
Abstract
Introduction
Colorectal cancer (CRC) is the second most prevalent cancer in Saudi Arabia, with a rising incidence among younger adults. Despite the known benefits of early detection and screening, public awareness and screening uptake remain limited. Understanding knowledge, attitudes, and determinants of screening and diagnosis is essential to guide public health interventions and policies.
Methods
This cross-sectional study was conducted between August 2024 and January 2025 among adults aged 18 years and older across Saudi Arabia using a validated Arabic-language self-administered questionnaire. Data were analyzed to assess CRC knowledge, screening practices, and diagnostic patterns, as well as their sociodemographic determinants.
Results
A total of 2113 participants (mean age: 34 ± 9.6 years; 74% female) completed the survey. Overall, 53% demonstrated good CRC knowledge, while screening prevalence was notably low (2%), and 2.1% reported a prior diagnosis. Higher knowledge was observed among males, participants with higher income, and those reporting frequent fiber intake. Higher BMI was associated with lower screening uptake, whereas education level and income influenced diagnosis likelihood. Age was significantly associated with both screening and diagnosis outcomes.
Conclusions
This study highlights moderate CRC knowledge and low screening participation among Saudi adults. Targeted national awareness campaigns, integration of CRC screening into primary healthcare, and digital outreach for younger populations are recommended to enhance early detection, promote preventive practices, and reduce the national CRC burden.
Plain Language Summary
This study from Saudi Arabia looked at how much people know about colorectal cancer (CRC), how often they get screened, and what factors affect these things. It found that while over half of the 2113 adults surveyed had good knowledge about CRC, very few had actually been screened (only 2%) or diagnosed (2.1%). Men, people with higher incomes, and those who ate more fiber knew more about CRC. People with higher body weight were less likely to get screened. Interestingly, those with higher education were less likely to be diagnosed. The study suggests that more effort is needed to raise awareness and improve access to screening to catch CRC early, especially among younger adults.
Introduction
Colorectal cancer (CRC) is one of the most commonly diagnosed malignancies and a leading cause of cancer-related deaths worldwide. 1 It is the third most diagnosed cancer globally and the second leading cause of cancer-related mortality, accounting for approximately 10% of all cancer cases and over 1.9 million new diagnoses annually. 2 By 2040, the global CRC burden is projected to rise by 63%, reaching 3.2 million new cases and 1.6 million deaths, with high-income countries being most affected.2,3 In Saudi Arabia, CRC has emerged as the most common cancer among men and the third most common among women, with an increasing incidence over the past decade. 4 Alarmingly, recent epidemiological shifts reveal a growing incidence in younger Saudi adults (<50 years), diverging from traditional patterns where CRC predominantly affects older populations. 5 Regional disparities are also evident: Jazan reports the lowest age-standardized incidence rates (ASIRs) at 2.7-3.1 per 100 000, whereas Riyadh and the Eastern Province show higher rates (7.5-9.2 per 100 000).4,6,7
CRC develops through a complex interaction of non-modifiable factors like age, male sex, and hereditary conditions such as familial adenomatous polyposis (FAP).3,5 Conversely, modifiable lifestyle factors—such as obesity, physical inactivity, excessive red meat consumption, smoking, and alcohol use—significantly contribute to CRC risk.3,5 In Saudi Arabia, these modifiable risks are particularly concerning, given the high prevalence of obesity (>35%) and physical inactivity (affecting 60% of adults). 8 Additionally, dietary transitions toward processed foods and low fiber intake, driven by urbanization, have been implicated in the rising CRC incidence. 9 Symptoms such as altered bowel habits, rectal bleeding, abdominal pain, unintended weight loss, and anemia often appear only at advanced stages of the disease, underscoring the critical importance of early detection and routine screening for improving outcomes and survival rates.
Despite rising CRC rates, screening in Saudi Arabia faces barriers such as fear of invasive procedures, gender-related cultural hesitancy, and low physician referral rates due to time constraints. 10 Geographic disparities in healthcare access further compound these challenges, with rural regions experiencing prolonged endoscopy of wait times exceeding six months in some provinces. 11 Current research on CRC in Saudi Arabia remains limited, characterized by small cohort studies (<500 participants) that fail to holistically assess behavioral risk factors, public knowledge, and diagnostic barriers.12,13 Notably, no prior study has concurrently examined CRC-related risk behaviors, symptom recognition, and screening attitudes—a critical gap that impedes the development of targeted prevention strategies. To address these limitations, this study employs a large-scale, cross-sectional survey of approximately 2000 adults in Saudi Arabia. By integrating quantitative assessments across these domains, this research aims to examine CRC knowledge scores, screening and diagnosis rates, as well as the determinants of these factors among residents of Saudi Arabia. The findings aim to focus on the need for screening programs, health campaigns, and policy reforms to mitigate the growing burden of CRC in Saudi Arabia.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted across Saudi Arabia using an online, self-administered questionnaire. Data collection targeted adults aged 18 years and older residing in the country. The study was conducted between August 2024 and January 2025. The age inclusion criterion of ≥18 years was chosen to capture knowledge and awareness of CRC risk factors and screening across the adult population in Saudi Arabia, not only those within the clinical “at-risk” age group. The reporting of this cross-sectional study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 14
Sample Size and Sampling Technique
Cochran’s formula was used to determine the required sample size. The initial sample size (n0) for an infinite population was calculated as follows:

Where: Z = 1.96 (for 95% confidence level) p = (assumed proportion) e = (margin of error)

Since the study population was finite, the sample size was adjusted using the finite population correction formula:


The minimum required sample size was 1068 participants. To improve statistical accuracy and address missing or incomplete responses, the final sample size was increased to 2113 participants. Convenience sampling was used to collect data from participants in the general population of Saudi Arabia through an online questionnaire.
Data Collection Tools
A self-administered online questionnaire was created using Google Forms to collect data from the general population of Saudi Arabia. Adapted from previous studies,16–18 it was translated into Arabic. The questionnaire included five sections: (i) sociodemographic and health-related behaviors, (ii) nutritional characteristics over the previous 6 months (iii) health conditions linked to CRC risk, (iv) CRC knowledge and screening participation, and (v) CRC diagnosis.
To evaluate participants’ knowledge of CRC risk factors, a structured-validated Arabic questionnaire was used. 15 The questionnaire included 15 close-ended “Yes” or “No” items on CRC risk factors, with one point for each correct response (score range: 0-15). Participants scoring ≥9 were categorized as having good knowledge, and ≤8 as poor knowledge. The total knowledge scores were normally distributed; therefore, the mean score was used as the cut-off, with participants scoring ≥mean categorized as knowledgeable and those scoring <mean categorized as not knowledgeable.
To ensure the tool’s validity, reliability, and clarity, a pilot test was conducted among 40 participants. Survey was deployed on a small group first. This helps identify confusing questions, poor wording, or technical issues that lead to frustration and satisficing. It ensured reduced response bias. Based on their feedback, minor revisions were made to enhance the questionnaire before final deployment. Participants were recruited using a convenience sampling method. The online questionnaire was distributed through widely used social media platforms such as Telegram, WhatsApp, X (formerly Twitter), Facebook, and other widely used channels which reduces sampling bias. To minimize social desirability bias, no personal identifiers were collected. Participants were presented with a clear description of the goals of study and informed permission was gained before participation.
Demographic information on individuals who declined to participate or did not complete the questionnaire could not be collected, as participation was entirely voluntary and anonymous. However, to ensure data quality, all responses were screened for completeness. A total of 7% incomplete submissions were excluded from the analysis, and only fully completed questionnaires were retained in the final dataset.
Statistical Analysis
Data were coded and analyzed using Microsoft Excel and R software (version 4.2.3). Descriptive statistics included means ± standard deviations for continuous variables and frequencies and percentages for categorical variables. The unpaired t-test was used to compare means of continuous variables between two independent groups, while the chi-square test was applied to assess associations between categorical variables, as these tests are suitable for normally distributed and categorical data, respectively. Multiple regression analyses were conducted to identify determinants of CRC knowledge and risk factors, with results reported as beta coefficients and odds ratios (OR) with 95% confidence intervals (CI). Statistical significance was set at P < 0.05. Bar plots were used to visualize CRC knowledge, screening, and prevalence. No formal sample size calculation was performed for this study; however, a total of 2113 participants were included, providing sufficient data for exploratory analysis.
Ethical Considerations
Participants were selected on a voluntary basis, and informed consent was acquired before participation. Ethical approval for this study was obtained from the Scientific Research Ethics Committee of Jazan University, Jazan, Saudi Arabia (Approval No. REC-45/11/1127, dated 02/06/2024). As the study involved human participants completing an online questionnaire, informed consent was obtained electronically from all participants, and participation proceeded only after consent was provided. The study was conducted in accordance with institutional ethical standards and the Declaration of Helsinki (1975, as revised in 2024). Participants were properly briefed about the objectives, methods, and their right to cancel their participation at any moment without consequences. All participant information was anonymized through a secure online Google Form that did not record names, email addresses, and no identifiable personal data were collected or stored. Privacy and confidentiality were maintained throughout the study to ensure their voluntary participation.
Results
Sociodemographic Characteristics
The study comprised 2113 participants (mean age: 34 ± 9.6 years; 74% female, n = 1562) with a mean body mass index (BMI) of 27 ± 6.8 kg/m2 (Figure 1). Sociodemographic characteristics revealed that 66% (1394) of participants were married, 29% (n = 612) single, and 5% (n = 107) divorced/widowed. The majority resided in urban areas (58%, n = 1225), while 42% (n = 888) lived in rural communities. Over half (58%, n = 1225) reported a monthly income below 5000 Saudi Riyal (SAR) (1332.78 USD). Approximately half of the participants (52%, n = 1097) held a bachelor’s degree or higher, while 46% (n = 971) completed high school and 2% (n = 45) were illiterate. Lifestyle factors indicated that 87% (n = 1837) were non-smokers, while physical activity levels varied: 22% reported light activity (<30 minutes of medium to intense activity 5 times/week (n = 464)), 28% moderate activity (>30 minutes 5 times/week n = 592)), and 51% (n = 1077) reported no regular physical activity (Table 1). Flowchart illustrating the participant selection process Sociodemographic Characteristics and Health-Related Behavior of Study Participants (n = 2113) Values are presented as Mean ± SD for continuous variables and frequency (%) for categorical variables.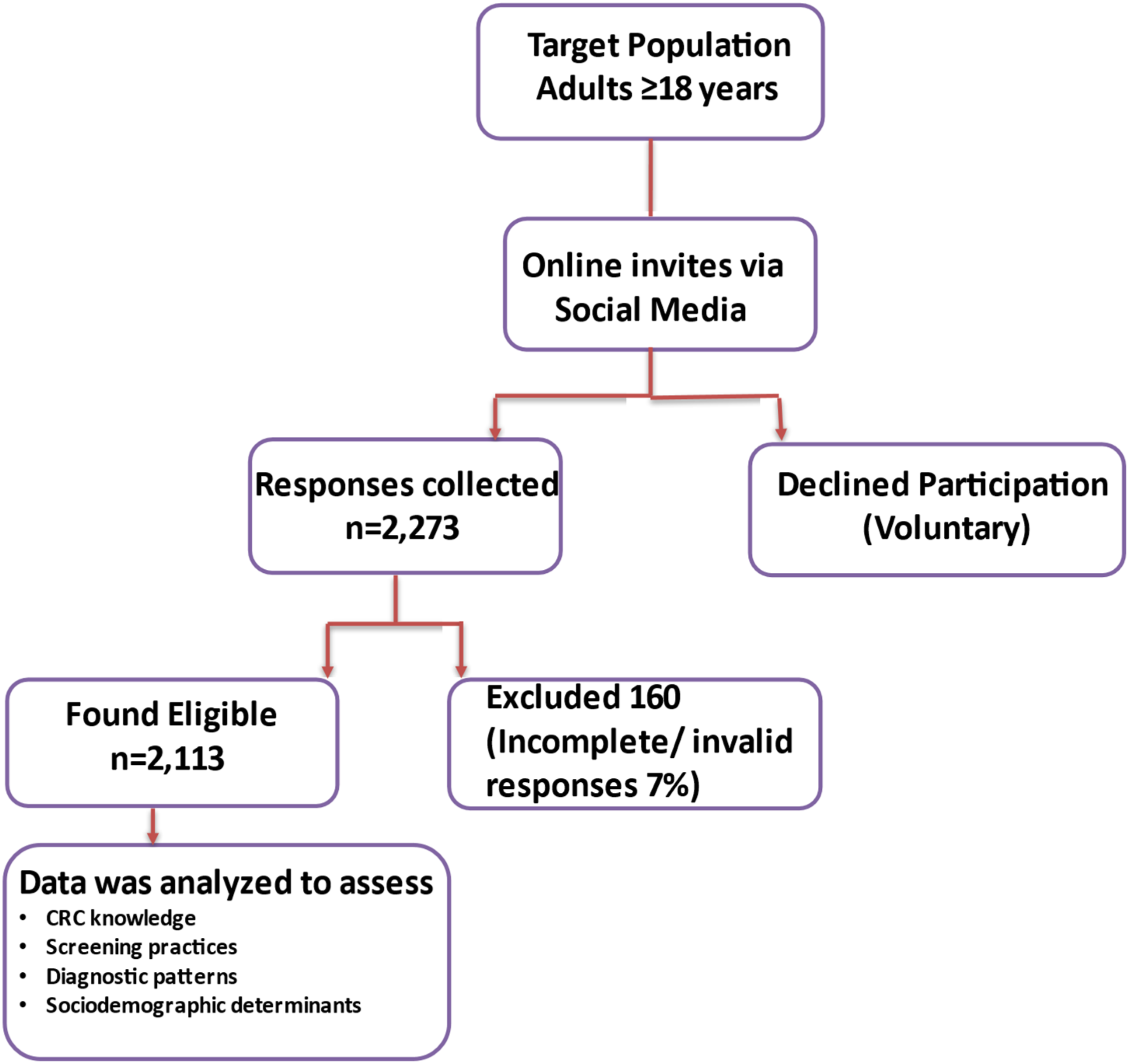

Nutritional Characteristics
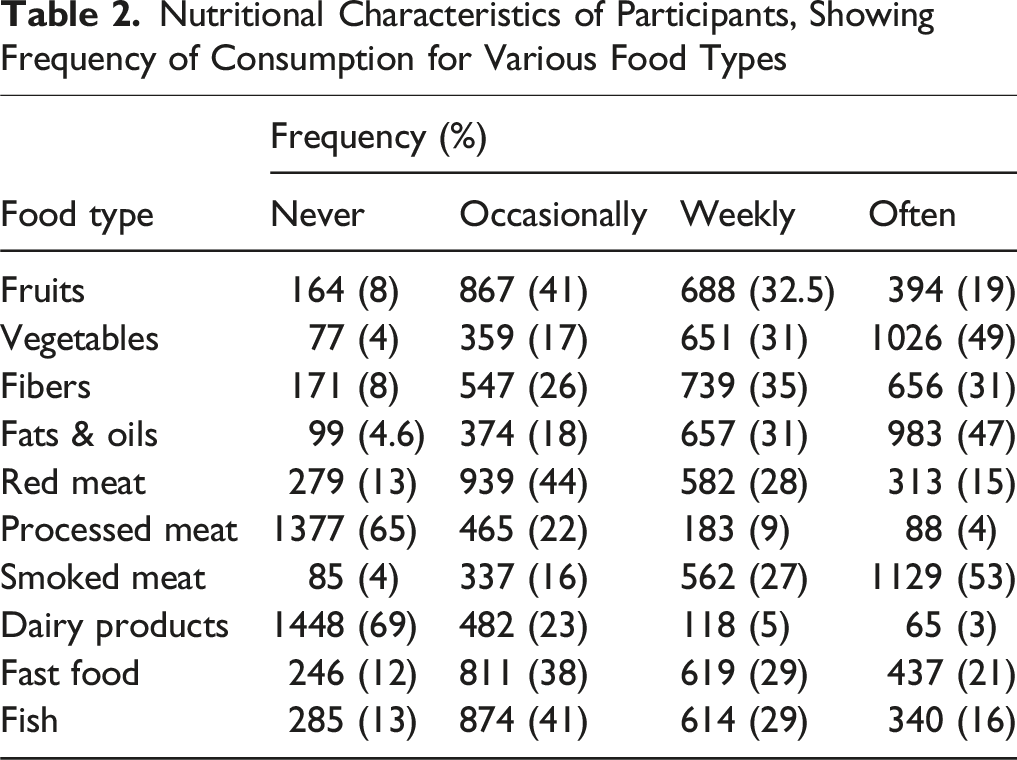
The analysis revealed three primary food groups with the highest consumption frequencies: smoked meat (53%, n = 1129), vegetables (49%, n = 1026), and fats/oils (47%, n = 983). Protein sources showed distinct patterns, with red meat (44%, n = 939) and fish (41%, n = 874) primarily consumed occasionally.
Nutritional Characteristics of Participants, Showing Frequency of Consumption for Various Food Types
Health Conditions Associated with CRC Risk
Prevalence of Health Conditions Associated With CRC Risk among Participants
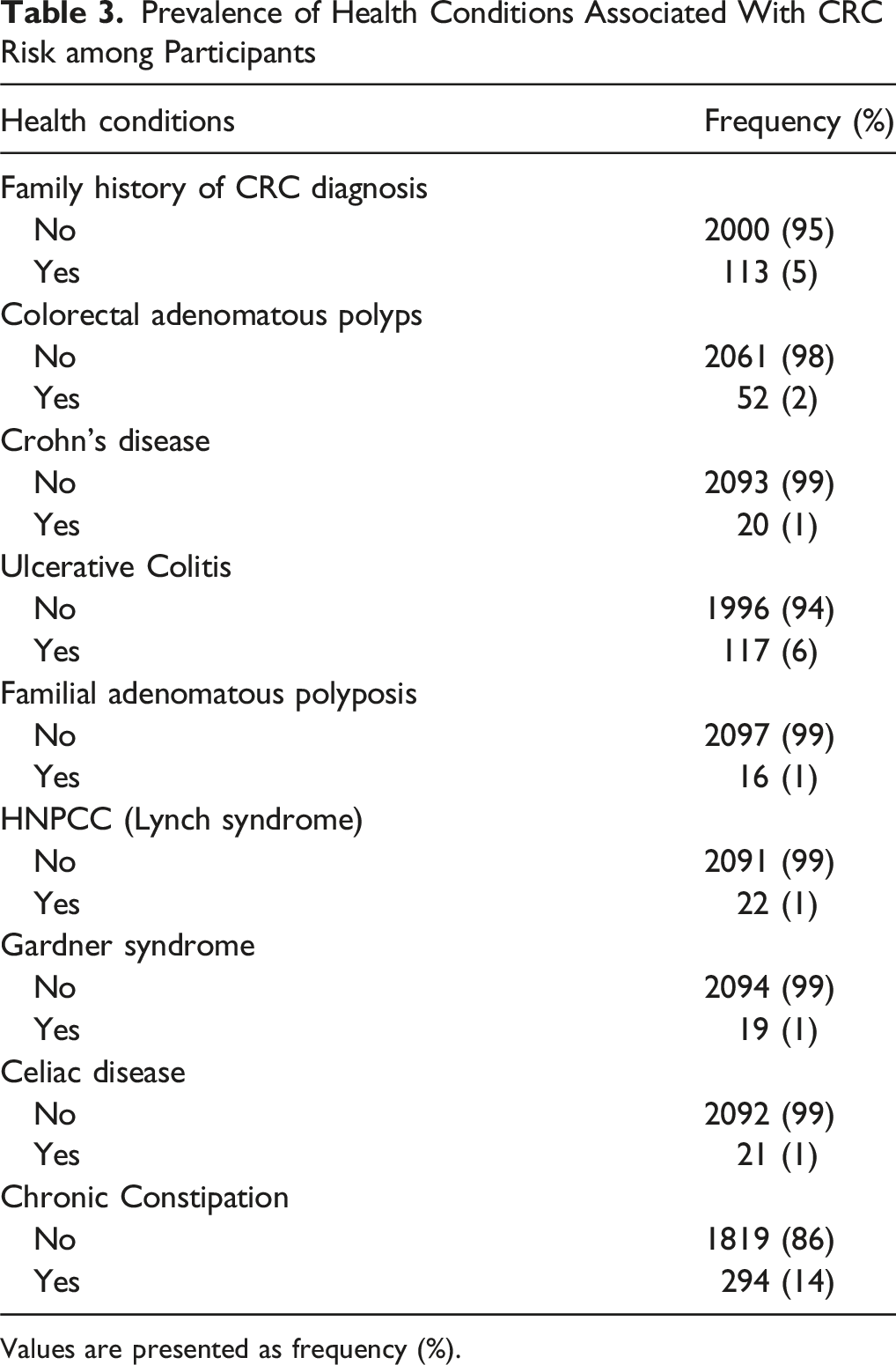
Values are presented as frequency (%).
Participation in CRC Screening and Diagnostic Testing
Participation in CRC Screening and Diagnostic Testing among Study Participants

Values are presented as frequency (%).
Knowledge About CRC Risk Factors among participants
The assessment of CRC knowledge revealed that 53% of participants (n = 1113) demonstrated good understanding, while 47% (n = 1000) showed poor knowledge scores (Figure 2). Regarding risk factor awareness, most participants correctly identified smoking and excessive alcohol consumption as significant CRC risks. Secondary perceived risk factors included elevated stress levels, frequent consumption of fats, and a family history of CRC (Figure 3). Distribution of CRC knowledge among participants (n = 2113). Good vs poor knowledge scores are shown as percentages Participants’ awareness of CRC risk factors. Bars represent the percentage of participants identifying each risk factor correctly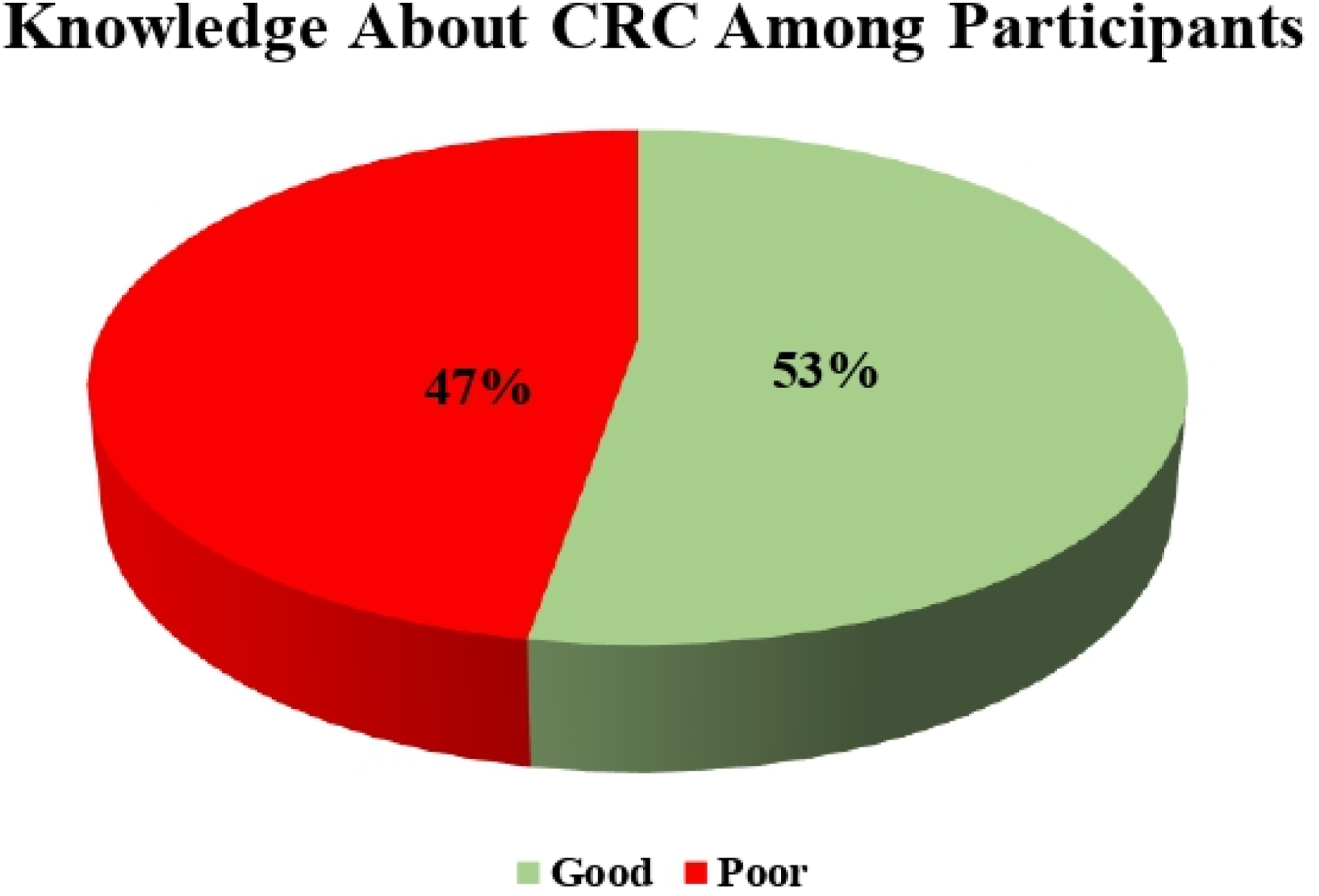

Determinants of CRC Risk Factor Knowledge Among Participants

Multivariable linear regression results are presented with β coefficients, 95% Confidence Intervals (CI), and P values.
Note: * indicates statistical significance at P < 0.05.
Logistic Regression of Factors Associated With CRC Screening Participation (n = 2113)

OR = Odds Ratio; 95% CI = Confidence Interval and P Values.
Note: * indicates statistical significance at P < 0.05.
CRC Diagnosis Among Participants
Logistic Regression of Factors Associated With Self-Reported CRC Diagnosis (n = 2113)

OR = Odds Ratio; 95% CI = Confidence Interval and P Values.
Note: * indicates statistical significance at P < 0.05.
Discussion
This study provides a critical analysis of CRC awareness, knowledge, and screening practices among 2113 adults in Saudi Arabia. It revealed varying awareness levels and notable gaps in understanding and participation in screening programs. These findings add to existing CRC literature and have important implications for health strategies aimed at improving awareness and screening uptake in the region.
A key finding of this study revealed that 53% of participants demonstrated “good” understanding of risk factors related to CRC, indicating a moderate level of awareness within the general population of Saudia. Literature showed comparable patterns in other Saudi regions: Khamjan et al. (2021) found that only 50% of medical students at Jazan University had moderate CRC knowledge, while 49.8% were unaware that CRC is a leading cancer that affects both genders significantly. 8 Alsajgh et al. reported that 57.3% of adults in Qassim region had poor awareness, while only 4.2% showed good understanding. 19 Similarly, Imran et al. showed that 82.3% of medical students in Jeddah were aware of CRC, only 50-60% understood its risk factors and symptoms. 20 These results suggested that even among educated groups, comprehensive CRC knowledge remains insufficient. In contrast, Khraiwesh et al. reported significantly higher awareness (83.9%) among Jordanian university students. This discrepancy may be attributed to the scientific/academic background of 70 % participants in Khraiwesh’s study. 18
Comparative evidence from other Arab countries underscores the widespread nature of knowledge and screening gaps. In Egypt, a national survey of 940 adults found that 71% had poor knowledge of colorectal cancer, with only 29% reaching a “good” knowledge threshold. 21 A Syrian cross-sectional study (n = 772) revealed that while 54.8% had heard of colonoscopy, merely 15.4% had undergone the procedure and only 27.8% considered themselves informed about CRC. 22 In Lebanon (n = 371), 83% were unaware of major CRC risk factors and only 15% reported having been screened; 43% expressed willingness to undergo screening when informed. 23 These findings align with our results of moderate knowledge (53% with “good” knowledge) and extremely low screening uptake (2%). Together, the regional evidence signals a consistent pattern of limited awareness and minimal screening engagement across the Middle East, suggesting that beyond individual sociodemographic variables, broader system and cultural factors may play key roles.
In our study, Male participants in our study showed better CRC knowledge [OR: 0.73; 95% CI: 0.29-1.18; P = 0.001], consistent with Milibari (2023) 24 and another study showing higher CRC screening awareness in men (64.9% vs 35.1%; P = 0.004). 25 This may reflect the higher CRC incidence around 1.5 time’s greater and earlier onset and 4-8 years sooner in males. 26 Social factors may also contribute. Conversely, Al-Hajeili et al. found higher CRC knowledge in females [OR: 1.73; P = 0.021], 11 possibly due to a sample with ∼70% women. Khayyat et al. found no significant gender or age link (P > 0.05), but emphasized education (P = 0.045) as key. 27 Although education is theoretically linked to awareness, our study found no significant association with CRC knowledge, possibly due to non-scientific backgrounds. Awareness may instead come from social media and public campaigns.
The predominance of female participants in this study (74%) may reflect greater engagement of Saudi women with online health surveys and social media platforms, which were the primary recruitment channels. Similar gender patterns have been observed in other digital health studies conducted in the region. 28 Conversely, the very low proportion of respondents reporting a family history of CRC may be attributed to limited familial awareness, fear, or social stigma surrounding hereditary cancers. Individuals with a known family history may also have avoided participation due to the sensitive nature of the topic. These factors could have contributed to participation bias and should be considered when interpreting the results.
Higher income was identified as a critical factor, affecting knowledge level, where higher income reflected improved knowledge scores. Similarly, Supachai et al reported that participants with their own income and income more than 30 000 THB/month participants had higher screening knowledge of 15-fold (OR 15.14, 95% CI 4.72-48.56) and 2.5-fold (OR 2.50, 95% CI 1.50-4.18), respectively. 29 Morey et al also showed higher income of around $100,000 or more was strongly associated with higher CRC knowledge scores (P = 0.00). This is likely due to factors such as better access to information, higher levels of education, and greater awareness of preventative healthcare practices. 30 Additionally, our analysis identified fiber consumption as a factor associated with higher CRC knowledge, an association not widely reported in previous studies. It is scientifically documented that both insoluble and soluble fiber ingestion tend to be beneficial against CRC, showing a clinically significant decrease in CRC risk. 31 Therefore, individuals with good awareness about CRC risk factors tend to consume more fibers.
Moreover, one of the most concerning findings of this study was the extremely low rate of CRC screening (2%) among participants. This is consistent with Alhassan et al., who indicated that, whereas 88% of the participants were familiar with CRC, just 16% had undertaken screening evaluation primarily by colonoscopy. 10 Another survey analysis (2014-2015) by Ni et al showed that despite access to primary care, only 11.5% of previously unscreened patients completed CRC screening within a year, and just 39.9% were up to date overall by 2015. 32 These figures indicate persistently low screening rates in underserved urban populations and suggest that community-based initiatives may be required to enhance overall screening rates.
The low CRC screening rate in our study was largely attributed to the relatively young mean age of participants (34 years), as screening is typically recommended for older adults. Poor knowledge about CRC risk factors and available screening methods also contribute significantly, as supported by Al-Amri et al., who found that only 48% had heard of screening tests, and 46.1% did not know what types of screening tests were available. 9 Similarly, another Saudi study 11 reported that 64.22% of respondents remained unaware of any sort of CRC screening tests. Moreover, psychological barriers such as fear of the procedure and fear of results, along with the absence of symptoms, further deter individuals from undergoing screening.9,11 Cultural beliefs about illness and aging may also play a role, particularly among older individuals who are more likely to fear screening outcomes. 9
Age was significantly associated with CRC screening, with older participants more likely to undergo screening than younger ones (OR = 1.10, 95% CI: 1.06-1.13, P < 0.001). This aligns with Power et al, who found older adults had greater CRC symptom awareness, increasing their likelihood of seeking care. They also more often linked low fiber intake to bowel cancer (67% vs 57%; P < 0.001), while younger individuals were more aware of alcohol-related risks (49% vs 41%; P = 0.009) and age as a risk factor (49% vs 40%; P = 0.004). 33 Another study found that individuals aged ≥70 were 3.38 times more likely to undergo CRC screening. 34 This age-related trend aligns with global practices, as screening guidelines mainly focus on adults aged 50-75 due to the higher CRC risk in older age groups.35,36
Additionally, higher BMI was associated with lower screening rates in our study [OR = 0.91, 95% CI: 0.85 – 0.97, P = 0.004]. Similar findings were reported by Alharthy et al., who observed an obesity rate of 5.2% among participants in Saudi Arabia. 31 One possible explanation is that individuals with obesity may avoid invasive screening due to embarrassment, fear of pain, and body image concerns. Graham et al. also reported that many healthcare professionals lack the skills and comfort to screen patients with high BMI, highlighting the need for training in appropriate techniques, managing refusals, and fostering a weight-inclusive clinical environment. 37 Additionally, only 2.1% of participants in the study had been diagnosed with CRC.
In 2024, Saudi Arabia’s GDP per capita (nominal) was approximately US$ 35 000. 38 By comparison, a monthly income below SAR 5000 (≈US$ 1333), equivalent to about US$ 16 000 annually, falls well below the national average. Such disparities often influence healthcare utilization, as individuals with lower incomes may face financial and structural barriers to screening and timely medical consultations. Conversely, present findings reported that participants with higher incomes were more likely to be diagnosed with CRC, likely due to better access to healthcare services enabling earlier detection. This does not suggest income increases CRC risk but reflects improved diagnostic opportunities. Conversely, Alharthy et al found unemployed individuals were more likely to undergo screening than the employed group (AOR: 1.85; 95% CI: 1.53-2.23). 31 Possibly due to greater availability of time or effective targeting by public health programs.
This study provides novel insights by integrating sociodemographic, dietary, and behavioral factors influencing CRC knowledge and screening in a large, diverse Saudi cohort. Unlike previous studies focused mainly on awareness, it links knowledge with lifestyle factors such as fiber intake and income, offering actionable targets for prevention. These findings fill a key gap in national data and support evidence-based interventions aligned with Saudi Vision 2030.
This study has several strengths, including a large sample size of 2113 participants, enhancing statistical power and relevance to the adult Saudi population. A validated Arabic questionnaire enabled comprehensive assessment of sociodemographics, diet, CRC-related knowledge, and health conditions. The cultural and geographical focus offers valuable insights for tailoring local public health policies. Additionally, detailed analysis of dietary habits helps identify lifestyle-related risk factors for targeted interventions.
Despite its strengths, the study is limited by its cross-sectional design, convenience sampling, self-reported data, and low CRC screening rates, which may affect the reliability of conclusions. The subgroup of participants diagnosed with CRC (n = 45) was small, which may have reduced the statistical power and limited the generalizability of findings related to CRC diagnosis. Since the survey was online and self-administered in Arabic, participation required a minimum level of literacy and digital access. Consequently, individuals who were unable to read or use online platforms were likely underrepresented. In our questionnaire, items on CRC screening history and CRC diagnosis were collected as separate self-reported variables. Although individuals diagnosed with CRC may have also reported undergoing screening (either prior to or during diagnosis), the survey did not explicitly distinguish these responses. Consequently, a degree of overlap between the two groups cannot be excluded. Moreover, no formal sensitivity analyses were conducted to assess the robustness of the findings.
Furthermore, the average age of respondents was 34 years, which is considerably younger than the recommended age for CRC screening. This demographic skew suggests that the reported knowledge scores primarily reflect awareness among younger adults, rather than those approaching the screening or high-risk age group (≥45 years). As a result, the findings may underestimate or misrepresent CRC knowledge levels among older adults, who constitute the primary target population for screening programs. Future studies should employ longitudinal or probability-based designs with adequate representation of older adults (≥45 years) to overcome the age skew and sampling bias. Additionally, objective verification of screening and diagnosis through medical records is recommended to minimize self-report bias and improve data validity. As this study employed a cross-sectional design, causal inferences and predictive associations could not be established. Therefore, the statistical findings presented in tables need to be interpreted as descriptive and associative rather than predictive. Longitudinal or prospective studies are needed to confirm these associations and evaluate predictive factors more robustly. The study highlights the urgent need for culturally tailored public health campaigns, national screening programs, and integration of CRC awareness into primary care.
Based on these findings, targeted public health strategies should focus on enhancing CRC awareness and screening participation across Saudi Arabia. Nationwide education campaigns, integration of screening into primary healthcare visits, and digital outreach initiatives can help reach younger populations and reduce access barriers. Establishing national registries and subsidizing screening services may further strengthen early CRC detection efforts and support the goals of Saudi Vision 2030.
Conclusion
This study identified potential gaps in CRC awareness and screening among adults in Saudi Arabia, with lower knowledge particularly observed among women and lower-income groups. Based on these findings, public health efforts may focus on targeted education campaigns to improve awareness, promote preventive behaviors, and standardize screening practices. Healthcare providers might consider routinely discussing CRC risk with patients, while policymakers could prioritize national screening programs and ensure equitable access to healthcare. Implementing these measures can help enhance early detection and improve overall CRC outcomes in the population.
Footnotes
Consent to Participate
Participants provided digital informed consent.
Author Contributions
O.A.I., M.A.J., and L.I.D. contributed to the study conception and design, drafting of the manuscript, and gave final approval, with all agreeing to be accountable for the work’s accuracy and integrity. O.A.I. and M.A.J. additionally participated in data acquisition, analysis, interpretation, and critical revision for intellectual content. R.A.A., R.M.A., and F.A.A. were involved in the study conception and design, data acquisition, manuscript drafting, and final approval. Y.B.A., O.A.M., and J.A.O. contributed to data acquisition, analysis, interpretation, drafting, and critical revision, and approved the final version. A.I.A., A.M.A., and M.J.A. participated in data acquisition, manuscript drafting, and final approval. W.S.B., J.A.H., and K.A. contributed to data acquisition, data analysis and interpretation, critical revision for intellectual content, and final approval of the manuscript. All authors have read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
Institutional Review Board Statement
This study was approved by Jazan University’s Scientific Research Ethics Committee (reference number REC-45/11/1127, dated 02/06/2024)