
Abstract
Introduction
Among opportunistically screened population with above normal-weight, screening-related information remains limited. This study aimed to evaluate the infection status and distribution of high-risk (hr) human papillomavirus (HPV) on precancerous grades and cancer among overweight women compared with normal-weight women, and further explored the association between clinical characteristics and both HPV infection and cervical lesions.
Methods
The reporting of this cross-sectional retrospective study conforms to STROBE guidelines. This study was conducted in the Affiliated Cancer Hospital of Xinjiang Medical University. A total of 720 out of 1146 women with complete medical records of demographic and clinical characteristics were enrolled on the colposcopy clinic. HrHPV infection status, cytology abnormality rates, detection rates of cervical intraepithelial neoplasia (CIN) grades and cancer, and clinical performance of triage tests were evaluated by Body Mass Index (BMI) levels, which were classified into two groups as overweight women (BMI ≥24 kg/m2) and normal-weight women (BMI <24 kg/m2).
Results
The hrHPV infection rate of overweight women (73.0%) was not significantly lower than that of normal-weight women (78.6%) by the GenoArray test (P = 0.09) and by HC2 test (68.5% vs 71.0%, P = 0.53). The positive rates of most frequent hrHPV subtypes of overweight women vs normal-weight women were HPV16 (31.1% vs 39.1%, P = 0.03). The detection rates of CIN lesions were lower among overweight vs normal-weight (28.3% vs 37.4%, P = 0.01), while the detections rate of cancer was slightly higher but not significant (7.2% vs 4.6%, P = 0.14). The clinical performance of different screening strategies were similar between overweight and normal weight women.
Conclusions
The HPV16 prevalence and the detection rate of cervical precancerous lesions was lower in overweight women than normal-weight women, indicating that targeted management strategies should be given to overweight women to decrease the underdiagnosis.
Introduction
Cervical cancer is the fourth most frequent cancer in women with an estimated 604 000 new cases and 340,000 deaths in 2020 worldwide.1,2 China is accountable for nearly 18% (∼106,000) of cervical cancer incidences and 14% (48,000) of deaths as a large population country. Such a severe burden of disease has aggravated global health inequalities. 3 Cervical carcinogenesis was multifactorial, involving not only persistent human papillomavirus (HPV) infection 4 but also key demographic and behavioral determinants such as age, 5 ethnicity, region, 6 marital status, 7 age of sexual debut, 8 education, 9 contraception, 5 gravidity, and parity. 10
The population with higher than normal Body Mass Index (BMI) has increased steadily worldwide. 11 More attention has been paid to obesity-related malignancies until now. Previous studies found that obesity contributed to the morbidity and mortality of cervical cancer.12-19 A Meta-analysis discovered that obese women were less likely to receive opportunistic screening than normal-weight owing to obesity-related complications, resulting in a lower detection rate of precancerous lesions but a higher incidence of cervical cancer.20-22 In another prospective and cross-sectional study, increasing BMI was associated with lower risks of Cervical Intraepithelial Neoplasia (CIN)2/3 but growing hazards of cancer in HPV-positive women.23,24 It was reasonable that overweight or even obesity was a risk factor of developing cervical cancer, because of decreasing detection rate of precancerous lesions. 25 However, previous studies have shown that screening-related information remains limited among opportunistically screened population with above normal-weight. We hypothesized that among overweight women identified through opportunistic screening, the HPV infection rate and CIN detection rate were lower than those relative in the normal-weight women.
Currently, according to the guidelines of the American Society for Colposcopy and Cervical Pathology (ASCCP) and the Chinese Society for Colposcopy and Cervical Pathology (CSCCP), the HPV and cytology testing remain the primary methods for cervical cancer screening in China. 26 A multicenter cross-sectional study of 40901 women demonstrated the following diagnostic performance metrics for detecting CIN grade 2 or worse (CIN2+) among patients referred for colposcopy in the United States: for high-risk(hr) HPV testing, the sensitivity was 88.2%, specificity 57.8%, positive predictive value (PPV) 10.9%, negative predictive value (NPV) 98.8%, positive likelihood ratio (LR+) 2.09, negative likelihood ratio (LR-) 0.20, and Youden’s index 0.460; for cytology at an atypical squamous cells of undetermined significance or worse (ASCUS+) threshold, the corresponding values were sensitivity 51.5%, specificity 73.4%, PPV 10.2%, NPV 96.3%, LR + 1.94, LR- 0.66, and Youden’s index 0.249. 27 Similarly, a cross-sectional study conducted in Shaanxi Province, China, found that among 1916 primary screening hrHPV positive patients referred for colposcopy, the sensitivity, specificity, PPV, NPV, area under the receiver operating characteristic curve (AUC), and Youden’s index of HPV 16/18 genotyping for detecting CIN2+ were 82.7%, 47.9%, 30.2%, 91.0%, 0.653, and 0.306, respectively. 28 However, on the hospital-based opportunistic cervical cancer screening among overweight women, the infection rates and distribution of hrHPV on precancerous grades and cancer, and clinical performance of different triage tests have not previously been reported.
This study evaluated the prevalence and distribution of hrHPV and the efficiency of opportunistic cervical cancer screening by using various screening methods based on BMI classification among women referred for colposcopy, and further explored the association between clinical characteristics and both HPV infection and cervical lesions. The aim of study was to promote the early prevention, detection and management of cervical cancer for overweight and obese groups.
Materials and Methods
Study Outpatients
A cross-sectional retrospective study was conducted at the Affiliated Cancer Hospital of Xinjiang Medical University in Northwestern China. Patients with abnormal cytology, positive HPV, and self-reported reproductive tract symptoms who were recommended for further colposcopy examination (EDAN, China) by the gynecologists during September 2021 to January 2022 were consecutively included in this study. Patients having radiotherapy or chemotherapy, incomplete baseline information, and undefined diagnoses were excluded (Figure 1). The senior colposcopist diagnosed and performed cervical biopsies if necessary. Digital medical records were collected from the hospital registration system (HIS system), including HPV and cytology, the transformation zone, colposcopic diagnosis of the unbiopsied, biopsy types, and histopathological diagnosis. Flowchart. Abbreviation: BMI, Body Mass Index; CIN, Cervical Intraepithelial Neoplasia
Meanwhile, demographic and clinical data were obtained from hospital records, including age, height, weight, reproductive history, sex-related history, and detection results. Approval was received from the Ethics Committee of the Affiliated Cancer Hospital of Xinjiang Medical University (approval number: K-2021055). Informed consent was dispensable, as all patient details were recorded anonymously and de-identified. The reporting of this cross-sectional study conforms to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 29
Study Procedure
Each patient referred for colposcopy underwent gynecological examination. The colposcopist exposed the cervix with a speculum, wiped the mucus off the cervical surface with a cotton swab, and slowly rotated the cervical brush 6-7 times in one direction to collect cervical samples: cytology samples were first collected with a sample collection brush and placed in specimen preservation solution (SurePath, BD Oncolarity, US); then HPV samples were collected using the Hybrid Capture 2 collection device (HC2, Qiagen, Hilden, Germany)/the diagnostic kit (HBGA-21PKG, Hybribio, China) and placed in their own commercial specimen transport medium. The above cervical samples were collected followed by disease requirements and voluntary principles. Laboratory tests are detailed below, and each test was performed completely blinded to other screening results.
HC2 Test
The HC2 test was a nucleic acid hybridization assay for semiquantitative detection of 13 hrHPV subtypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) in bulk using microplate chemiluminescence for signal amplification. If the relative light unit/cutoff ratio (RLU/CO) were ≥1.0, samples were considered as HC2-positive. 30 According to a standard protocol, the HC2 test was performed at the laboratory department of the Affiliated Cancer Hospital of Xinjiang Medical University.
GenoArray Diagnostic Kit
The GenoArray Diagnostic Kit was an HPV DNA subtypes assay using the TePCR-reverse dot blot hybridization assay. 31 21 HPV subtypes were identified including 14 hrHPV subtypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68), 1 intermediate-risk HPV53, and 6 low-risk HPV subtypes (6, 11, 42, 43, 44 and 81). 32 According to a standard protocol, the HPV subtypes assay was also performed at the laboratory department of the Affiliated Cancer Hospital of Xinjiang Medical University.
Cytology
The liquid-based cytology (LBC) slides were prepared using Papanicolaou staining from cytological specimens in the sample preservation solution and interpreted according to the Bethesda 2001 classification system. 33 Cytological findings were classified as follows: negative intraepithelial lesion or malignancy (NILM), atypical squamous cells of undetermined significance (ASCUS), low-grade squamous intraepithelial lesion (LSIL), and atypical squamous epithelial cells not excluding high-grade squamous intraepithelial lesion (ASC-H), which included atypical adenosine cells (AGC), high-grade squamous intraepithelial lesion or worse (HSIL), which included squamous cell carcinoma (SCC) and adenocarcinoma in situ (AIS). The cytologists from the pathology department of the Affiliated Cancer Hospital of Xinjiang Medical University interpreted all slides and were blinded to other screening results.
Colposcopy and Histopathology
The colposcopist smeared the cervix with 5% acetic acid. (1) If white acid epithelium was observed after acetic acid application, the cervical biopsy was performed for each suspicious lesion area; (2) If the colposcopy impression was normal but abnormal HPV and/or cytological findings, discomfort, self-described symptoms, and benign findings (such as polyps or condyloma acuminatum), biopsy or diagnostic resection was performed. Cervical canal biopsy was required if necessary. (3) Out of ethical considerations, if the colposcopy impression was normal and laboratory findings showed ASCUS or less by cytology and negative HPV 16/18, biopsy was avoided. Cervical biopsies were performed by the senior colposcopist with over 20 years of colposcopy working experience.
The two pathologists performed histological diagnosis on hematoxylin and eosin (H&E)-stained slides at the pathology department of the Affiliated Cancer Hospital of Xinjiang Medical University. Immunohistochemical staining for p16 and Ki67 was performed on tissue samples against ambiguous diagnosis, respectively. Histopathological findings were classified as benign, CIN1, CIN2, CIN3, and cancer according to the World Health Organization (WHO)-approved criteria. Conjoint H&E and p16/Ki67 stained slides determined the ultimate diagnosis indicated by the worst results.
Statistical Analysis
Demographic and clinical characteristics were analyzed using descriptive statistics. Continuous variables are described using means and standard deviation, as well as categorical variables using frequencies and percentages. According to Chinese standards, BMI was classified into four groups: underweight (<18.5 kg/m2), normal (18.5-23.9 kg/m2), overweight (24-27.9 kg/m2), and obesity (≥28 kg/m2).34,35 Given the very few numbers of underweight women (4.4%) in our study, we combined underweight and normal BMI group together, named normal-weight women; and we combined overweight with obesity in one group named overweight women. 15 HPV subtypes were considered as hrHPV, which consists of 14 known hrHPV subtypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and 1 intermediate-risk HPV53. HPV viral-load was described as continuous variables using RLU/CO. The agreement was evaluated by Cohen’s kappa values between the HC2 test and HPV subtypes assay. Considering the very few numbers of finding ASC-H plus AGC (3.4%) in cytological grades, we combined ASC-H/AGC and HSIL as cytology high-grade group. According to BMI classification, sensitivity, positive predictive value (PPV), were calculated for different triage approaches with respective 95% confidence intervals (CIs) for detecting CIN2+. The triage efficiency was evaluated by the number needed to refer to colposcopy to find one case of CIN2+ (NNR). The significant differences between the groups were evaluated by the Pearson χ2 test. The associated factors with dependent variable (hrHPV infections, cervical lesions and BMI) were analyzed through binary and multinomial logistic regression analysis, expressed as odds ratios (ORs) and 95%CIs.
Data were statistically analyzed using Graphpad Prism 9.3.1, Excel 2019, MedCalc Statistical Version 20 (MedCalc Software Ltd., Ostend, Belgium) and SPSS version 28 (IBM, New York, USA). P < 0.05 (2-sided) was considered statistically significant.
Results
Among 1146 women referred for colposcopy, 426 women were excluded based on the aforementioned exclusion criteria. Finally, a total of 720 women aged 21-73 years, with a median age of 45 years (interquartile range [IQR] 37-52 years) were analyzed (Figure 1). As Table 2 summarized, 76.1% (528/694) women were hrHPV positive by HPV GenoArray Diagnostic Kit, while 69.9% (373/534) women were hrHPV positive by HC2 test. The agreement between the HC2 assay and the HPV subtype test showed fairly well with kappa values as 0.66 in normal-weight women and 0.68 in overweight women (Supplement Figure 1). 79.3% women received cervical biopsies, of which 239 were diagnosed as precancerous lesions (CIN1-3) and 42 as cancer.
Clinical Characteristics of Overweight Women Referred for Colposcopy
Characteristics of Women Referral for Colposcopy Based on BMI Classification

aKazak, Mongolian, Hui, Kirgiz.
bWidowed, Separated, Divorced, and not informed.
cNulliparous and not informed.
Abbreviation: BMI, Body Mass Index. P < 0.05; significant p values are bolded.
Screening Data of Women Referral for Colposcopy Based on BMI Classification
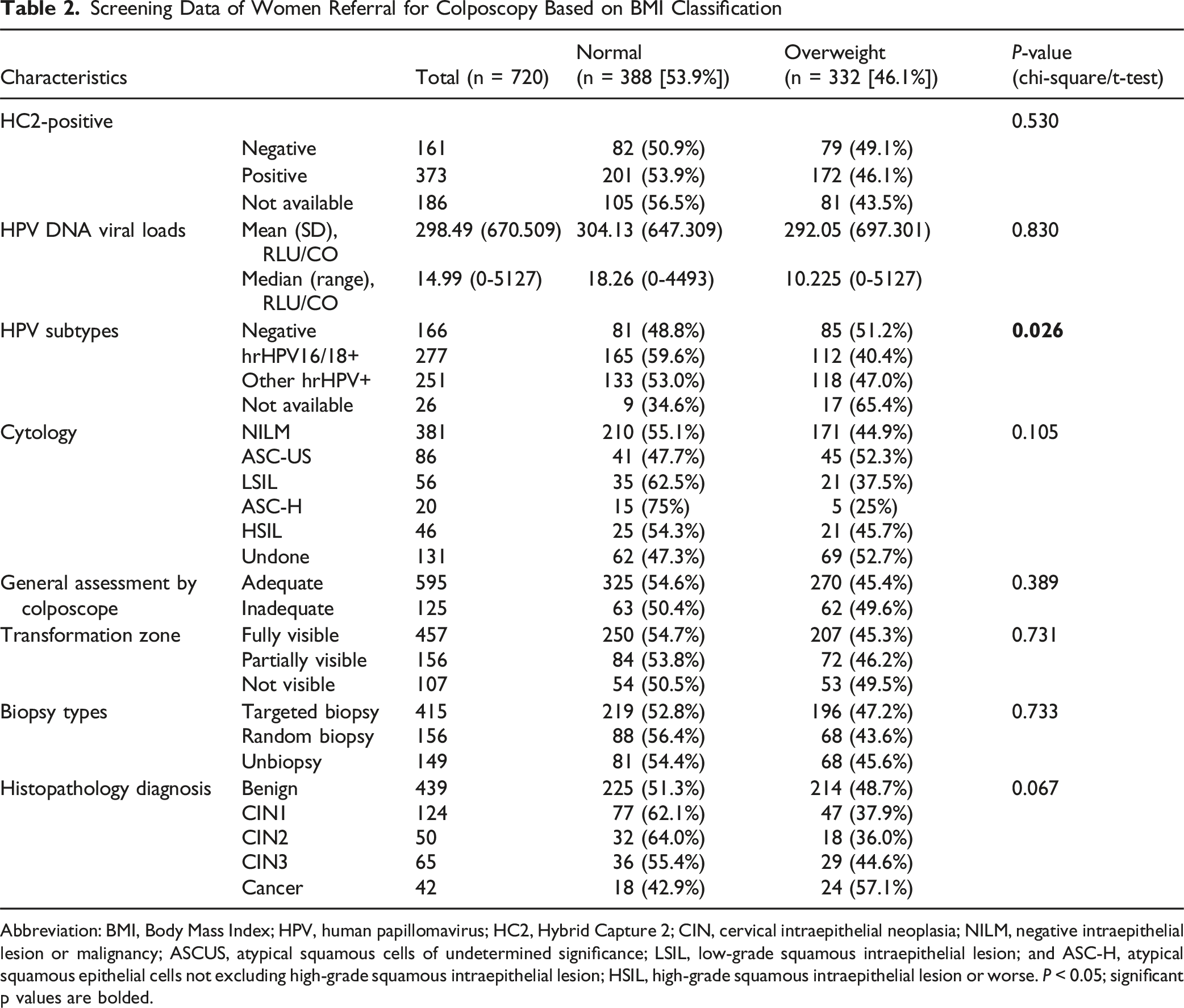
Abbreviation: BMI, Body Mass Index; HPV, human papillomavirus; HC2, Hybrid Capture 2; CIN, cervical intraepithelial neoplasia; NILM, negative intraepithelial lesion or malignancy; ASCUS, atypical squamous cells of undetermined significance; LSIL, low-grade squamous intraepithelial lesion; and ASC-H, atypical squamous epithelial cells not excluding high-grade squamous intraepithelial lesion; HSIL, high-grade squamous intraepithelial lesion or worse. P < 0.05; significant p values are bolded.
Distribution and Prevalence of hrHPV Subtypes according to BMI Classification
Among 694 women with genotyping information, the most prevalent five hrHPV subtypes were HPV16 (246, 35.4%), followed by HPV 52 (69, 9.9%), HPV 58 (53, 7.6%), HPV 53 (46, 6.6%), and HPV 18 (44, 6.3%). Among 528 women with hrHPV positive by GenoArray test, 351 women (66.5%) had single subtype infections, while 177 women (33.5%) had multiple subtype infections. Of 351 women with single hrHPV subtypes, the most prevalent subtypes were HPV16 (168, 47.8%), followed by HPV 52 (30, 8.5%). Of 177 women with multiple hrHPV subtype infections, 111 (62.7%) were infected by two HPV subtypes, 28 (15.8%) were triple infections, and HPV53 did not show coinfection with any other types. Moreover, the HPV16/18 co-infection were the most prevalent combination (63, 56.8%) in the double type infections group.
Considering BMI status, of 315 women with overweight, the most frequent subtypes was HPV16 (31.1%), which was significant lower than the HPV16 prevalence in 379 normal-weight women (39.1%, P = 0.03), followed by HPV52 (24, 7.6% vs 45, 11.9%, P = 0.06), HPV53 (22, 7.0% vs 24, 6.3%, P = 0.71), HPV58 (20, 6.3% vs 33, 8.7%, P = 0.24), and HPV18 (19, 6.0% vs 25, 6.6%, P = 0.75) in overweight women vs normal-weight women (Figure 2A). Additionally, single hrHPV prevalence of overweight women (48.0%) was higher than that of normal-weight women (52.0%, P = 0.29), as same results on multiple hrHPV prevalence (19.7% vs 22.7%, P = 0.34) (Figures 2B and C). The Distribution and Prevalence of hrHPV Subtypes According to BMI Classification. Note: The Distribution and Positive Rates Were About A) hrHPV Subtypes in Normal-Weight Women, Overweight Women, and all Women, B) Single hrHPV Subtypes in Normal-Weight Women and Overweight Women, and C) Multiple hrHPV Subtypes in Normal-Weight Women and Overweight Women. Abbreviation: BMI, Body Mass Index; hr, High-Risk; HPV, Human Papillomavirus
The Detection Rate of Each Histopathological Grade Classified by Genotype and BMI Status
A total of 528 women with hrHPV-positive were pathologically diagnosed after colposcopy examination. Of these, 246 women had histological abnormalities (46.6%), from mild to severe lesions: CIN1 (100, 18.9%), CIN2 (49, 9.3%), CIN3 (61, 11.6%), and cancer (36, 6.8%), respectively. Of 694 women with the Genoarray test, HPV16 was dominant for finding CIN1 (37, 5.3%), CIN2 (26, 3.7%), CIN3(45, 6.5%), and cancer (28, 4.0%) (Figure 3C). The Cumulative Detection Rates and Distribution of HPV Subtypes in Different Pathological Results According to BMI Classification. Note: The HPV Cumulative Detection Rates and Distribution are Shown in A) Normal-Weight Women, B) Overweight Women, and C) All Women. Abbreviation: BMI, Body Mass Index; HPV, Human Papillomavirus; CIN, Cervical Intraepithelial Neoplasia
Considering BMI classification, the detection rates of each precancerous stage was lower among 332 overweight women vs 388 normal-weight women (28.3% vs 37.4%, P = 0.01), from mild to severe lesions: CIN1 (14.2% vs 19.8%, P = 0.05), CIN2 (5.4% vs 8.2%, P = 0.14), and CIN3 (8.7% vs 9.3%, P = 0.78), respectively, although slightly higher for detecting cancer (7.2% vs 4.6%, P = 0.14). HPV16 was also the main types for finding histological abnormality in the overweight and normal-weight groups. Furthermore, there are some differences between HPV genotypes observed in cervical cancer cases between two groups. In overweight women with cervical cancer, HPV16/18/31/33/53/58/59 were detected, whereas HPV16/18/33/52/56 were observed among normal-weight women suffered from cervical cancer (Figures 3A and B).
Clinical Performance of Different Tests according to BMI Classification
Overall, two HPV tests were superior in sensitivity (>92%), while the cytology was superiority in PPV with the lowest number of colposcopy referrals to detect one CIN2 + case (NNR = 2.5). When combining two tests to triage women referred for colposcopy, HPV16/18+ with reflex cytology (ASC-US+) demonstrated decreased sensitivity (∼90%) with the increased PPV (∼33%). All indicators were similar between overweight and normal-weight women.
Diagnostic Performance of Triage Tests for CIN2 + Detection Based on BMI
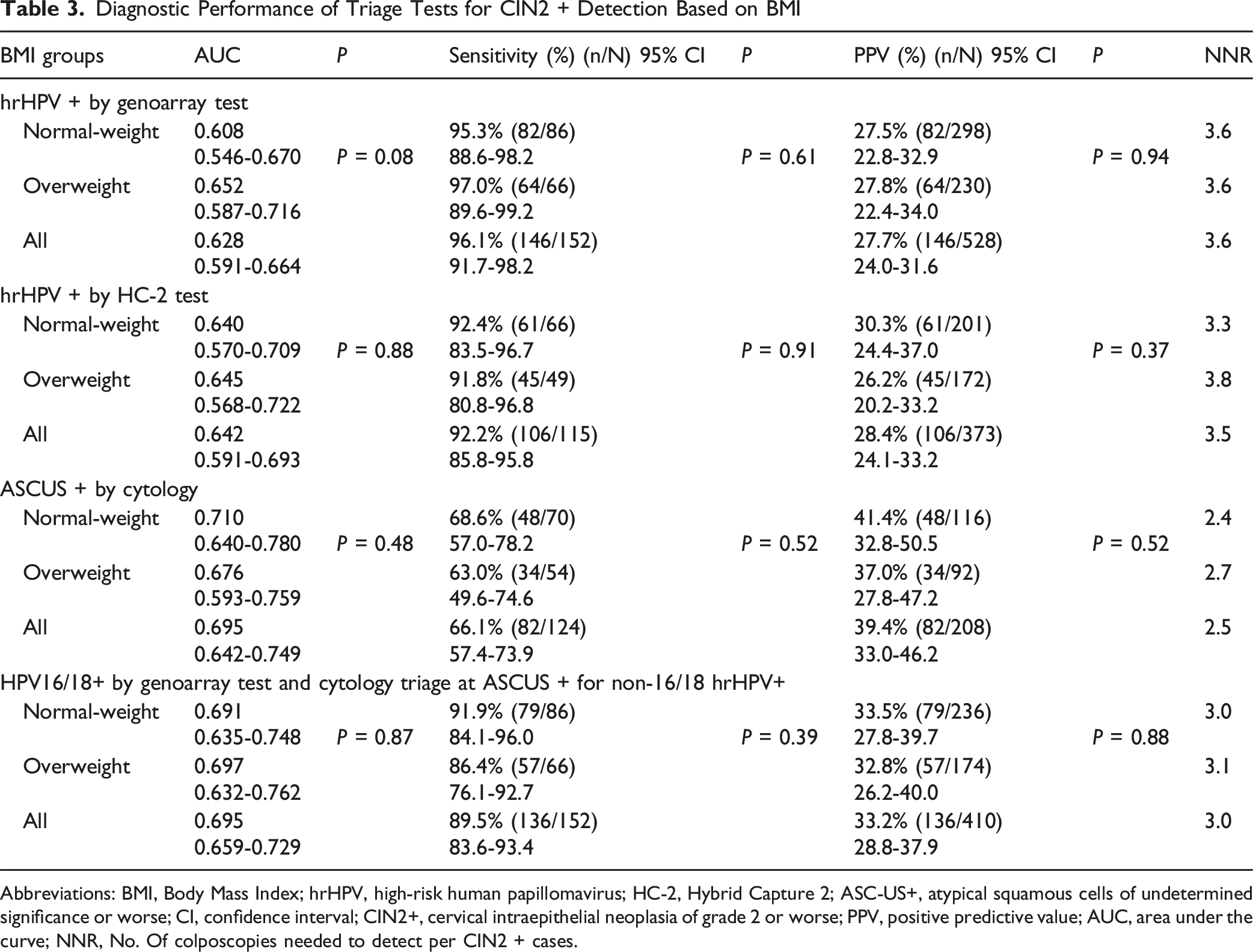
Abbreviations: BMI, Body Mass Index; hrHPV, high-risk human papillomavirus; HC-2, Hybrid Capture 2; ASC-US+, atypical squamous cells of undetermined significance or worse; CI, confidence interval; CIN2+, cervical intraepithelial neoplasia of grade 2 or worse; PPV, positive predictive value; AUC, area under the curve; NNR, No. Of colposcopies needed to detect per CIN2 + cases.
Associated Factors with BMI in Women Referred for Colposcopy
As summarized in Supplement Table 1, binary and multinomial logistic regression analyses were performed with adjustments for BMI, age, ethnic group, region, marital status, age at sexual debut, education, contraceptive, and gravidity. Using the Genoarray assay, the analysis revealed that women aged ≤45 years had a higher risk of HPV 16/18 infection, while premarital intercourse and married were associated with a lower risk of non-16/18 HPV infection. Similarly, when using the HC2 assay, married was also associated with a lower risk of hrHPV infection. Additionally, the results indicated that women in Southern or Northern Xinjiang were associated with an elevated risk of CIN2 and cervical cancer, while the non-contraceptive use may increase the risk of CIN3 and cervical cancer.
Association Factors With BMI by Age Stratified


Discussion
According to hospital-based samples of 720 women screened for cervical cancer, we analyzed the type-specific HPV prevalence and distribution for overweight women in the northwest of China. We herein found that overweight women had a lower prevalence of hrHPV than normal-weight women tested by the GenoArray test and HC2 test for precancerous lesions, although they had a higher prevalence for cancer. It was speculated that overweight women should be given attention and closely monitored to keep them from the occurrence of cervical cancer caused by a missed diagnosis in the precancerous stage.
The probability of detecting precancerous lesions may weaken for the majority of overweight and even obese women. While HPV16 remains the most common carcinogenic type, Multicenter hospital-based observational studies have reported an overall HPV16 prevalence of 39.96%, 36 whereas our study observed a moderately lower rate (35.4%). HPV testing demonstrated high sensitivity (96%), consistent with previous study.37,38 Although screening effectiveness was comparable between overweight and normal-weight groups, HPV16 positivity was significantly lower in the overweight group. This may be attributed to the substantially increased referral of hrHPV-positive women for colposcopy, coupled with the procedure’s limited diagnostic accuracy (ranging from 37% to 66%), which likely leads to higher detection of invasive cancers rather than precancerous lesions, especially among overweight and obese women.39-43
HPV53-infected women with overweight should receive clinical attention. Previous studies showed that non-vaccine-covered HPV53 prevalence was 1.5% in population-based screening in Huzhou, China. 44 Single HPV53 pathogenicity was low during the longest follow-up to 34 months. 45 However, of among overweight women in our study, HPV53 was associated with cancer, although the HPV53 infection rate was 7% and only presented as a single infection pattern.
To our knowledge, our research was the first to explore the association between BMI and opportunistic cervical cancer screening for women referred for colposcopy. Apart from age, region, climate, lifestyle behaviors, and demographic information, BMI was also associated with the prevalence of hrHPV subtypes and the development of cervical cancer.46-51 This research evaluated the epidemiology and frequency of hrHPV subtypes and the viral loads of hrHPV DNA in histological or cytological grades based on BMI categorization. The HPV16/18 infections were lower among overweight women vs normal-weight women. We also found that, in hospital-based opportunistic cervical cancer screening program, the cancer prevalence in overweight women was higher than that of normal-weight women, but the prevalence of precancerous lesions was lower. Discovery was similar to the previous prospective population-based study. 23 Our further analysis revealed that overweight women aged ≥45 years were less likely to have HPV16/18 infection, even though logistic regression showed no significant association between overweight and either hrHPV positivity or cervical lesions. Among overweight women without a reduction in cancer incidence, there may be a higher proportion of non-hrHPV-related cervical cancers that require effective screening strategies for detection.
Effective screening strategies should be brought up for overweight and obese women to identify cervical precancerous lesions and prevent them from the development of cervical cancer. These prompted further warnings for overweight and obese. First, overweight women should receive more clinical care. Overweight women paid less attention to opportunistic screening,20-22 resulting in a lower screening positive rate than normal-weight women, because of obesity-related diseases like cardiovascular and cerebrovascular diseases, 52 sleep-respiratory distress syndrome, 53 and endometrial cancer. 54 Second, weight stigma and discrimination may repress physical and mental health and seriously threaten the societal principles of equality, diversity, and inclusion. 55 It was urgent and necessary for us to take optimized action on health policy, such as self-sampling, 56 home-use testing, public education, and so on, to maximize the accessibility of opportunistic screening for overweight or obese women. Furthermore, exploring cervical cancer triage strategies that are more suitable for overweight and obesity will be the next crucial step. Continuing to develop clinical screening techniques were suitable for overweight and obese women, although current detection and sampling methods has been thoroughly checked. 57 Existing screening methods may result in underdiagnosis of precancerous lesions and increasing the odds of cervical cancer, due to insufficient detection on overweight women. Finally, we proposed that the precancer identified correctly was crucial for the subsequent management of overweight and obesity. We need to evaluate whether existing equipment (e.g., speculum size) and procedures enabled visualization and sampling of the cervix in overweight and obese patients. The lack of appropriately sized equipment or vaginal dilation tools for retraction of the lateral vaginal wall made cervical visualization with possibly more challenging in clinical colposcopy practice for overweight and obesity.
There were some limitations in this research. First, this study was an observational study. Our results can’t infer causation and might be affected by unmeasured confounders. Further investigation in prospective studies is still needed. Next, a priori sample size calculation was unperformed. However, based on our results, we found that the study nevertheless meets the minimum statistical power requirement for conventional research, which was 0.806. Conducting rigorous studies with sufficient statistical power remains an integral component of our future work. Furthermore, this study may have selection bias, due to women referred by gynecologists. Given that the current study is one of the very few studies evaluating the association between BMI and hrHPV as well as cervical lesions, which might focus gynecologists on overweight women, the promising findings provide the necessary evidence for future population-based, multicenter studies to further evaluate the screening populations without clinically significant symptoms or signs. Additionally, this study may have information bias, since 18.2% of patients did not perform cytology, 25.8% did not get the HC2 test, and 3.6% did not undergo the HPV subtypes assay. However, the observational study was of a natural status, meaning there were no interventions and better matched the real world. Finally, we did not get data on additional obesity-related disorders and the total number of sex-partners throughout life, although reasonably healthy women had a noticeably higher likelihood of opportunistic screening.
Conclusions
In conclusion, the HPV16 prevalence and the detection rate of cervical precancerous lesions of overweight women were lower than that of normal-weight women, although higher for cancer.
These implied that higher BMI might be associated with the underdiagnosis of precancer lesions, which might lead to the development of cervical cancer. Despite the immense potential of the HPV vaccine, the screening will continue to be the cornerstone of cervical cancer prevention for future many years. 48 Given that obesity is a global problem, this study may have important implications for the secondary prevention of cervical cancer for overweight and obesity.
Supplemental Material
Supplemental Material - The Infection Status and Distribution of hrHPV in Cervical Lesions Among Overweight Women Referred for Colposcopy: A Cross-Sectional Study
Supplemental Material for The Infection Status and Distribution of hrHPV in Cervical Lesions Among Overweight Women Referred for Colposcopy: A Cross-Sectional Study by Aiyuan Wu, Sumeng Wang, Dou Wang, Peng Xue, Guzhalinuer Abulizi, Remila Rezhake, Youlin Qiao in Cancer Control.
Footnotes
Acknowledgments
We acknowledge the great support of the staffs from colposcopy clinics and gynecologic department from the Affiliated Cancer Hospital of Xinjiang Medical University.
Ethical Considerations
The study was approved by the Research Ethics Committee of the Affiliated Tumor Hospital of Xinjiang Medical University (approval number: K-2021055) on February 17, 2021.
Consent to Participate
Informed consent was waived because the data were retrospectively extracted and entirely anonymized.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Xinjiang Uygur Autonomous Region Tianshan Talent Program—Young Top-Notch Talents in Science and Technology (2024TSYCCX0048), the Postdoctoral Fund of Affiliated Cancer Hospital of Xinjiang Medical University, the Soft Science Research Project of Wuxi Science and Technology Association (KX-25-B09), and the Postdoctoral Fund of the Affiliated Women’s Hospital of Jiangnan University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.