Age-Standardized Rates; Black Vertical Bars Indicate 95% Confidence Intervals (CI) for Numbers, and Shaded Bands Represent 95% CI for Rates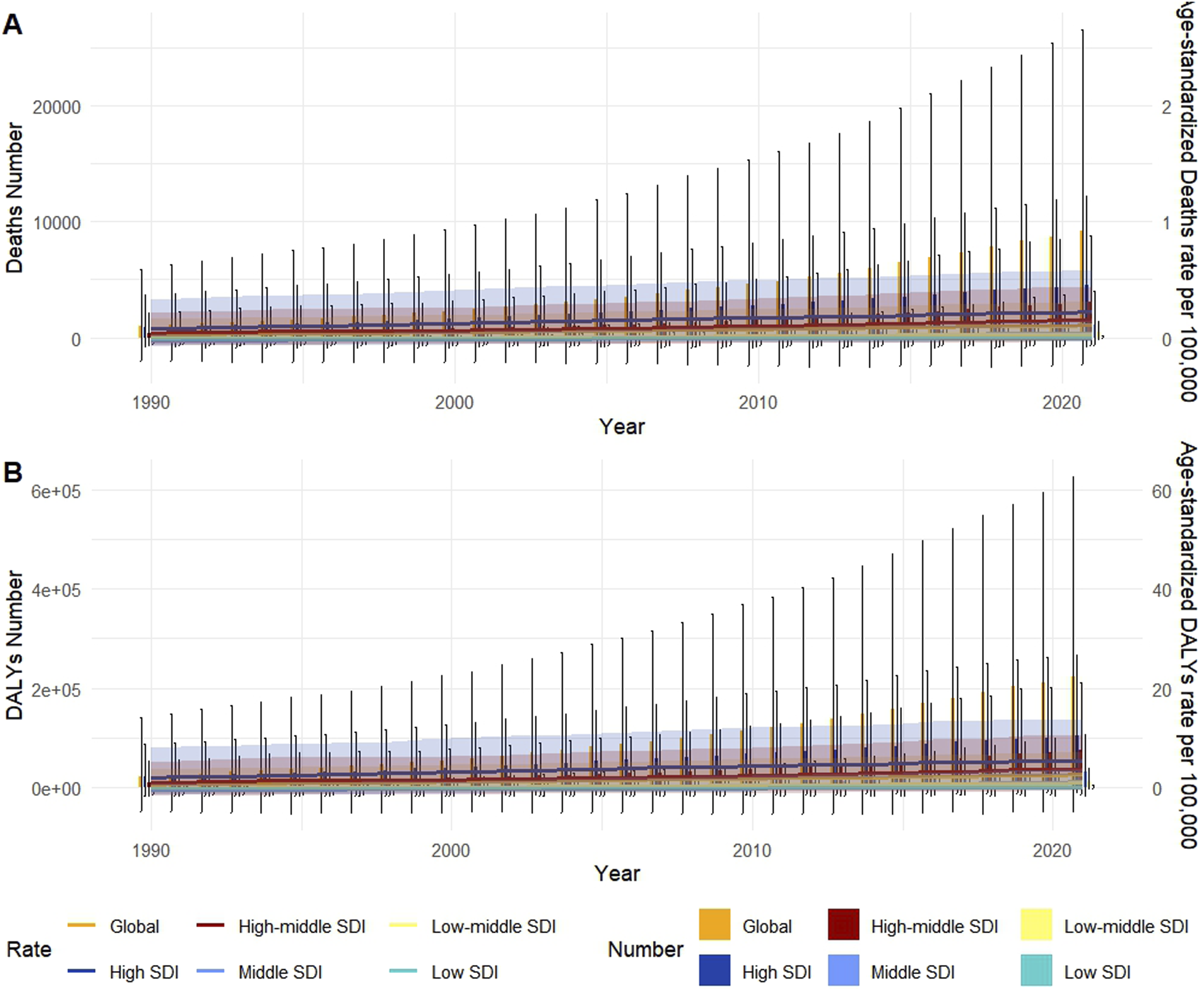
An analysis of data from 204 countries showed that, compared with 1990, the ASMR for PC attributable to high BMI demonstrated a global upward trend in 2021 (Figure 3). In 1990, regions where ASMR was relatively high were North America, Europe, Oceania, and Northern Asia (Figure 3A). At this time, the five countries where the highest numbers of deaths attributed to high BMI-related PC were the United States (616.89; 95% UI: −135.71 to 1843.56), the Russian Federation (260.85; 95% UI: −75.85 to 757.98), Germany (179.67; 95% UI: −78.01 to 598.07), the United Kingdom (120.06; 95% UI: −60.26 to 422.70), and Ukraine (82.77; 95% UI: −11.67 to 223.74). By 2021, the ASMR for PC attributable to high BMI rose dramatically in Oceania and Northern Asia (Figure 3B). Among all countries, Brazil (EAPC: 6.08%; 95% CI: 5.57 to 6.58) experienced a sharp rise in the deaths from high BMI-related PC and occupied the fourth position in the world, following the USA (2666.00; 95% UI: −2.55 to 5994.49), the Russian Federation (863.74; 95% UI: −19.36 to 2105.64), and Germany (500.43; 95% UI: −85.31 to 1422.66). It is worth mentioning, however, that in calculating the EAPC of ASMR and ASDR across the five SDI regions and 204 countries, the existence of zeroes or negative values in some regions (eg, in Algeria or the Low SDI region) from 1990 to 2021 compromises the validity of standard log-linear regression. To ensure continuity and reliability of estimation, we supplemented the analysis using segmented regression and the two-point method, as described in the Methods section. Nonetheless, EAPC estimates remain missing (NA) for certain locations, limiting direct comparability of temporal trends over the full 1990-2021 interval. To mitigate this limitation, we additionally calculated the total TPC from 1990 to 2021 as a descriptive measure of overall burden fluctuation. The integration of these data indicates that the majority of nations and regions have observed an increase in the burden of PC related to high BMI. For instance, in the Global, the EAPC for ASMR was 4.77% (95% CI: 4.41-5.14), while the TPC reached 3.30% (−17.68 to 22.21). However, TPC fails to capture nonlinear trends or inflection points during intervening years. An illustrative example is the Middle SDI region, where the total number of deaths increased markedly between 1990 and 2021, yet the TPC was negative due to the lack of attributable burden in the baseline year. By contrast, the EAPC estimated via segmented and two-point methods yielded positive values consistent with the expected trajectory (Table 2). Consequently, changes in the burden of high BMI-related PC require assessment using both EAPC and TPC. Age-Standardized Mortality Rate (ASMR) and Its Total Percentage Change (TPC) for Pancreatic Cancer Attributable to High BMI Across Countries and Territories, 1990-2021. (A) ASMR in 1990; (B) ASMR in 2021; (C) Total Percentage Change (TPC) of ASMR, 1990-2021 Change in Mortality and DALYs for Pancreatic Cancer Attributable to High BMI Across Regions, 1990-2021. Detail Values are Available in the Appendix

Sex- and Age-Specific Distribution of PC Attributable to High BMI
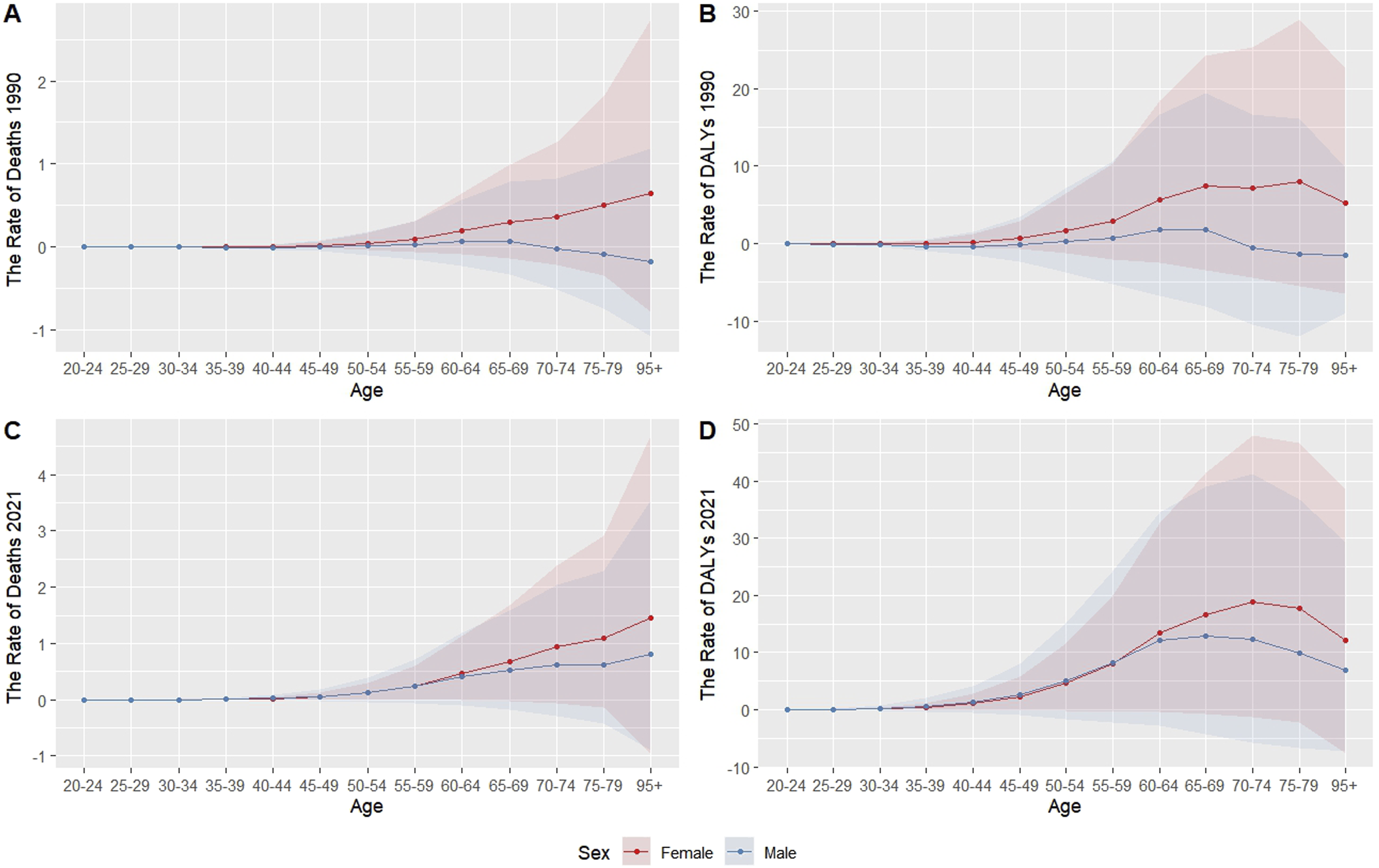
An analysis of sex-specific differences revealed that, in both 1990 and 2021, the total number of deaths and DALYs attributable to high BMI-related PC was consistently higher among females than males (Figure 4). In 1990, the number of male deaths was negative (−12.41; 95% CI: −1342.37 to 2227.20), signifying lack of attributable burden of high BMI on PC deaths in men for that year (Figure 4A). In contrast, female deaths reached 967.05 (95% CI: −751.66 to 3634.38) (Figure 4A). Over the subsequent 31 years, both sexes showed substantial upward trends in death and DALYs. It is worth noting that the number of deaths escalated to 3653.50 (95% CI: −1666.55 to 11,878.32) in males in 2021 (Figure 4C). Age-stratified analysis identified that, in 1990, the number of deaths and DALYs attributable to high BMI-related PC were predominantly concentrated among individuals aged ≥45 years (Figures 4A and B). Significantly, the number of male deaths in the 20-49 and ≥70 age groups was negative, indicating a lack of attributable burden over that period (Figure 4A). In 2021, both deaths and DALYs had dramatically increased across all age groups, with males experiencing a greater magnitude of increase than females in most age groups (Figures 4C and D). Mortality and DALY rates demonstrated consistently higher values among females aged ≥60 years compared to males (both 1990 and 2021) (Figure 5). However, DALY rates among individuals aged ≥70 years exhibited a declining trend in 2021 (Figure 5D). The analysis of the EAPC in ASMR showed that the most significant increases were observed in the 45-49 age group (6.03%, 95% CI: 5.18 to 6.88) and the 80-84 age group (6.54%, 95% CI: 5.96 to 7.12) (Table 3). The Number of Deaths and DALYs Attributed to High BMI-Related Pancreatic Cancer, in 1990 and 2021, Differentiated by Gender and Age. (A) Number of Deaths in 1990; (B) Number of DALYs in 1990; (C) Number of Deaths in 2021; (D) Number of DALYs in 2021. Bar Plots Show the Number of Deaths and DALYs from Pancreatic Cancer Attributable to High BMI Across Age Groups in 1990 and 2021, Stratified by Sex. Red Bars Represent Females; Blue Bars Represent Males Death and DALYs Rates Attributable to High BMI-Related Pancreatic Cancer by Sex and Age, in 1990 and 2021. (A) Death Rate in 1990 by Age and Sex; (B) DALY Rate in 1990 by Age and Sex; (C) Death Rate in 2021 by Age and Sex; (D) DALY Rate in 2021 by Age and Sex. Line Charts Illustrate Age-specific Death and DALY Rates Attributable to High BMI-Related Pancreatic Cancer for Males and Females in 1990 and 2021. The Hatched Section Shows 95% Confidence Intervals Change in ASMR for Pancreatic Cancer Attributable to High BMI Across Age Groups , 1990-2021

Decomposition Analysis of PC Mortality Attributable to High BMI
From 1990 to 2021, multiple factors contributed to the rising deaths attributable to high BMI-related PC, primarily including aging, population growth, and epidemiological changes (Figure 6). Globally, these three factors resulted in an increase of 8260.71 deaths from high BMI-related PC during the 31-year period: 13.88% due to aging, 25.84% due to population growth, and 60.28% due to epidemiological variations—the main cause in the world of deaths attributable to high BMI-related PC (Table 4). While the impact of epidemiological change was more pronounced in men (71.36% increase), it was also the leading contributor to female deaths (52.79% increase) (Table 4). In addition, aging and population growth exerted greater effects on females than males (Table 4 and Figure 6). Decomposition Analysis of Changes in Deaths Attributable to High BMI-Related Pancreatic Cancer by Sex, 1990-2021. The Decomposition Analysis Calculates the Relative Contributions—Population Growth, Aging, and Epidemiological Changes—to the Number of Deaths from Pancreatic Cancer Due to High BMI Between 1990 and 2021. The Black Dots in the Figure Represent the Cumulative Effect of These Three Factors. The x-axis Represents the Number of Deaths; The y-Axis denotes Males, Females, and Both Genders The Relative Contributions of Three Factors—Population Growth, Population Aging, and Epidemiological Changes—To the Number of Deaths From Pancreatic Cancer Attributable to High BMI Around the World From 1990 to 2021

Inequality Analysis of PC Attributable to High BMI
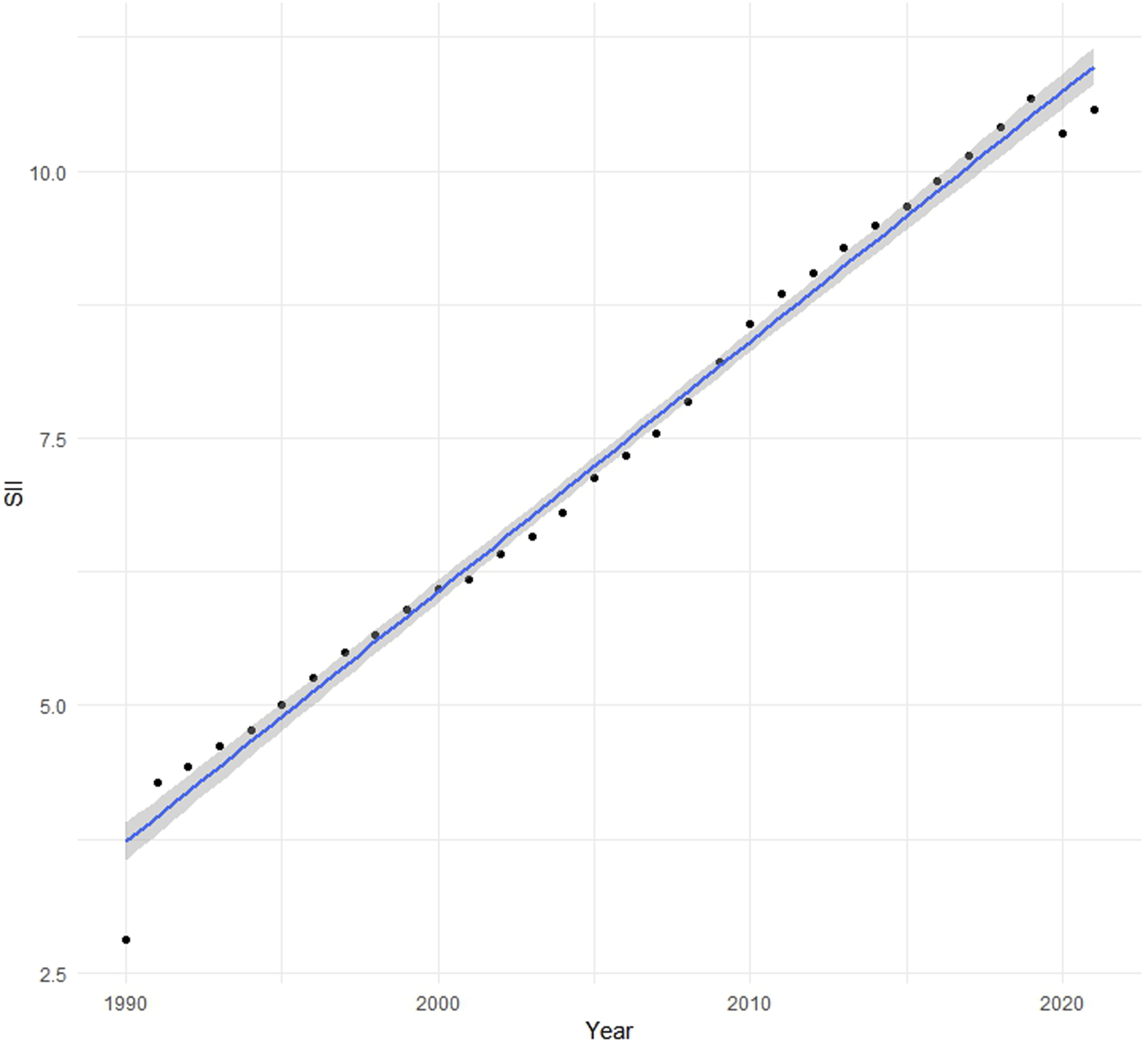
Between 1990 and 2021, the SII for PC attributable to high BMI exhibited a consistent increase, rising from 2.82 (95% CI: 2.79-4.44) per 100,000 population in 1990 to 10.59 (95% CI: 9.99-13.32) in 2021 (Figures 7 and 8). This upward trend reflects a positive correlation between ASDR and the SDI. The marked increase in SII highlights a widening inequality in the burden of high-BMI-related PC between high- and low-income countries over the past three decades Absolute Income-Related Healthy Inequality in the Burden of High BMI-Related Pancreatic Cancer, 1990 vs 2021. Each Dot Represents a Country, Sized by Population; the x-axis Shows Countries Ranked by SDI (From Lowest to Highest), and the y-axis Shows Age-Standardized DALY Rates (ASDR) per 100,000 Population; Lines Represent the Slope Index of Inequality (SII) for 1990 and 2021; Labels Highlight China and India as High-Population Countries The Trendline Demonstrates the Trend in Slope Index of Inequality (SII) for Age-Standardized DALY Rates (ASDR) Attributable to High BMI-Related Pancreatic Cancer From 1990 to 2021. Points Represent Annual SII Estimates for ASDR Across Countries Ranked by SDI, and the Blue Line Shows the Fitted Linear Trend. An Increasing SII Indicates Widening Inequality in Disease Burden
Joinpoint Regression Analysis of PC Attributable to High BMI
Joinpoint regression analysis was conducted to evaluate temporal trends in the ASMR and ASDR of PC attributable to high BMI. However, due to negative ASMR and ASDR values among males from 1990 to 1992, which were unable to be calculated, Joinpoint analysis was performed using data from 1992 to 2021. From 1992 to 2021, both ASMR and ASDR of BMI-related PC were higher in females than in males and the total population (Figure 9). Three groups (male, female, and total) all showed an upward trend in the ASMR and ASDR of BMI-related PC during this time (Figure 9). The AAPC of ASMR during 1992-2021 in total was 4.51% (95% CI: 4.34 to 4.69, P < 0.000001), 2.99% (95% CI: 2.83 to 3.15, P < 0.000001) for females, and a significantly higher 14.87% (95% CI: 11.61 to 18.24, P < 0.000001) for males (Table 5). Although females maintained higher ASMR and ASDR over time, the difference between groups narrowed due to the sharp increase in males (Figure 9). These findings suggest that while the burden remained greater in females, the growth rate of PC attributable to high BMI was substantially higher in males. Detailed values are provided in Table 5. Joinpoint Regression Analysis of Global Burden of Pancreatic Cancer Attributable to High BMI, 1992-2021.(A) Trends in ASMR, by Sex and Overall; (B) Trends in ASDR, by Sex and Overall; (B) Trends in ASMR, by Sex and Overall. The Curves Represent Sex-Specific and Combined-Sex Trends With Identified Joinpoints. The APC Values and Corresponding Time Segments are Indicated on the Right of the figure. Asterisks (*) Denote Statistically Significant APC (P < 0.05) Trends in ASMR and ASDR for Pancreatic Cancer Caused by High BMI Around the World From *P < 0.05. AAPC: Average Annual Percent Change. APC: Annual Percent Change.

Age-Period-Cohort(APC) Effects on PC Mortality Attributable to High BMI
Figure 10 illustrates the age–period–cohort (APC) effects on mortality rate attributable to high BMI-related PC. Mortality rates began increasing from ages 20-24 and peaked at ages 75-79. Figure 10A and C exhibit a sustained increase in mortality rates with age, but the rate of growth declined with advancing age. Analysis by birth cohort further revealed that within each age group, mortality rates rose with later birth years (Figures 10D and B). Age, Period, and Birth Cohort Effects on the Death Rate in High BMI-Related Pancreatic Cancer by APC Models. (A) Mortality Trends by Age Group Across Time; Each Line Represents a 5-Year Interval. (B) Mortality Trends by Age Across Birth Cohorts; Each Line Denotes a 5-Year Cohort. (C) Mortality Trends by Age Groups Across Diagnostic Year; Each Line Corresponds to a 5-Year Age Category. (D) Mortality Trends Across Age Groups for Consecutive Birth Cohorts; Each Line Indicates a 5-Year Age Group
A stratified analysis of various age groups from 1992 to 2021 shows mortality rates attributable to high BMI-related PC rose in all age groups. In addition, mortality rates increased more slowly in age groups ≥50 compared to younger groups across all cohorts. It is worth noting that among younger age groups, such as those aged 35 to 39, the mortality rate from high BMI-related PC showed a substantial increase from 2005 to 2010, followed by a slower growth rate. This signifies a crucial turning point in the mortality trend for this age group. In contrast, for other older age groups, the mortality rate reached a significant turning point primarily between 2000 and 2005 (Figure 10C).
Twenty-Year Projection of PC Mortality Attributable to High BMI
Forecasts of the burden of high BMI-related PC from 2022 to 2041 showed that the ASMR in the overall population will constantly increase, as well as in both females and males (Figure 11). In 2041, the ASMR for males will increase from 0.09 per 100,000 (95% UI: −0.04 to 0.30) to 0.14 per 100,000 (95% CI: 0.09 to 0.19). Female ASMR will increase from 0.12 per 100,000 (95% UI: −0.01 to 0.31) to 0.18 per 100,000 (95% CI: 0.15 to 0.21). Although females will maintain a constantly higher mortality rate than males, the increase rate will be lower. In summary, over the next 20 years, the burden of high BMI-related PC is expected to increase. Trends and Forecast of Age-Standardized Mortality Rate (ASMR) Attributable to High BMI-Related Pancreatic Cancer by Sex, 1990-2041. (A) ASMR of Males From 1990 to 2041; (B) ASMR of Females From 1990 to 2041; (C) ASMR of Both Sexes Combined From 1990 to 2041.The Red Lines Represent Observed Age-Standardized Mortality Rates (ASMR) From 1990 to 2021, and the Yellow Dotted Lines Represent Projected ASMR From 2022 to 2041 Based on ARIMA Models. Vertical Dashed Lines Indicate the Start Year of the Forecast Period
Discussion
Based on GBD 2021 data, we found that both the number of deaths and DALYs from high BMI-related PC increased nearly tenfold globally between 1990 and 2021. The Middle SDI region exhibited the most pronounced rise, but the largest absolute number of deaths was found in the High SDI region, followed by High-Middle SDI, Middle SDI, and Low-Middle SDI, and finally the Low SDI. Interestingly, although the high SDI region recorded the highest number of deaths in both 1990 and 2021, the increase was only fivefold—representing the smallest rise among all five SDI regions, compared with more than sevenfold increase in other regions. The reason why high-income regions like the USA and Australia have the heavy burden of high BMI-related PC is primarily attributed to high obesity prevalence. Long-term consumption of high-fat diets and high-sugar foods, lack of physical activity, population aging, and low birth rates collectively result in an increased population of high BMI in those areas.23-25 However, due to their better economic conditions, specific health programs and precautionary policies have been established there,23,26 accompanied by enhanced education against the adverse effects of overweight. Thus, even though the underlying burden is heavy, the burden of PC in relation to high BMI appears to have progressed more slowly in the past decade compared to others. Meanwhile, although the burden of PC attributable to high BMI in middle- and low-income regions is still lower than that in high-income countries, its relative increase has become more significant in recent years.
Projections about the future economic impact of PC indicate that the most significant increases in total costs will occur in low-income regions. Specifically, from 2019 to 2060, the overall economic burden in high-income nations would quadruple, while low- and lower-middle-income countries will have a 12- to 25-fold rise in total disease-related costs. 26 The evolving patterns of epidemiology are closely shaped by changing socioeconomic conditions in middle- and low-income nations. In resource-constrained settings, survival-oriented priorities often overshadow preventive health behaviors. Consequently, the risks associated with high BMI do not manifest in a significant mortality burden initially. 23 During the transformative phase of economic restructuring, characterized by a significant increase in commodity prices and sharp wealth disparity, behavioral changes were seen among nutritionally disadvantaged individuals.23,26 Despite a global economic improvement, the use of ultra-processed foods (characterized by long shelf life, high availability, and elevated caloric density) has pronouncedly risen, resulting in a substantial increase in calorie intake, particularly among individuals residing in low-income regions. Obesity, as a chronic condition, further exacerbates systemic deficiencies in healthcare systems of these countries—marked by poor diagnostic infrastructure, fragmented prevention programs, and inadequate long-term treatment. These limitations contribute to an increasing burden of obesity-related illnesses, especially in communities undergoing lifestyle transitions.27,28
Overall, these findings highlight that the global health inequality in the burden of high BMI-related PC,29,30 along with its underlying mechanisms, may be attributed to three pathways: (1) Obesogenic high-income environments: Among high-income countries, a longstanding cultural appetite for high-calorie diets and physical inactivity has created an obesogenic atmosphere that perpetually boosts risks of PC. Even with interventions such as sugar-sweetened beverage taxes (eg, the UK Soft Drinks Industry Levy 31 ) and healthy food subsidies (eg, the US Supplemental Nutrition Assistance Program 32 ), reductions in obesity-related mortality have been modest, as deeply rooted dietary behaviors continue to sustain a high disease burden. (2) Developing countries nutritional shift: While global assistance programs have driven economic improvements in low-income countries, paradoxically, they have also accelerated the transition to energy-dense diets. Prioritizing resource allocation towards food availability rather than nutritional quality has resulted in surging obesity rates and rising PC burdens.33,34 (3) Healthcare system deficiencies: In low-income areas, the presence of chronic disease management deficiencies leads to inadequacies in diagnosis and treatment. The progression of obesity-related conditions, combined with the vague symptoms and high treatment costs of PC, often leads to late-stage diagnoses in low-resource settings.6,33 To alleviate these disparities, we propose a three-pronged intervention framework: (1) High-income countries: Implement thorough obesity education, adopt fiscal policies to reshape dietary patterns, and accelerate precision medicine research for early detection of PC. (2) Middle- and low-income countries: Develop nutrition education programs in culturally appropriate ways and establish community-level screening systems targeting high-risk populations. (3) International coordination: Enhance international coordination on food policy governance, promote a universal strategy for appropriate healthy diets, and implement tailored interventions. These interventions may include BMI surveillance programs in developed countries and increased investment in healthcare infrastructure in developing nations.
From 1990 to 2021, the global mortality burden of PC attributable to high BMI underwent marked shifts in both gender and age structures. Spanning the 31-year observation period, the total mortality burden of PC attributable to high BMI was still higher in women than in men. However, the growth rate of the burden among men was faster, with an ASMR AAPC of 14.87% (95% CI: 11.61-18.24, P < 0.000001). Additionally, these results indicated a trend of the burden shifting from older age groups to younger ones. Among women, compared to 1990, the number of deaths in the 20-49 age group increased by 7-12-fold in 2021, exceeding those aged 50 and above (the 4-7-fold increase); this trend was even more remarkable among men. The above phenomena show that the epidemiological characteristics of PC associated with high BMI are undergoing a significant transition: from a pattern dominated by women toward a diminishing gender gap due to the swift rise in the male burden, and from a pattern dominated by the elderly toward a younger group.
The higher burden of PC attributable to high BMI observed in women may stem from multiple factors, including physiological metabolism, behavioral habits, and social environment. Studies show that women generally have higher levels of leptin than men and a greater distribution of brown adipose tissue. These characteristics may enhance energy storage tendencies, thereby increasing the susceptibility of individuals to obesity.35,36 Additionally, hormonal changes amid pregnancy may affect the risk of PC—certain surveys suggest that higher parity may be associated with reduced risk, but declining global fertility rates in recent years have weakened this protective mechanism.37-39 At the behavioral level, some cross-sectional studies have indicated that women are more likely to consume high-calorie sweets and engage in less physical activity than men. 40 Moreover, women tend to experience greater role strain and psychological stress in both family and workplace contexts, which may indirectly contribute to increased obesity risk.39-42
In contrast, the rapidly escalating mortality burden among men in recent years is likely associated with the increasing prevalence of central obesity and evolving socioeconomic dynamics. Biologically, males exhibit a greater susceptibility to visceral fat buildup, a phenomenon closely linked to an increased risk of PC.40,43 Furthermore, the accelerating pace of life and rising socioeconomic pressures—particularly affecting younger male populations—have exacerbated obesity rates and, in turn, the burden of PC in this demographic.37,42
Accordingly, tailored strategies should consider gender- and age-specific differences, particularly middle-aged and younger males, who have shown a rapidly increasing burden. Public awareness of obesity-associated diseases, such as PC, requires enhancement, psychosocial burdens necessitate mitigation, and physical activity merits greater emphasis. Men in this age group need to be encouraged to reduce sedentary behavior, prevent the buildup of excess belly fat, and support extended paternity leave where available. Furthermore, health assessments and disease screenings had better be provided to individuals employed in high-stress occupations, such as transportation, security, and construction, to mitigate the incidence of PC.
In addition, we noted that the reasons for the persistently higher burden of PC with high BMI in women, beyond physiological and behavioral factors, may also be influenced by social structural inequalities. In several middle- and low-SDI countries, women continue to face multiple disadvantages in education, healthcare, and social status. They are forced into higher levels of stress and inequality due to childbearing, family responsibilities, limited labor market participation, and sustained psychological strain. Such factors as those mentioned above increase the prevalence of obesity among women and indirectly exacerbate their pancreatic cancer burden.41,42,44 Despite the implementation of initiatives such as the United Nations’ Women’s Empowerment Principles, 45 the Beijing+30 Platform for Action, 46 and the Expanded Family and Medical Leave Act, 47 which have somewhat slowed the rate of increase in BMI-related PC among women in recent years, the deeply ingrained cultural norms and uneven global implementation of these measures continue to hinder substantial progress. This reality highlights that the fundamental social determinants of the long-term gendered disparity in PC burden remain largely neglected.
With the obesity burden in women still increasing, national public health system should offer more positive, multi-faceted solutions to prevent the increase of obesity-related diseases. Specifically, policies should (a) aim to reduce the costs of purchasing micronutrient-rich foods, 48 (b) intensify population-wide awareness campaigns targeting gender-specific metabolic risks, 35 and (c) improve workplace structures for women—specifically by extending the duration of paid maternity leave (18+ weeks)—as well as providing support for stress reduction to relieve reproductive and employment-related burdens. 48 In aggregate, these measures could mitigate gender-based health disparities in high BMI-related PC.
Conclusion
In summary, the burden of high BMI-related PC has increased from 1990 to 2021. Females and older groups have been much more severely affected, whereas the rate of increase is sharper among males and younger groups. Meanwhile, health inequalities persisted across the world during this period. Therefore, countries and regions must implement relevant strategies to overcome these increasingly expanding issues. In addition, international collaboration is necessary to reduce disparities in medical infrastructure and preventive capacity.
Limitation
This research also has several limitations. First, the quality of primary data in some low-SDI countries remains limited, which may affect the accuracy and representativeness of disease burden estimates. Second, due to the presence of zero or negative values for ASMR and ASDR data in some countries and regions between 1990 and 2021, standard linear regression methods are not fully applicable, resulting in missing EAPC estimates for some regions. Although this study used two-point estimation and segmented estimation to address missing values and retain as much of the dataset as possible, these adjustments still affect the trend comparability between countries and regions. Hence, future investigations should prioritize high-quality, complete data and refine modeling methods to achieve more robustness and interpretability in trend evaluation.
Supplemental Material
Supplemental Material - Reversed Gender Burden of Pancreatic Cancer Attributable to High BMI: A GBD 2021 Analysis of 204 Countries With Projections to 2041
Supplemental Material for Reversed Gender Burden of Pancreatic Cancer Attributable to High BMI: A GBD 2021 Analysis of 204 Countries With Projections to 2041 by Ruishuang Chen and Junping Wei in Cancer Control.
Supplemental Material
Supplemental Material - Reversed Gender Burden of Pancreatic Cancer Attributable to High BMI: A GBD 2021 Analysis of 204 Countries With Projections to 2041
Supplemental Material for Reversed Gender Burden of Pancreatic Cancer Attributable to High BMI: A GBD 2021 Analysis of 204 Countries With Projections to 2041 by Ruishuang Chen and Junping Wei in Cancer Control.
Footnotes
Acknowledgement
The authors appreciate the work by the GBD 2021 collaborators and all who helped with this study.
Ethical Approval
This study complies with the GATHER guidelines. The data employed in this study are aggregated, ensuring that no information of individual patients or public personnel is directly implicated.
Author Contributions
Ruishuang Chen: data acquisition and analysis; manuscript writing; data visualization;Junping Wei: manuscript writing, review, and/or revision, funding acquisition.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Source of funding for this research: Special Project on Clinical Evidence-based Research of Traditional Chinese Medicine under the Project for Improving the Clinical Research and Outcome Transformation Capabilities of High-level Traditional Chinese Medicine Hospitals at the Central Level (HLCMHPP2023084).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.