
Abstract
Introduction
Despite improved outcomes with PD-1 inhibitors (PD-1i) in advanced non–small cell lung cancer (NSCLC), the determinants of cancer-, cardiovascular disease (CVD)-, and other-cause mortality remain poorly characterized in older adults. This study applies competing-risks methods to estimate cause-specific mortality and to identify predictors for each cause in this population.
Methods
A retrospective cohort study was conducted using the 2014-2019 SEER-Medicare linked database, including patients aged 65 years or older with advanced NSCLC who received PD-1i (nivolumab or pembrolizumab). Mortality outcomes included deaths from CVD, NSCLC, other cancers, and other diseases. Predictors included treatment-related factors (e.g., PD-1i type), demographic factors (e.g., age, sex), socioeconomic status (e.g., Medicaid dual eligibility), cancer-related factors (e.g., NSCLC stage), and comorbidities (e.g., congestive heart failure [CHF]). Competing risk analyses were performed using the Fine-Gray model, with cause-specific Cox models for sensitivity analyses.
Results
Among 5076 patients, 68.36% received nivolumab and 31.64% received pembrolizumab. Of 3746 deaths, most were from NSCLC (85.34%), while 2.80% were from CVD. No significant difference in CVD mortality risk was observed between the two PD-1i (sub-distribution HR [sHR] = 1.08; 95% CI: 0.63-1.84), but NSCLC mortality was associated with a lower risk in the pembrolizumab group (sHR = 0.67; 95% CI: 0.60-0.74) compared to the nivolumab group. A history of CHF (sHR = 2.10; 95% CI: 1.37-3.21) and Medicaid dual eligibility (sHR = 2.70 vs private insurance; 95% CI: 1.28-5.56) were associated with increased CVD mortality. NSCLC mortality was higher in Stage IV/distant than in Stage IIIB/regional (sHR = 1.24; 95% CI: 1.13-1.35) and males (sHR = 1.11; 95% CI: 1.03-1.20).
Conclusions
These results highlight the potential value of integrated cardio-oncology models and strategies addressing socioeconomic inequities among older adults receiving PD-1i. However, conclusions should be tempered by the SEER–Medicare data structure, including lack of biomarker information and restricted applicability to younger or non-Medicare populations.
Plain language summary
Lung cancer remains the leading cause of cancer-related deaths in the U.S. Thanks to new treatments like immunotherapy, especially for a type called non-small cell lung cancer (NSCLC), more patients are living longer. Two commonly used immunotherapy drugs—nivolumab and pembrolizumab—have shown promising results. However, there are concerns about side effects, including risks to heart health. This is especially important for older adults, who often already have heart conditions. This study looked at nearly 5000 people aged 65 or older with advanced NSCLC who were treated with either nivolumab or pembrolizumab. Researchers used the national cancer registry and Medicare records to understand which causes of death were most common, such as NSCLC, heart disease, or other diseases, and which patient factors were linked to these outcomes. Most patients died from NSCLC, while a small number died from heart-related problems. The risk of heart-related death was similar between the two drugs. The study also found that patients who had a history of congestive heart failure or were enrolled in both Medicare and Medicaid (a national health insurance program for people with lower income) were more likely to die from heart disease. Lung cancer deaths were more common among men and those with more advanced stages of cancer. These findings suggest that when treating older adults with lung cancer, doctors should consider more than just the cancer. A patient’s heart health and financial situation may also affect treatment outcomes. This information can help guide more personalized treatment decisions and better support the needs of older adults receiving immunotherapy.
Keywords
Introduction
Lung cancer is the second most commonly diagnosed cancer and remains the leading cause of cancer-related deaths in the United States, accounting for approximately 20% of all cancer deaths. 1 More than 70% of lung cancer cases are diagnosed at advanced stages, classified as regional or distant, with a significant proportion occurring in individuals aged 65 years or older. The majority (approximately 84%) of lung cancer cases are non-small cell lung cancer (NSCLC), and the median age at diagnosis is 71 years.2,3
Over the past decade, immune checkpoint inhibitors (ICIs), particularly those targeting programmed death-1 (PD-1), have significantly improved clinical outcomes in advanced NSCLC. 4 Despite these advancements, ICIs are associated with immune-related adverse events (irAEs), 5 and recent studies have reported that immune-mediated cardiovascular toxicities, such as myocarditis, though rare, are increasingly recognized and can be life-threatening.6-9 Given the large number of patients eligible for ICI therapy, recent studies emphasized the need for improved recognition, definitive clinical evidence of ICI-associated cardiovascular toxicities.7-9
Age is the most significant risk factor for cardiovascular disease (CVD), 10 and older patients are more susceptible to cancer therapy-induced cardiotoxicity than younger counterparts. 11 In NSCLC, non-cancer-specific mortality is a major competing risk for NSCLC-specific mortality, and its contribution increases with age.12,13 Notably, deaths from non-NSCLC causes rise progressively with age, with CVD being the most prominent contributor. 13 However, prior studies focused on early-stage disease or did not account for ICI treatment. Furthermore, despite the increasing number of older patients with NSCLC, they remain underrepresented in clinical trials, including those evaluating ICIs,14,15 resulting in limited population-level data on mortality patterns and their factors in this population.
With the advent of PD-1 inhibitors and other novel therapies, survival in advanced NSCLC has improved; nonetheless, 5-year relative survival remains low. 16 As a result, the influence of comorbid conditions, both cancer-related and non–cancer-related, on outcomes has become increasingly salient. To individualize care and reduce preventable deaths, it is essential to delineate competing causes of death and their predictors. However, studies specifically characterizing cause-specific mortality among older adults with advanced NSCLC treated with PD-1 inhibitors remain limited. To address this critical knowledge gap, our study aims to examine the competing risks of cause-specific mortality in older patients with advanced NSCLC receiving PD-1 inhibitors. Specifically, we aim to identify factors influencing NSCLC-related and CVD-related mortality in this population.
Methods
Data Sources
The Surveillance, Epidemiology, and End Results (SEER)-Medicare linked database combines clinical, demographic, and cause-of-death information from cancer registries with claims data from the Medicare program.17,18 The SEER program, sponsored by the National Cancer Institute, collects cancer epidemiology data covering approximately 48% of the U.S. population. 19 Medicare is a federal health insurance program serving older adults, individuals with disabilities, and those with end-stage renal disease, and it is the primary health insurance provider for 97% of the U.S. population aged 65 and older. 17 The SEER-Medicare data do not include direct identifiers. 20 The Institutional Review Board of the University of Texas at Austin determined that this study was not classified as human subjects research and was secondary use of a de-identified data set.
Study Design
This retrospective cohort study was conducted using the SEER-Medicare linked database from 2014 to 2019. The index date was defined as the initial receipt of pembrolizumab or nivolumab (Figure 1). The receipt of pembrolizumab or nivolumab was identified using the Healthcare Common Procedure Coding System (HCPCS) and National Drug Codes (NDC) (Supplemental Table 1). We defined the pre-index period as the 12 months before the index date to capture the patient’s history of comorbidities. The post-index period was defined as the follow-up period from the index date to the date of death or the end of the study (December 31, 2019), whichever occurred first. The reporting of this study conforms to STROBE guidelines.
21
Study Design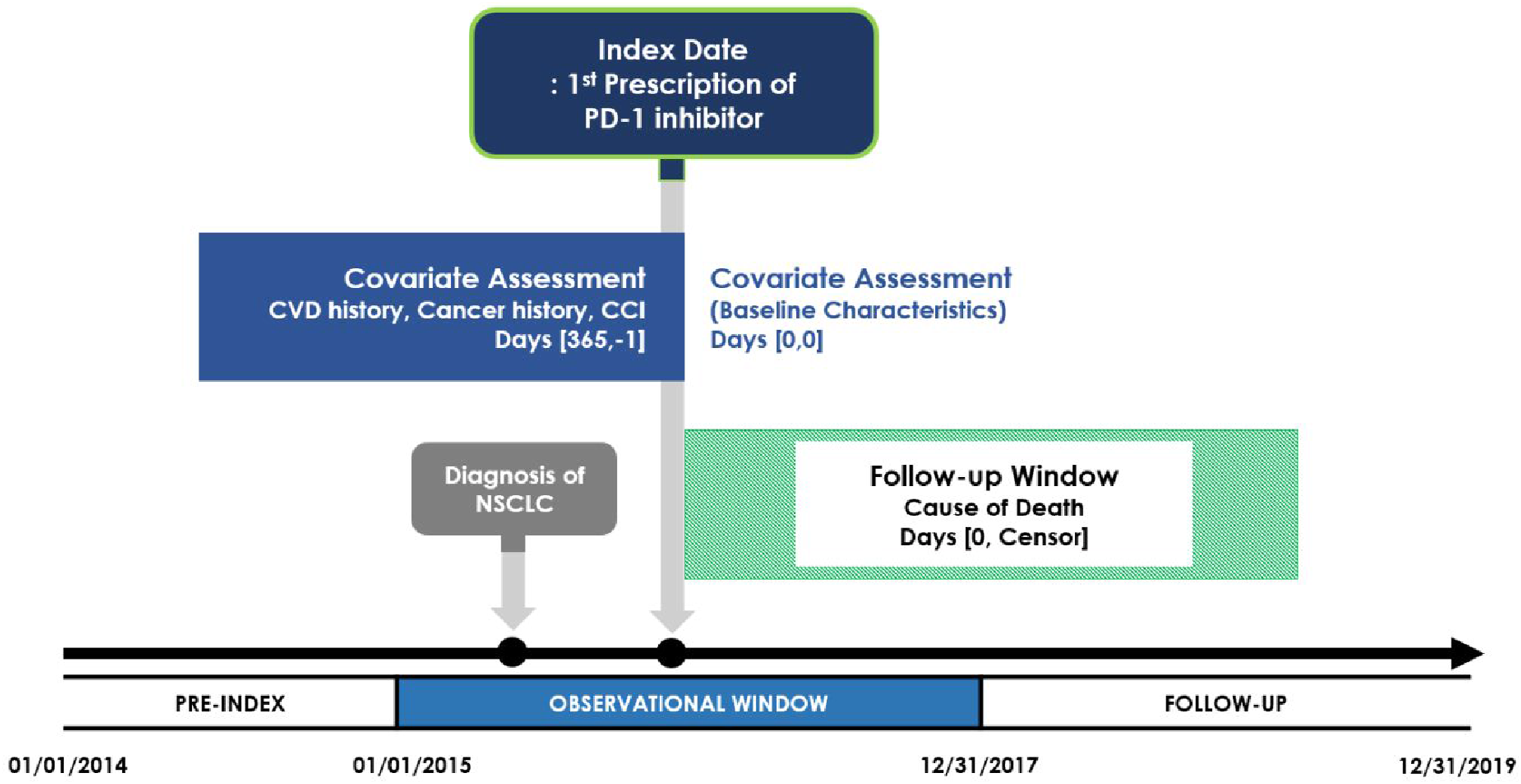
Study Population
We included patients diagnosed with advanced NSCLC at age 65 years or older who received pembrolizumab or nivolumab between January 1, 2015, and December 31, 2017. NSCLC was defined using the International Classification of Diseases, tenth revision, Clinical Modification (ICD-10-CM: C34.x), and histologic type (ICD-O-3). We defined advanced NSCLC as stages IIIB to IV by the American Joint Committee on Cancer (AJCC) or regional and distant stages by the SEER summary stage.
Patients were excluded if they met any of the following criteria: (1) Eligibility for Medicare due to end-stage renal disease or disability during the study period, (2) Lack of continuous eligibility for both Medicare Parts A and B, (3) Enrollment in a Medicare health maintenance organization (HMO), (4) Death within 4 weeks of the index date, or (5) A discrepancy of more than two months between the date of death reported in SEER and Medicare.
Outcomes
The primary outcomes of interest were overall survival and cause-specific mortality, classified into 4 groups: CVD, NSCLC, other cancers, and other diseases, based on the ICD-10-CM codes. CVD was defined as diseases of the heart, hypertension without heart disease, cerebrovascular diseases, atherosclerosis, aortic aneurysm, and other diseases of the arteries, arterioles, and capillaries, as identified using the ICD-10-CM codes. 22
Predictors
We included a range of variables, including demographics, tumor characteristics, treatment-related factors, and comorbid conditions, to assess their relationship with each cause of death. Information on patient age, gender, race, and socioeconomic factors such as income and geographic region was included. We also included the primary health insurance provider, marital status, stage of NSCLC at diagnosis, and detailed tumor characteristics, such as the primary site, laterality, and histology of NSCLC. Income was assessed at the area level using the median household income of the census tract in this study. Additionally, we included the Charlson Comorbidity Index (CCI) to evaluate the influence of pre-existing comorbidities, 23 during the 1 year before the index date. Obesity, smoking, and alcohol use disorder history were also identified. We defined systemic corticosteroid use as an oral corticosteroid prescription exceeding 10 mg of prednisone-equivalent daily dosage after the index date.24,25
Statistical Analysis
For the descriptive analysis of baseline characteristics, we used t-tests for continuous variables and Fisher’s exact test or chi-square test for categorical variables to compare characteristics between PD-1 inhibitor user groups. To estimate hazard ratios (HRs) for comparisons between two periods and the impact of each factor on death, we used the multivariate Cox proportional hazards regression model. Given that different cause-specific deaths were treated as competing risk events, the Fine-Gray model was used as the primary analysis to assess the relationship between predictors and mortality. Additionally, the cause-specific Cox model was employed as a sensitivity analysis to evaluate the robustness of the results. Statistical analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC, USA).
Results
We identified 5076 older patients with advanced NSCLC who met the study’s inclusion criteria. Among them, 68.36% (n = 3470) were treated with nivolumab, and 31.64% (n = 1606) were treated with pembrolizumab (Figure 2). More than 70% of the participants (n = 3746) died during the study period. Among all the patients, the majority died from NSCLC (85.34%), while 1.17% of deaths were attributed to ischemic heart diseases (0.93% of total deaths in the pembrolizumab group and 0.84% in the nivolumab group) and 1.63% of deaths were attributed to other CVDs (1.25% of total deaths in the pembrolizumab group and 1.18% in the nivolumab group). Patient Selection Flow
Characteristics of Older Adults With Advanced Non-small Cell Lung Cancer (NSCLC) by Type of Programmed Death-1 (PD-1) Inhibitors (N = 5076)

Abbreviations: SD = standard deviation, CCI = Charlson comorbidity index, COPD = chronic obstructive pulmonary disease.
aOthers include American Indian/Alaska native/Asian/Pacific islander.
bNon-married include divorced/separated/widowed/never married.
cIncome was assessed at the area level using the median household income of the census tract. Q1–Q2 indicates an income level ≤ $62,622, while Q3–Q4 indicates an income level > $62,622.
dOthers include TRICARE/Military/Veterans Affairs/Indian/Public Health Service/Insurance status unknown.
eOthers include origin unspecified/unknown/paired site.
fFisher exact test was used.
The results from the multivariable Fine-Gray model showed no significant difference in mortality due to CVD (sub-distribution hazard ratio [sHR] = 1.08; 95% CI: 0.63-1.84; P = 0.79), other cancers (sHR = 0.92; 95% CI: 0.66-1.28; P = 0.63), or other diseases (sHR = 0.71; 95% CI: 0.48-1.05; P = 0.09) between the two PD-1 inhibitors (Supplemental Figure 1). However, a difference in NSCLC-related mortality was observed, with the pembrolizumab group showing a lower risk (sHR = 0.67; 95% CI: 0.60-0.74; P < 0.01) compared to the nivolumab group.
Competing Risks of Mortality in Older Patients With Advanced Non-small Cell Lung Cancer (NSCLC) Treated With Programmed Death-1 (PD-1) Inhibitors: Results From Fine-Gray Model

Abbreviations: HR = hazard ratio; CVD = cardiovascular disease; NSCLC = non-small cell lung cancer.
CI = confidence interval; PD-1 inhibitor = programmed death-1 inhibitor; CHF = congestive heart failure.
MI = myocardial infarction; PVD = peripheral vascular disease; CBVD = cerebrovascular disease.
COPD = chronic obstructive pulmonary disease.
Notes. *: P < .05; **: P < .01; ***: P < .001.
aOthers include American Indian/Alaska native/Asian/Pacific islander.
bNon-married include divorced/separated/widowed/never married.
cIncome was assessed at the area level using the median household income of the census tract.
dOthers include TRICARE/Military/Veterans Affairs/Indian/Public Health Service/Insurance status unknown.
A history of CHF was associated with increased mortality from all causes except NSCLC, including a two-fold higher risk of CVD mortality (sHR = 2.10; 95% CI: 1.37-3.21; P < 0.01) and mortality due to other diseases (sHR = 1.97; 95% CI: 1.40-2.78; P < 0.01). Older age was a significant predictor of NSCLC mortality. Patients over 80 years old had a 17% higher risk of NSCLC mortality (sHR = 1.17 compared to 65-69 years group; 95% CI: 1.04-1.32; P = 0.01).
Other treatment-related factors were associated with mortality. A history of lung cancer surgery was associated with higher mortality from other cancers (sHR = 1.70; 95% CI: 1.15-2.51; P = 0.01). A history of radiation was associated with higher mortality from other cancers (sHR = 1.53; 95% CI: 1.17-2.01; P < 0.01) or other diseases (sHR = 1.43; 95% CI: 1.04-1.98; P = 0.03).
Competing Risks of Mortality in Older Patients With Advanced Non-small Cell Lung Cancer (NSCLC) Treated With Programmed Death-1 (PD-1) Inhibitors: Results From Cause-specific Cox Model

Abbreviations: HR = hazard ratio; CVD = cardiovascular disease; NSCLC = non-small cell lung cancer.
CI = confidence interval; PD-1 inhibitor = programmed death-1 inhibitor; CHF = congestive heart failure.
MI = myocardial infarction; PVD = peripheral vascular disease; CBVD = cerebrovascular disease.
COPD = chronic obstructive pulmonary disease.
Notes. *P < .05; **P < .01; ***P < .001.
aOthers include American Indian/Alaska native/Asian/Pacific islander.
bNon-married include divorced/separated/widowed/never married.
cIncome was assessed at the area level using the median household income of the census tract.
dOthers include TRICARE/Military/Veterans Affairs/Indian/Public Health Service/Insurance status unknown.
Discussion
This retrospective study examined the competing risks of 4 causes of death among older adults with advanced NSCLC receiving nivolumab or pembrolizumab and identified factors influencing mortality. As expected in a population with late-stage NSCLC, the leading cause of death was NSCLC, which aligns with the previous study showing the risk of death from lung cancer increases with stage. 13
We found no significant differences between the two PD-1 inhibitors in mortality related to CVD, other cancers, or other diseases after controlling for covariates. By contrast, pembrolizumab was associated with significantly lower NSCLC-related mortality compared to nivolumab. Although the pembrolizumab group had a higher proportion of stage IV disease, the nivolumab group had a higher prevalence of other adverse prognostic factors, including race/ethnicity, lower income, squamous histology, and several comorbidities.26,27 These variables were included in the survival model, yet the nivolumab group still showed a higher hazard of NSCLC-related death, suggesting potential selection bias or residual confounding beyond measured covariates. Prior randomized trials reported no meaningful differences in efficacy or safety between nivolumab and pembrolizumab in advanced NSCLC,28,29 and real-world studies also found no significant difference in progression-free survival after adjusting for covariates including programmed death-ligand 1 (PD-L1) expression.30,31 During the study period, pembrolizumab use was enriched for PD-L1–positive tumors by FDA label requirements, 32 whereas nivolumab could be prescribed regardless of PD-L1 status. 33 Accordingly, unmeasured differences in PD-L1 expression between treatment groups, which was not available in SEER-Medicare, could bias comparative estimates of NSCLC-specific mortality. Histology was also significant factor of NSCLC-related mortality, with adenocarcinoma and large cell carcinoma demonstrating a lower mortality risk compared to squamous cell carcinoma. These findings are consistent with previous research, which reporting that adenocarcinoma patients had significantly better 5-year overall survival rates than those with squamous cell carcinoma. 34
We found that certain patient demographics were associated with specific causes of death. As age is a well-established risk factor for mortality,12,13 our findings confirmed that older age was associated with higher NSCLC mortality. In the primary analysis using the Fine-Gray model, age showed a non-significant trend toward higher CVD mortality; however, the sensitivity analysis demonstrated a significantly higher hazard for CVD mortality among older patients. This association was particularly pronounced in patients aged 80 years or older compared to the younger group, emphasizing the need for tailored geriatric care in oncology. Sex-based differences in outcomes were also notable, with male patients exhibiting higher NSCLC mortality. This aligns with prior research indicating that female sex is a consistent predictor of better survival outcomes, independent of histology, stage, or treatment.35-37 These results highlight the importance of understanding sex-based differences in response to cancer therapies. In contrast to previous reports,14,27 neither Hispanic nor Black race/ethnicity was not significantly associated with mortality from any cause in our study. This may be attributable to the predominance of White patients (over 80%), and limited statistical power for subgroup comparisons.
Furthermore, clinical factors were associated with mortality. Pre-existing congestive heart failure (CHF) was associated with a significantly increased risk of not only CVD mortality but also mortality due to NSCLC and other diseases. CHF is one of the most common comorbid conditions in NSCLC patients and is associated with a significantly increased mortality risk.38-40 A German study also reported that the prevalence of CHF increases with age. 39 The elevated mortality risk may be due to the lower likelihood of NSCLC patients with CHF receiving surgery or chemotherapy compared to those without. 40 These findings underscore the importance of integrating routine cardiovascular screening and management strategies into the care of older NSCLC patients receiving ICIs to address overlapping risks.
Treatment-related adverse events, particularly systemic steroid use can affect survival. In our primary analysis, systemic corticosteroid use was not associated with mortality from any cause, whereas the sensitivity analysis suggested a protective effect on NSCLC- and other cancer-related mortality. Corticosteroids are often used at higher doses for cancer-related symptoms 41 ; however, their role during ICI treatment remains debated. Some studies reported the systemic corticosteroid use was related to poor outcomes in patients with NSCLC,42,43 while others reported detrimental effects only when used for cancer-related palliative indications, with no association for non cancer-related use. 44
Socioeconomic factors were also related to mortality. Medicare-Medicaid dual beneficiaries had an increased risk of CVD mortality after adjusting for covariates. This population is more likely to have low income and a high disease burden,45,46 and socioeconomic factors can influence access to care, treatment adherence, and outcomes.26,27,45,47,48 Survival disparities associated with Medicaid status are well-documented, although prior studies often did not specify cause of death or treatment type.49-51 Insurance-related disparities in CVD mortality among cancer survivors have also been reported. A recent study using SEER data found that lung cancer patients without insurance or on Medicaid had significantly higher CVD mortality than those with non-Medicaid insurance. 38 Lower PD-L1 testing rate and among NSCLC patients on Medicaid compared to those with commercial insurance may further contribute to these disparities. 51 Our findings confirm persistent insurance-related survival disparities in NSCLC patients, particularly in CVD mortality, highlighting the need for integrated cancer and CVD management in this vulnerable population.
This study has several limitations. First, the SEER-Medicare linked database does not include laboratory biomarkers, including PD-L1 expression levels, which may contribute to residual confounding. 52 Furthermore, although SEER-Medicare data contain variables related to behavioral factors such as smoking, alcohol consumption, and obesity, these variables have low sensitivity and may be underreported. 53 Additionally, a recent study suggests that the “Primary Payer at Diagnosis” variable in the SEER dataset may be unreliable. 54 Since all patients in our study were expected to be insured through Medicare by definition, this variable may have limitations in reflecting differences in insurance coverage. Second, the study period may limit the generalizability of our findings to the current population. We identified patients who received PD-1 inhibitors between 2015 and 2017. Around 2017, ICI-induced myocarditis became more widely recognized and systematically managed. Since then, significant advancements have been made in understanding, diagnosing, and managing cardiotoxic AEs, including myocarditis. Consequently, our findings may not fully reflect the current clinical practice in cardio-oncology. Third, our study did not include data on treatment line or duration, which may limit the interpretation of efficacy and toxicity outcomes. Both PD-1 inhibitors received initial FDA approval in 2015 for metastatic NSCLC in the second- or later-line setting,32,33 and contemporaneous clinical guidelines likewise recommended them for second-line treatment.55,56 Given the study’s identification window (2015-2017), it can be assumed that most patients received PD-1 inhibitors in the second-line or later setting. Fourth, while newer ICIs, such as PD-L1 and cytotoxic T-lymphocyte–associated protein 4 (CTLA-4) inhibitors, have recently been approved, their limited use in this cohort precluded meaningful analysis. As a result, our study focused exclusively on two PD-1 inhibitors. Future research using more recent data could provide a broader understanding of ICIs and their impact on mortality and causes of death in patients with NSCLC. Lastly, the study population consists exclusively of Medicare beneficiaries aged 65 years or older, limiting the generalizability of the findings to younger or non-Medicare populations.
Despite these limitations, our study has several notable strengths. First, to our knowledge, this is the first study to investigate overall survival and four types of cause-specific mortality among patients receiving PD-1 inhibitors in a real-world, population level in the U.S. Second, by categorizing mortality into four specific causes, including CVD, we provide valuable insights into the importance of managing comorbidities and risk factors in older adults with advanced NSCLC. Lastly, our use of both Fine-Gray and cause-specific Cox models ensures robust handling of competing risk events, consistent with best practices in competing risk analysis. 57
Conclusions
While PD-1 inhibitors have demonstrated significant survival benefits in patients with advanced NSCLC, their immune-related cardiotoxic effects are an increasing concern. However, their impact on cause-specific mortality, including CVD mortality remains poorly understood. We found no significant differences in CVD mortality between the two PD-1 inhibitors, though pembrolizumab was associated with lower NSCLC mortality. A history of CHF and Medicaid dual eligibility were significant risk factors for CVD mortality, highlighting the need for effective management of cardiovascular comorbidities in patients with advanced NSCLC, particularly in vulnerable populations. Additionally, older age was identified as a strong predictor of significantly higher CVD and NSCLC mortality, emphasizing the critical importance of integrating geriatric cardio-oncology into patient care. However, conclusions should be tempered by the SEER–Medicare data structure, including lack of biomarker information and restricted applicability to younger or non-Medicare populations.
Supplemental Material
Supplemental material - Factors Associated With Cause-specific Mortality in Older Patients With Advanced NSCLC Treated With PD-1 Inhibitors: A Retrospective Study
Supplemental material for Factors Associated With Cause-specific Mortality in Older Patients With Advanced NSCLC Treated With PD-1 Inhibitors: A Retrospective Study by Yeijin Kim, PharmD MS, Yan Liu, MD, PhD, Hae Sun Suh, MA, PhD, Chanhyun Park, MEd, PhD in Cancer Control
Footnotes
Acknowledgments
This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the National Cancer Institute; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database. In addition, the collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the authors and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors.
Ethical Considerations
The Institutional Review Board (IRB) of the University of Texas at Austin (IRB ID: STUDY00002383) determined that this study does not constitute human subjects research. Therefore, informed patient consent was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by two grants from Ministry of Food and Drug Safety: 21153MFDS601 and RS-2024-00331719 (2024).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.