
Abstract
Background
Pancreatic cancer is one of the most aggressive malignant tumors worldwide, often resulting in poor prognosis. Smoking is widely recognized as a significant risk factor for this disease.
Methods
This study extracted data on the disease burden of pancreatic cancer attributable to smoking in China from the Global Burden of Disease 2021 (GBD 2021) database. A total of 447 334 individuals were included in the analysis. A joinpoint regression model was used to calculate the annual percentage change (APC) and average annual percentage change (AAPC) to assess trends in the disease burden from 1990 to 2021. The age-period-cohort model was applied to explain the epidemiological trends of the disease by controlling for variables associated with age, period, and birth cohort. Decomposition analysis was conducted to quantify the relative contributions of population growth, population aging, and epidemiological changes. The Autoregressive Integrated Moving Average (ARIMA) model was utilized to forecast the burden of pancreatic cancer due to smoking in China over the next 15 years.
Results
From 1990 to 2021, the age-standardized mortality rate (ASMR) and the age-standardized disability-adjusted life years rate (ASDR) due to smoking-related pancreatic cancer in China exhibited an upward trend. By 2021, the total number of deaths and disability-adjusted life years (DALYs) had almost doubled compared to 1990. The mortality and DALY rates increased with age, peaking at approximately 85 years and 70 years, respectively, indicating a substantial burden on the elderly population. Furthermore, we predict that female ASMR and ASDR may start to decline in the next 15 years; however, the absolute burden remains unchanged. Conversely, the ASMR and ASDR for males continue to rise, indicating an increasing burden, with the male burden consistently surpassing that of females.
Conclusions
This study demonstrates that from 1990 to 2021, the burden of pancreatic cancer attributable to smoking in China has intensified, with significant disparities related to sex and age. The future outlook appears quite severe, given the large population base and accelerating population aging. Strong smoking cessation and control measures specifically targeting elderly males are imperative to limit tobacco exposure among high-risk groups, as these measures are crucial for alleviating the burden of pancreatic cancer in China.
Keywords
Introduction
Pancreatic cancer is a highly lethal malignancy with a poor prognosis, characterized by a 5-year relative survival rate of approximately 10%. 1 Most individuals are diagnosed at advanced stages, with about 80%-85% of patients losing the chance for surgical intervention due to tumor metastasis and other factors.2,3 According to the Global Cancer Observatory (GLOBOCAN) 2022, pancreatic cancer has become the sixth leading cause of cancer-related mortality worldwide and shows an increasing trend. 4 In recent years, there has been a gradual increase in the disease burden of pancreatic cancer in China. As estimated by the Global Burden of Disease (GBD) 2021 database, pancreatic cancer ranks fifth among malignancies in men and sixth in women. Consequently, pancreatic cancer not only exacerbates both social and personal economic burdens but also poses a significant public health challenge that impedes the development of modern healthcare systems.
Despite achieving certain breakthroughs in cancer prevention and treatment, managing pancreatic cancer remains particularly daunting in China. 5 Due to the unclear etiology of pancreatic cancer, analyzing modifiable risk factors can facilitate relevant authorities in implementing appropriate early prevention and treatment strategies. Smoking is recognized as a modifiable risk factor for various cancers, such as lung cancer 6 and colorectal cancer. 7 The GBD 2021 database identifies smoking as the primary attributable risk factor for pancreatic cancer, 8 defining smokers as individuals who have used any tobacco products daily or occasionally in the past or present. An international case-control study indicated that smokers have a threefold increased risk of developing pancreatic cancer compared to non-smokers, 9 and pancreatic cancer in smokers may involve more genetic mutations. 10 However, changes in other factors such as lifestyle, healthcare quality, and socioeconomic conditions can either exacerbate or mitigate the impact of smoking on mortality rates. These factors are crucial for a comprehensive assessment of disease burden. Assuming that smoking-related pancreatic cancer mortality and DALY rates in China increased from 1990 to 2021, with a more pronounced rise among males compared to females, the disease burden is expected to continue growing in the future. Strengthening tobacco control efforts will effectively slow the rate of increase in this burden.
In this study, it is crucial to account for the three key variables: age, period, and birth cohort. Aging 11 is associated with physiological changes and the cumulative effects of smoking, both of which contribute to the burden of pancreatic cancer. Over the past 30 years, transformations in dietary patterns, improvements in healthcare systems, and changes in tobacco policies have directly or indirectly influenced pancreatic cancer burden. 12 Furthermore, individuals from different birth cohorts have been exposed to distinct historical, cultural, and lifestyle contexts, which further modulate the disease burden. 8 These variables are indispensable for a precise and comprehensive assessment of pancreatic cancer burden. Therefore, this study utilizes the latest GBD 2021 data to conduct a comprehensive analysis of the gender difference in smoking-related burden of pancreatic cancer in China over the past 30 years and forecast for the next 15 years, aiming to fill existing research gaps and provide reference for policy-making in prevention and treatment.
Materials and Methods
Data Source
The data used in this study were freely obtained from GBD 2021 (https://ghdx.healthdata.org), which is provided by the Institute for Health Metrics and Evaluation, University of Washington, and the data are credible and reliable. This study, which integrates data from national cancer registries, vital registration systems, household surveys, and hospital records, analyzed 447 334 cases of pancreatic cancer in China from 1990 to 2021 where the cause was attributed to smoking. To address the issue of missing data, the MR-BRT (Meta-Regression—Bayesian, Regularized, Trimmed) method was utilized, incorporating correction factors to adjust for potential data biases. The specific methods are as follows: GBD Estimates were categorized as “Risk factor,” with “Measure” denoting “Deaths” and “DALYs,” “Metric” representing “Number, Percent, and Rate,” “Risk” defined as “Smoking,” “Cause” as “Pancreatic Cancer,” “Location” as “China,” “Sex” as “Both, Male, and Female,” and “Year” covering the range of “1990-2021.” The GBD study employs standardized inclusion and exclusion criteria, which have been comprehensively described in previous literature. 13 The inclusion criteria for this study are the same as those described above. For exclusion criteria, individuals with missing data for any key variables specified in the inclusion criteria were excluded. Additionally, individuals with other severe chronic conditions (such as advanced heart failure, end-stage renal disease) that could potentially confound the relationship between smoking and pancreatic cancer burden were also excluded. Since there are very few relevant patients under 30 years of age (negligible), the age groups included in the study ranged from 30 to over 95 years, segmented into 14 age groups every 5 years. According to the International Classification of Diseases, 10th Edition (ICD-10), pancreatic cancer is coded as C25-C25.9 and Z85.07.14,15 The research methods and statistical modeling of GBD 2021 have been described in detail in previous literature.16,17
Joinpoint Regression Analysis
We employed Joinpoint software to assess the temporal trends of age-standardized mortality rates (ASMR) and age-standardized DALY rates (ASDR),
18
estimating the annual percentage change (APC), average annual percentage change (AAPC), and their 95% confidence intervals (CI), which express the statistical significance of trend directions. We observed which segments showed statistical significance (P < 0.05). An APC greater than 0 indicates an upward trend, while an APC less than 0 signifies a downward trend, and segments close to zero represent stability. In both formulas, n stands for the number of age groups. W
i
refers to the weight of the ith age group in the standard population. This weight indicates the proportion of individuals in that particular age group within the structure of the standard population. mi represents the ASMR of the disease under study in the ith age group of the study population. Meanwhile, di denotes the ASDR of the disease in the ith age group of the study population.

Age-Period-Cohort Analysis
The age-period-cohort analysis model is frequently used in statistical and epidemiological research, capable of assessing mortality trends from age, period, and cohort perspectives. Unlike traditional analysis methods, this model employs the intrinsic estimator (IE), providing reliable results without restrictive assumptions and broad applicability.19,20 Moreover, when analyzing the disease burden among different birth cohorts, the annual data were divided into separate age groups and then traced back to their respective birth cohorts. Although the time range of this study extends from 1990 to 2021, the data included are from individuals born in 1900 and later years.
Decomposition Analysis
Using decomposition analysis, we identified the impacts of demographic age structure, population growth, and epidemiological changes on disease burden from 1990 to 2021. This method allows for deeper insight into the significance of population and health system factors concerning disease burden. Changes in age structure may reflect population aging trends. Age-adjusted mortality and DALY rates represent epidemiological changes, while population growth is determined by overall changes.
Autoregressive Integrated Moving Average Model
We utilized the autoregressive integrated moving average (ARIMA) model to predict the number of pancreatic cancer deaths, ASMR, DALYs, and ASDR attributed to smoking in China over the next 15 years, employing the “forecast” package (version 8.23.0). In addition, to guarantee the reliability, validity, and accuracy of the prediction, relevant tests were carried out. These tests aimed to verify the stationarity of the time series, the absence of seasonality, and the normality of residuals. The outcomes suggest that the assumptions of the ARIMA model were met in our research. All statistical analyses and visualizations were conducted using R software (version 4.4.1).
Ethical Statement
This study complies with the GATHER guidelines. 21 The data employed in this study are aggregated, ensuring that no information of individual patients or public personnel is directly implicated.
Results
Descriptive Analysis
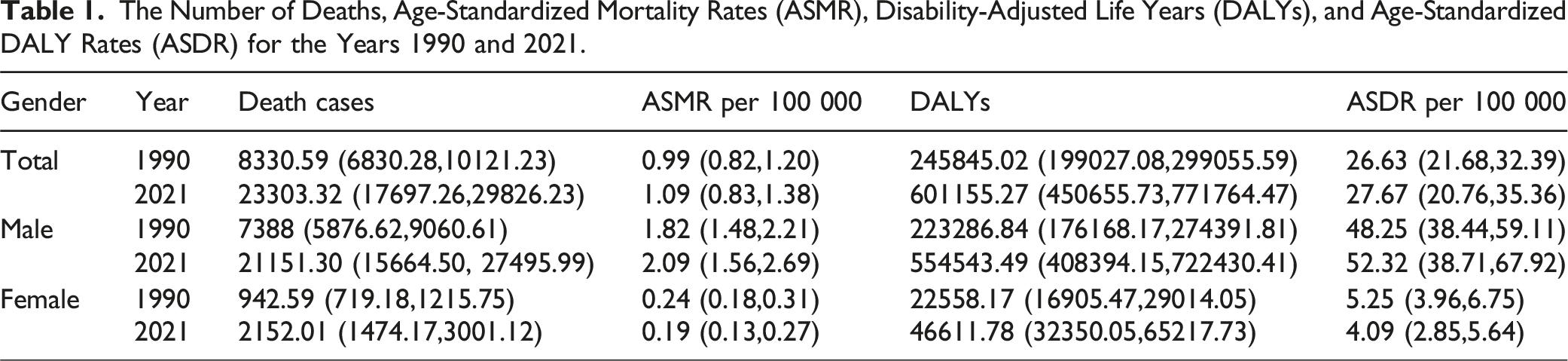
The Number of Deaths, Age-Standardized Mortality Rates (ASMR), Disability-Adjusted Life Years (DALYs), and Age-Standardized DALY Rates (ASDR) for the Years 1990 and 2021.

The Number of Deaths, Age-Standardized Mortality Rates, Disability-Adjusted Life Years (DALYs), and Age-Standardized DALY Rates Attributable to Smoking-Related Pancreatic Cancer in China in 2021, Differentiated by Gender.
Figure 2 shows that from 1990 to 2021, the number of deaths and DALYs due to smoking in both male and female pancreatic cancer patients steadily increased. Despite a similar trend for both genders, the number of cases in men far exceeded those in women across all years, with the gap widening over time. When examining the age-standardized mortality and DALY rates, men displayed a fluctuating increasing trend, while women showed a slight early increase before gradually decreasing from 1996 onward. Clearly, men bore a heavier disease burden compared to women. Trends in Deaths, Age-Standardized Mortality Rates, DALYs, and Age-Standardized DALY Rates Related to Smoking-Induced Pancreatic Cancer in China From 1990 to 2021, Differentiated by Gender.
Joinpoint Regression Analysis
Trends in Age-Standardized Mortality and DALY Rates (per 100 000 Individuals) for Pancreatic Cancer Caused by Smoking in China From 1990 to 2021.

*P < 0.05.

Temporal Trends of Age-Standardized Mortality Rates (ASMR) and Age-Standardized DALY Rates (ASDR) Associated With Pancreatic Cancer due to Smoking From 1990 to 2021.
Age-Period-Cohort Effects
The age-period-cohort model analyzing the effect of age, period, and cohort on mortality and DALY rates illustrated different patterns of change due to age and time. Figures 4A and 5A depict the trends of mortality and DALY rates by age for the years 1992, 1997, 2002, 2007, 2012, and 2017. Mortality and DALY rates rapidly increased from ages 30 to 70, with DALY rates peaking at age 70. Mortality rates experienced milder changes from ages 70 to 80, while DALY rates gradually declined. From ages 80 to 85, both mortality and DALY rates again exhibited an upward trend, peaking around age 85, followed by a decline in both rates. Figures 4B and 5B show the cohort trends in mortality and DALY rates due to pancreatic cancer from smoking across different age groups. Figures 4C and 5C illustrate the changes in smoking-related pancreatic cancer mortality and DALY rates across different age groups from 1990 to 2021. For the age groups of 70 to 90 years, both mortality and DALY rates exhibited an upward trend, while other age groups largely demonstrated a trend of first decreasing and then increasing. The age group with the highest mortality rates in recent years has been 85 to 89 years, while the age group of 70 to 75 years has consistently had the highest DALY rates over the past 30 years. Figures 4D and 5D describe the changes in mortality and DALY rates based on specific age cohort groupings. Age-specific Annual Percentage Change (APC) in Age-Standardized Mortality Rates Caused by Smoking-Related Pancreatic Cancer in China. (A) Trends in Mortality Rates Across Different Age Groups Over Various Time Periods; Each Line Represents a 5-Year Interval. (B) Mortality Trends for Different Birth Cohorts by Age; Each Line Represents a 5-Year Birth Cohort Period. (C) Mortality Trends for Different Age Groups Based on Diagnostic Year; Each Line Corresponds to a 5-Year Age Group. (D) Mortality Trends Across Various Age Groups for Different Birth Cohorts; Each Line Signifies a 5-Year Age Group. Age-specific Annual Percentage Change (APC) in Age-Standardized DALY Rates due to Smoking-Related Pancreatic Cancer in China. (A) Trends in DALY Rates Across Different Age Categories Over Various Time Periods; Each Line Corresponds to a 5-Year Interval. (B) Trends in DALY Rates for Different Age Groups by Birth Cohort; Each Line Represents a 5-Year Birth Cohort Period. (C) Trends in DALY Rates by Diagnostic Year Across Various Age Groups; Each Line Indicates a 5-Year Age Group. (D) Trends in DALY Rates Among Different Age Groups by Birth Cohorts; Each Line Signifies a 5-Year Age Group Period. Figure 5.

Decomposition Analysis of Smoking-Induced Mortality and DALYs in Pancreatic Cancer
The decomposition analysis of smoking-related pancreatic cancer deaths and DALYs from 1990 to 2021 is illustrated in Figure 6. For mortality, population growth emerged as the predominant driving factor, while epidemiological changes and population aging exerted similar effects on both genders. Males were significantly more affected by population growth than females, while epidemiological changes were also a considerable driver for male mortality. Conversely, epidemiological changes and population aging appeared to restrain increases in female mortality, thereby alleviating the overall burden to some extent. As for DALYs, population growth remained the dominant driving force, followed by population aging, with epidemiological changes exerting the least impact on both genders. Compared to females, the influence of population growth on males was more pronounced. Furthermore, population aging contributed significantly to increases in DALYs, with a larger effect on males. Notably, epidemiological changes had a suppressive effect on female DALYs while being a driving force for male DALYs. The decomposition analysis highlighted the interrelationships among population growth, population aging, and epidemiological shifts in influencing the changing smoking-attributed pancreatic cancer burden in China. The Relative Contributions of Three Factors—Population Growth, Population Aging, and Epidemiological Changes—To the Number of Deaths and DALYs From Pancreatic Cancer Attributable to Smoking in China From 1990 to 2021. The Black Dots in the figure represent the Cumulative Effect of These Three Factors. (A) Decomposition of Deaths Changes for Males, Females, and Both Genders. The X-Axis Label ‘Value’ Represents the Number of Deaths in Thousands. (B) Decomposition of DALYs Changes for Males, Females, and Both Genders. The X-Axis Label ‘Value’ Represents the Number of DALYs in Thousands.
Burden of Pancreatic Cancer Attributed to Smoking in China Projected for the next 15 Years
Projection of the burden of smoking-related pancreatic cancer in China for the next 15 years indicates that the ASMR will increase from 2.09 per 100 000 for males in 2021 to 2.22 per 100 000 by 2036. In contrast, the ASMR for females will decrease from 0.19 per 100 000 to 0.17 per 100 000. Similarly, male ASDR is projected to increase from 52.32 per 100 000 in 2021 to 55.14 per 100 000 in 2036, while the ASDR for females will decrease from 4.09 per 100 000 to 4.00 per 100 000. Over the next 15 years, the disparity in burden between males and females is expected to widen, with males experiencing a significantly greater burden than females Figure 7. Trends in Mortality and DALY Rates for Smoking-Related Pancreatic Cancer in China From 2022 to 2036. (A, B) Age-Standardized Mortality Rates for Males and Females, Respectively. (C, D) Age-Standardized DALY Rates for Males and Females, Respectively.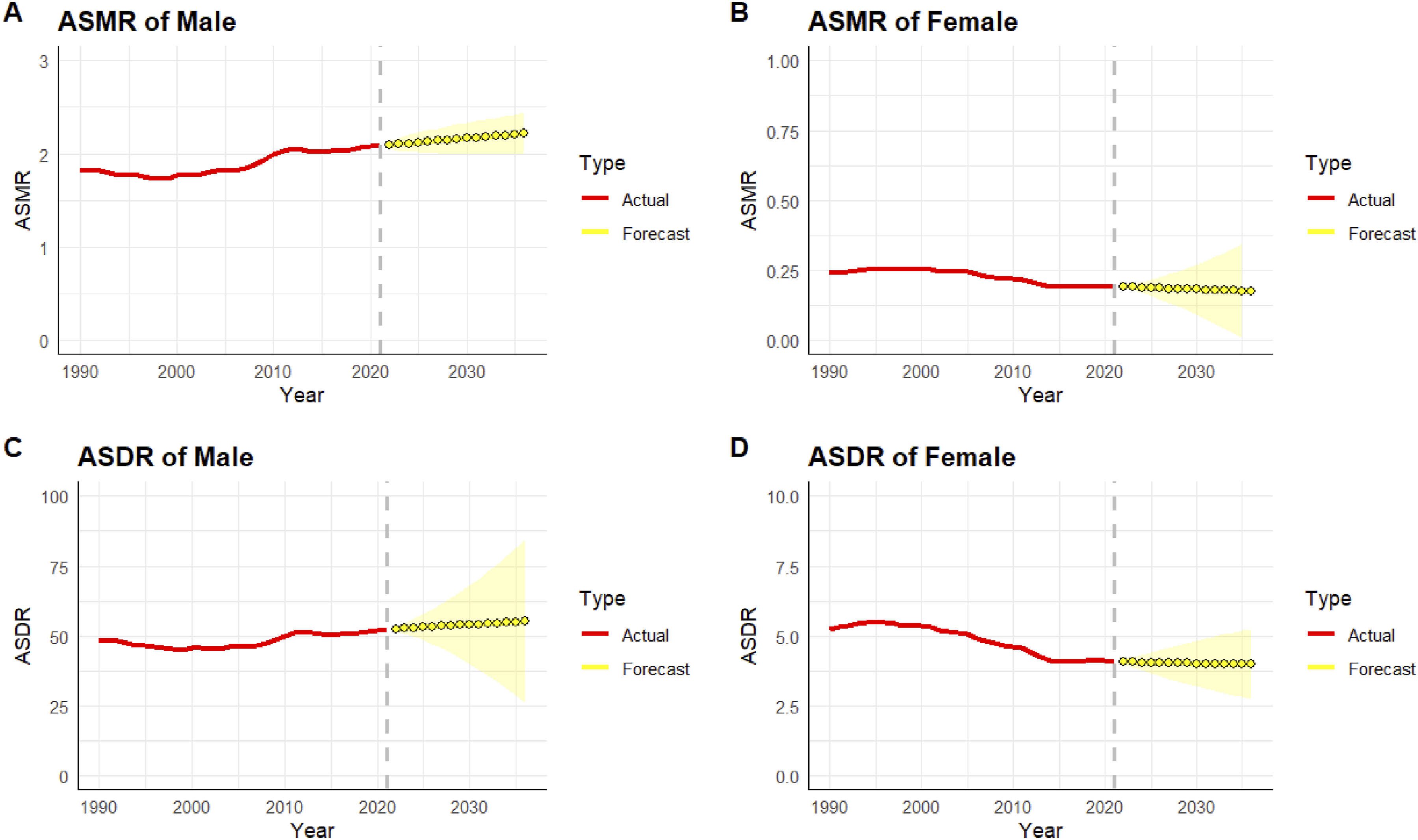
Discussion
Pancreatic cancer is a malignant tumor characterized by its high fatality rate. Over the past 30 years, there has been a significant increase in the burden of pancreatic cancer worldwide, more than doubling in some regions. 22 Not only do metabolic risk factors contribute to the occurrence and progression of pancreatic cancer, 23 but lifestyle risk factors, such as smoking, also play a crucial role in the burden of this disease. Previous studies have identified smoking as the largest risk factor contributing to age-standardized mortality rates of pancreatic cancer worldwide. 16 In China, the burden of pancreatic cancer remains concerning, and understanding smoking, a risk factor strongly associated with pancreatic cancer, can help the Chinese government implement effective prevention and control measures to mitigate the severe disease burden. Therefore, this study utilizes the latest 2021 Global Burden of Disease (GBD) data to analyze trends in the disease burden of smoking-related pancreatic cancer in China from 1990 to 2021 from multiple perspectives, including gender, age, period, and cohort. Using decomposition analysis, we clarify the impact of three factors—population aging, population growth, and epidemiological changes—on the disease burden and predict mortality and DALY rates for the next 15 years.
To the best of our knowledge, this is the first comprehensive assessment of the epidemiological trends of smoking-related pancreatic cancer in China. The results indicate that, from 1990 to 2021, the number of deaths and DALYs due to smoking-related pancreatic cancer in China has shown an overall upward trend for males and females, while the age-standardized mortality rates (ASMR) and age-standardized DALY rates (ASDR) have generally increased for males and decreased for females. The burden is heavier for males compared to females, which aligns with global trends, 24 and similar trends have also been observed in Australia. 25 Joinpoint regression analysis revealed key turning points in the ASMR and ASDR over time. The age-period-cohort model displayed that mortality and DALY rates peak at approximately 85 and 70 years of age, respectively, indicating a substantial disease burden among the elderly. Decomposition analysis revealed that the primary driving factor for both mortality and DALY rates was population growth, with epidemiological changes contributing significantly to mortality and population aging contributing substantially to DALY rates. Although female ASMR and ASDR may show a declining trend over the next 15 years, the absolute numbers remain concerning, and the burden on males continues to increase. In the broader context of China’s large and aging population, these findings emphasize the substantial public health impact of smoking on pancreatic cancer and highlight the need for the formulation of tailored prevention and control measures targeting high-risk populations and specific risk factors.
Smoking is a well-established risk factor for many cancers, including pancreatic cancer. It has been shown that smoking induces the overexpression of CBX3 in pancreatic cancer cells and tissues, thereby inhibiting the expression of SMURF2 and promoting malignant progression. 26 Research on smoke produced by smoking indicates that it contains at least 250 harmful chemicals, 60 of which are carcinogenic. 27 Tobacco smoke promotes the proliferation of pancreatic cancer cells by activating adrenergic receptors and stimulating extracellular signal-regulated kinase phosphorylation. 28 Nicotine, one of the most prevalent carcinogens in smoke, has been found in mouse studies to facilitate the progression of pancreatic cancer by downregulating GATA6, inducing acinar cell dedifferentiation. 29 Furthermore, studies indicate that smokers who quit are much less likely to develop pancreatic cancer than non-smokers. 30 Thus, enhancing health education initiatives and encouraging smokers to quit early is critically important. Furthermore, frequent consumption of red meat and processed meat products has been associated with an increased risk of pancreatic cancer. 31 Other risk factors, such as obesity, 32 diabetes,33-35 chronic pancreatitis,36,37 and alcohol consumption, 38 are also linked to a higher likelihood of developing pancreatic cancer. When these factors are combined with smoking, they exhibit a synergistic effect, accelerating disease progression and ultimately leading to higher mortality rates. Although healthcare infrastructure in China has improved in recent years, disparities in medical resources across different regions persist. High-quality healthcare services are concentrated in limited areas, which hinders the early detection and treatment of smoking-related pancreatic cancer. Additionally, the lack of emphasis on pancreatic cancer screening and the limited treatment options for advanced-stage disease contribute to poor prognosis and elevated mortality rates.
There is a notable gender difference in the mortality and DALY rates due to smoking-related pancreatic cancer in China, with the overall burden among males being greater than that among females, particularly in the elderly demographic aged 70-90. The relatively lower mortality and DALY rates for females may correlate with a lower prevalence of female smokers. Research reveals that the global male smoking rate (25%) is approximately five times that of females (5.4%), with figures in China far exceeding these global averages. 39 The relative estrogen deficiency in female smokers is also a significant contributor to the gender disparity. 40 Estrogen may improve metabolism and regulate inflammatory responses, potentially playing a preventive role against pancreatic cancer. A meta-analysis has shown 41 that the duration and dosage of smoking also play roles in gender differences, although further investigation is required. Moreover, risk factors such as smoking and alcohol consumption are more common in men, which significantly increases the incidence of pancreatic cancer mortality. 42 Research from Switzerland indicates that tobacco control is currently the most effective measure to prevent cancer deaths. 43 However, in China, awareness of the hazards associated with smoking is often lacking. Smoking frequently serves as a significant means of social interaction among men in certain contexts. Expensive cigarettes act as a form of social currency, being shared as a gesture of friendship, thus bridging social connections.44,45 The potential negative impact of quitting smoking on traditional social behaviors, alongside ingrained mindsets, poses challenges to the implementation of smoking cessation policies in China. Such challenges may hinder government efforts to promote smoke-free environments and smoking restrictions, 46 and the establishment of smoking cessation clinics 47 may also face obstacles. Therefore, there is a critical need for substantial improvements in smoking behavior in China, and it is essential for relevant authorities to establish robust policies to alter these detrimental practices, which would ultimately benefit long-term health and mitigate disease burdens.
Our findings indicate that the disease burden varies significantly across different age groups. Over the past 30 years, mortality and DALY rates have shown an initial rise followed by a decline with increasing age, peaking at about 85 years and 70 years, respectively. The harmful effects of smoking develop gradually; since most smokers begin smoking at a young age, 48 early harm often remains inconspicuous, contributing to the overall disease burden in the elderly population. As the country with the largest elderly population globally, China faces an increasingly severe aging situation 49 that necessitates urgent attention to public health issues arising from it. Additionally, older patients often present with characteristics such as reduced immunity, malnutrition, numerous underlying conditions, and inadequate health awareness, rendering the treatment and prognosis of pancreatic cancer quite challenging. Consequently, improving disease awareness among older adults, implementing appropriate incentive measures, and effectively preventing complications are all very beneficial objectives. Moreover, a health survey in China has indicated a significant decline in the age at which individuals begin smoking, from 22 years to 17.5 years. 50 Tobacco control measures targeting adolescents in China require further strengthening, and relevant legislation needs improvement, such as increasing penalties for selling tobacco to minors.
In conclusion, the burden of pancreatic cancer attributed to smoking in China from 1990 to 2021 remains substantial, and significant investments of human, material, and financial resources are needed to mitigate the harms of smoking-related pancreatic cancer from the root. Given the differences in gender and age, public health systems should prioritize treatment and prevention of pancreatic cancer in vulnerable groups, particularly elderly males. On one hand, pancreatic cancer health education activities should be conducted in areas significantly populated by the elderly, promoting healthy eating, encouraging appropriate medical consultations, and facilitating early detection, diagnosis, and treatment. On the other hand, the significant challenge of smoking cessation in high-risk populations must be addressed, such as through raising tobacco prices 51 and increasing the visibility of health warnings on tobacco packaging, 52 which would help reduce tobacco consumption and lower smoking rates. Adolescents, who represent the future of the nation, must be protected from the harms of smoking and encouraged to say “no” to tobacco. In such a vast country as China, various provinces should develop tailored plans aimed at differentiated prevention and treatment strategies for various populations to avoid irrational allocation of medical resources that could lead to wastage.
The strength of this research lies in its use of the latest statistical data to comprehensively analyze national burden trends, employing decomposition analysis for the first time to assess the primary driving factors behind mortality and DALY rates, thus providing new references for practitioners. Despite these valuable findings, this study does have several limitations. Firstly, the inherent limitations of the GBD2021 database impact this research. These limitations include biases arising from methodological assumptions, heterogeneity introduced during data aggregation, and other constraints mentioned elsewhere. Secondly, our comprehensive analysis of the national burden of pancreatic cancer attributable to smoking did not fully explore the differences between various provinces and rural-urban divides in China, with inevitably missing data in remote areas. Finally, this study treats smoking as an independent influencing factor; however, in reality, it interacts with other factors such as obesity, type 2 diabetes, chronic pancreatitis, and alcohol use disorder. Over the past three decades, obesity 32 and type 2 diabetes33-35 have emerged as significant public health challenges in China and are also important risk factors for pancreatic cancer, with their prevalence steadily increasing. The incidence of chronic pancreatitis in China has also continued to rise, 36 and individuals with chronic pancreatitis face a 13-fold higher risk of developing pancreatic cancer compared to the general population. 37 Similarly, alcohol consumption in China has been on the rise, 38 and alcohol use disorder may influence the prevalence of chronic pancreatitis and obesity. These factors, directly or indirectly, contribute to the burden of pancreatic cancer associated with smoking. This study did not explicitly control for these confounding variables, and future research should consider incorporating them to provide a comprehensive understanding of their complex roles in the burden of pancreatic cancer.
Conclusion
In summary, the burden of pancreatic cancer attributable to smoking in China has increased from 1990 to 2021, and the outlook remains dire, with smoking still being the primary risk factor for pancreatic cancer. The burden on males is significantly higher than that on females. Implementing vigorous smoking cessation and control measures targeting elderly males and restricting high-risk populations from tobacco exposure could greatly alleviate the burden of pancreatic cancer. Given the lethality of pancreatic cancer, increased investment in research related to pancreatic cancer remains crucial to overcoming medical challenges.
Footnotes
Acknowledgements
We are grateful to the Global Burden of Disease Study 2021 database, which provided the raw data for the study.
Ethical Statement
Author Contributions
HW: study conception, design, data analysis, and manuscript writing; WS and JZ: data organization and manuscript preparation; GW and ZD: manuscript preparation; ZJ: study conception, design, and provided funding, resources, and writing guidance. All authors reviewed and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to acknowledge the financial support received for this research article. Specifically, this study was funded by the China Medical Education Association under the 2022 Major Scientific Research Topics (No. 2022KTZ005), the Jiangsu Province 14th Five-Year Medical Key Discipline in Traditional Chinese Surgery (No. ZDXK202251) and the Leading Talents Training Project of Traditional Chinese Medicine in Jiangsu Province (No. SLJ0311).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.