
Abstract
Plain Language Summary
Why was the study done? This study was conducted to understand the global impact of rare cancers known as soft tissue and other extraosseous sarcomas (STOES). These cancers, although rare, significantly affect patients worldwide, making it important to monitor their occurrence and impact. What did the researchers do? We analyzed global health data from 1990 to 2021 to find out how many people are diagnosed with these cancers each year, how many live with them, and how many die from them. We examined these trends across different global regions and among various demographic groups. What did the researchers find? By 2021, approximately 480,473 people worldwide were living with these cancers, an increase from 1990. The highest rates of these cancers were in economically developed regions, with significant increases also noted in Central Asia, Central Europe, and Southern Sub-Saharan Africa. Men were more affected than women. The rise in cases is attributed to an aging population and overall population growth. We predict a decrease in these cancer cases by 2030, although regional and gender disparities will persist. What do the findings mean? The findings emphasize significant regional and demographic variations in the incidence of these rare cancers. Recognizing these patterns allows for better allocation of health resources and guides research efforts. Despite a projected decrease in cases, ongoing efforts are needed to address disparities through targeted health policies and improved early detection, diagnosis, and multidisciplinary management of STOES.
Keywords
Introduction
Soft Tissue and Other Extraosseous Sarcomas (STOES), rare and highly aggressive, comprise less than 1% of all adult malignant tumors.1,2 Predominantly located in the extremities (59%), trunk (19%), retroperitoneum (15%), and head and neck (9%), these tumors present significant clinical challenges due to complex treatment protocols. 3 Although extensive local excision and radiation therapy may enhance local control, approximately one-third of all patients with high-risk soft tissue sarcomas remain at risk for metastasis and death.2,4 In 2018, approximately 13,040 individuals in the United States were diagnosed with soft tissue sarcoma (STS), resulting in about 5150 fatalities. These figures likely underestimate the actual disease burden. 3 Consequently, comprehending the global burden of STOES is essential for devising effective public health strategies and allocating resources.
Systematic monitoring of cancer burden variations across diverse populations, geographical regions, and temporal spans is indispensable for strategic health planning and establishing priorities in clinical care and research. Policymakers depend on granular, region-specific data to rigorously evaluate the effectiveness of cancer control programs, monitor their progress, and allocate resources with precision.5,6 However, the literature remains deficient in detailed studies addressing the integration of STOES into the Global Burden of Disease (GBD) database. In contrast to previous iterations of the GBD, which non-specifically categorized such tumors under “other malignant tumors”, the 2021 update of the GBD methodologically distinguishes STOES.7,8 This innovation emphasizes the profound necessity for and substantial value of comprehensive data collection in this specialized field.
This study aims to comprehensively assess the global disease burden of STOES by analyzing the GBD database. We seek to address gaps in the literature by elucidating the impact of STOES across various regions and populations, thereby underpinning public health policy and intervention strategies. By clarifying the epidemiological characteristics and burden of these tumors, we will develop more effective diagnostic more effective diagnostic and treatment strategies to enhance patient survival and quality of life. Additionally, this research will inform future studies and foster global focus and resource allocation for improving early detection, diagnosis, and multidisciplinary management of STOES.
Methods
We extracted annual data on incident cases, prevalent cases, deaths, disability-adjusted life years (DALYs), age-standardized incidence rates (ASIRs), age-standardized prevalence rates (ASPRs), age-standardized mortality rates (ASMRs), and age-standardized DALY rates (ASDRs) of STOES from 1990 to 2021, by location and sex from the Global Health Data Exchange (GHDx) query tool (https://ghdx.healthdata.org/gbd-results-tool). Data were available from a total of 204 countries and territories. These regions were categorized into five groups based on the socio-demographic index (SDI) and 21 GBD regions according to geographical proximity. 9
Data on socioeconomic status, including the SDI for 2021 and the Universal Health Coverage Index (UHCI) values for 2019, were collected using the GHDx query tool. 10 Additionally, the Human Development Index (HDI) data for 2021 were sourced from the 2023-2024 Human Development Report. 11
Ethical Statement
The data used in this study were sourced from the GBD 2021 database (https://vizhub.healthdata.org/gbd-results), thus, ethical approval was not required. This study complies with the GATHER guidelines. 12
Statistical Analysis
EAPC
Estimated annual percentage change (EAPC) 13 is a summary and widely used measure of age-standardized rates (ASRs) 14 tend over a specified time interval. A regression line was fitted to the natural logarithm of the ASR, ie, y = α + βx + ε, where y = ln (ASR) and x = calendar year. EAPC was calculated as 100*(eβ−1) with its 95% confidence interval (CI) reflecting the temporal trend in ASR. The trend in ASRs was reflected in the EAPC value and its 95% CI: ASR indicates an upward trend when the EAPC and the lower bound of the 95% CI are positive; conversely, ASR indicates a downward trend when the EAPC and the upper bound of the 95% CI are negative.
Joinpoint Regression Analysis
Joinpoint regression analysis was employed to evaluate the temporal trends in ASIR, ASPR, and ASMR between 1990 and 2021. The annual percent change (APC) and average annual percent change (AAPC) were calculated to estimate the changes in STOES across multiple sub-periods and the overall study period, respectively. A 95% CI for the APC or AAPC entirely above, below, or including zero was interpreted as indicating an increasing, decreasing, or stable trend, respectively. 15
Correlation Analysis
Spearman correlation analyses were conducted to assess the correlations between EAPCs and SDI values (2021), UHCI values (2019), and HDI values across 204 countries and territories. 16
Decomposition Analysis
Decomposition analysis is employed to pinpoint the factors contributing to changes in the absolute number of age-related disease burdens. 17 This method identifies the additive effects of differences in factors between two groups (specifically, populations in 1990 and 2021) and their impact on the overall disease burden. We conducted a decomposition analysis to evaluate DALY changes between 1990 and 2021, focusing on three factors: (1) age structure, (2) epidemiologic changes, and (3) population size. This analysis enables us to quantify the contribution of each of these factors to the overall changes in DALYs.
Bayesian Age-period-cohort
Comparative studies have shown that age-period-cohort methods outperform time series approaches in predictive performance. Notably, the probabilistic forecasts generated by the Bayesian age-period-cohort (BAPC) model are well-calibrated and maintain a reasonable range.18,19 The rationale for the BAPC model has been previously described. 20 Using the BAPC model, we projected the absolute numbers, rates, and ASRs for STOES until 2030.
All statistical analyses were conducted utilizing R software, version 4.2.2. A two-tailed P-value less than 0.05 was considered statistically significant.
Results
Global Level
Age-Standardized Rates of Incidence and Mortality per 100,000 Population in 1990 and 2021, and EAPC From 1990 to 2021 for STOES, by SDI Quintiles and 21 GBD Regions

STOES, soft tissue and other extraosseous sarcomas; ASR, age-standardized rates; EAPC, estimated annual percentage rate; SDI, socio-demographic index; UI, uncertainty interval; CI, confidence interval.
Joinpoint regression analysis revealed distinct temporal trends in ASIR, ASPR, ASMR, and ASDR between 1990 and 2021 (Supplemental Table 5, Supplemental Figure 1). ASIR increased significantly between 1990 and 1995 (APC: 1.41), followed by fluctuations and a marked decline from 2018 to 2021 (APC: −1.43). The overall ASIR trend demonstrated a modest but statistically significant decline (AAPC: −0.13) (Supplemental Table 5, Supplemental Figure 1A). A similar pattern was observed for ASPR, with a significant increase from 1990 to 1995 (APC: 1.42) and a pronounced decline from 2018 to 2021 (APC: −1.47). The overall ASPR exhibited a significant downward trend (AAPC: −0.10) (Supplemental Table 5, Supplemental Figure 1B). ASMR consistently declined across all time intervals, with the greatest reduction observed between 1995 and 2001 (APC: −1.47). The overall ASMR trend showed a substantial and consistent decrease (AAPC: −0.66) (Supplemental Table 5, Supplemental Figure 1C). Similarly, ASDR exhibited a continuous and statistically significant decline over the study period. The most pronounced decline occurred from 2018 to 2021 (APC: −1.76), with an overall AAPC of −0.94 (Supplemental Table 5, Supplemental Figure 1D).
Regional Level
In 2021, the high SDI quintiles recorded the highest ASIR (2.05 per 100,000 population) and ASPR (10.61 per 100,000 population) among all SDI quintiles (Table 1, Supplemental Table 2). However, the highest ASMR (0.95 per 100,000 population) and ASDR (33.41 per 100,000 population) were recorded in low SDI quintiles, and subsequently in high SDI quintiles (Table 1, Supplemental Table 4). From 1990 to 2021, only high SDI quintiles exhibited an increasing pattern in incidence and prevalence (EAPC of 0.17 and 0.23), while middle, low-middle and low SDI quintiles exhibited declines (Table 1, Supplemental Tables 1-4). The mortality and DALYs decreased across all SDI quintiles. In 2021, High-income North America, Australasia, and Western Europe exhibited the highest ASIRs for STOES at 2.63, 2.52, and 2.41 per 100,000 population, respectively, among the 21 GBD regions. Germany, Malta, and Bermuda recorded the highest ASIR of 2.77, 2.74, and 2.7 per 100,000 population, respectively. Similarly, they reported the highest ASPR of 14.38, 14.51, and 13.95 per 100,000 population, respectively (Table 1, Supplemental Tables 1 and 2). Eastern Sub-Saharan Africa reported the highest ASMR and ASDR at 1.58 and 53.14 per 100,000 population, respectively, the highest country-specific rates in Uganda and South Sudan (Table 1, Supplemental Tables 3 and 4). Oceania exhibited the lowest rates of ASIR, ASPR, ASMR, and ASDR among all regions (Table 1, Supplemental Tables 1-4).
From 1990 to 2021, nearly half of the countries experienced an increase in STOES incidence and prevalence, with decreases in mortality and DALYs in about three-quarters (Figure 1, Supplemental Figures 2 and 3). Significant increases in all STOES burden indicators were observed in Central Asia, Central Europe and Southern Sub-Saharan Africa. Conversely, significant declines were noted in East Asia, Southeast Asia, South Asia, Oceania, Central Sub-Saharan Africa, North Africa and Middle East, and Eastern Sub-Saharan Africa. Among individual countries, Georgia exhibited the greatest increase, while the Maldives experienced the largest decrease (Table 1, Supplemental Tables 1-4). The Geographical Distribution of EAPC in the Age-Standardized Incidence Rates (A) and Mortality (B) for STOES Burden Globally From 1990 to 2021. STOES, Soft Tissue and Other Extraosseous Sarcomas; EAPC, Estimated Annual Percentage Change
Age and Sex Patterns
In 1990, children aged 0-4 experienced the highest disease burden across all STOES metrics, with ASDR being more than double that of other age groups (Figure 2). By 2021, although conditions for the 0-4 age group had improved, the metrics remained elevated. After age 5, ASIR and ASPR progressively increased with age, reaching their peak at 70-74 years, identifying 65-79 years as the primary high-risk group (Figure 2A and B). The age group exhibiting the highest ASMR transitioned from 65-69 years in 1990 to 70-74 years in 2021, whereas the peak burden of DALYs shifted to a younger cohort at 60-64 years (Figure 2C and D). Population Pyramid of Incidence (A), Prevalence (B), Mortality (C), and DALYs (D) for STOES by Age Group and Sex in 1990 and 2021. STOES, Soft Tissue and Other Extraosseous Sarcomas; DALYs, Disability-Adjusted Life Year
Globally, males consistently exhibit a higher disease burden of STOES than females. In 1990, the ASIR for males was 1.2 times that of females, which increased to 1.33 by 2021. Similarly, the ASMR for males increased from 1.24 times that of females to 1.35 times (Table 1). Between 1990 and 2021, all metrics of STOES disease burden in females demonstrated a marked decline. Conversely, males showed a significant reduction in both the ASMR and ASDR, with EAPCs of −0.65 and −0.95, respectively. Additionally, there were slight fluctuations in ASIR and ASPR, with EAPCs of −0.06 and −0.01, respectively (Figure 3, Supplemental Tables 1-4). Temporal Trends of Age-Standardized Rates of Incidence, Prevalence, Mortality, and DALYs in Males and Females for STOES From 1990 to 2021. STOES, Soft Tissue and Other Extraosseous Sarcomas; DALYs, Disability-Adjusted Life Year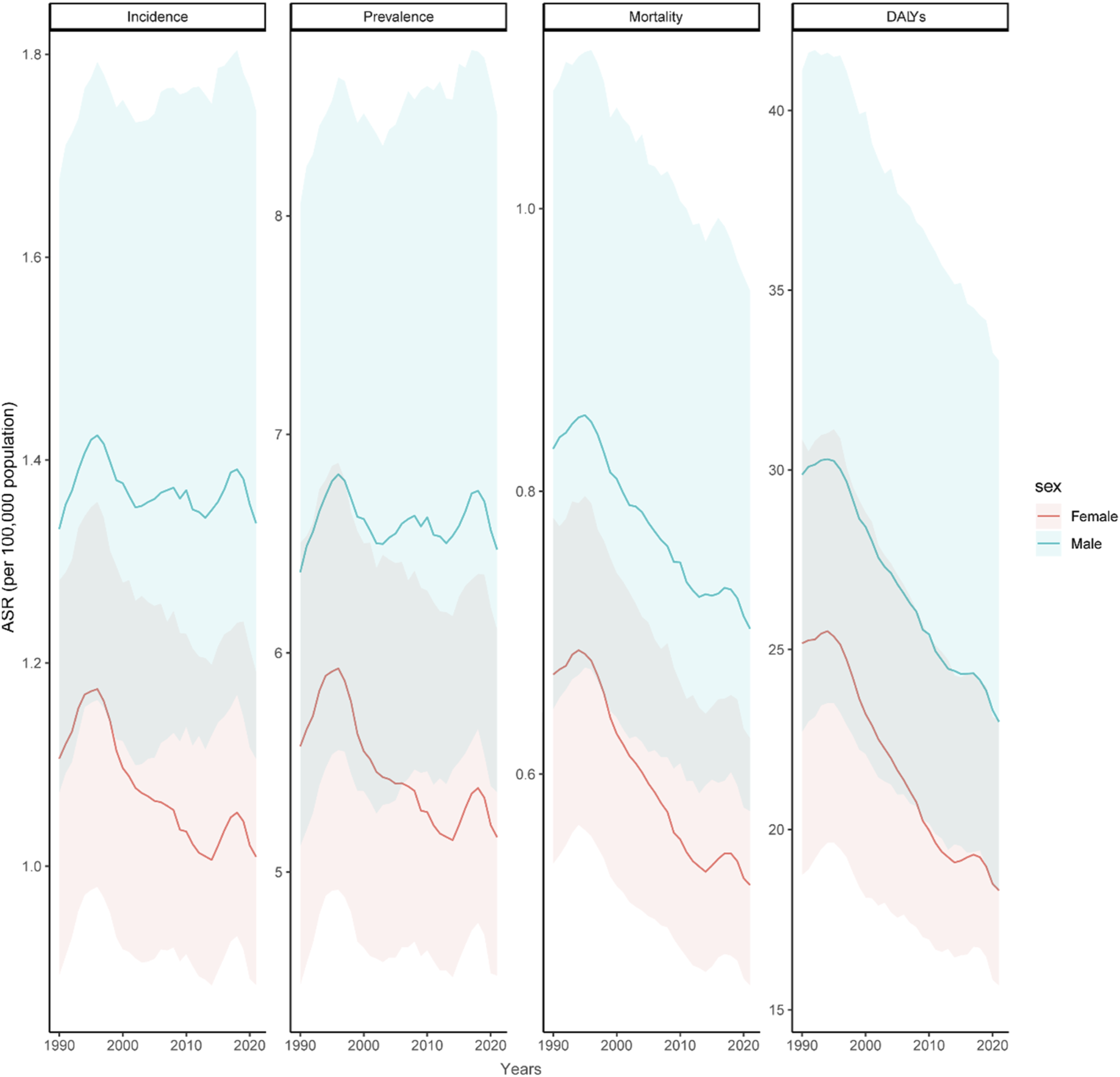
Correlation Analysis
In 1990 and 2021, a positive correlation was observed between SDI, HDI, UHCI, and the ASIR (r = 0.3, 0.38, and 0.41) and ASPR (r = 0.33, 0.41, and 0.44) of STOES, with no correlation to the ASMR and ASDR (Supplemental Figures 4-6). From 1990 to 2021, HDI showed a positive correlation with the EAPCs of ASIR (r = 0.23, P = 0.0018), ASPR (r = 0.26, P = 0.00047), and ASDR (r = 0.16, P = 0.037) (Supplemental Figure 8). However, the EAPC of ASMR displayed no correlation with HDI, and both SDI and UHCI showed no correlation with the EAPCs of these metrics (Supplemental Figures 7 and 9).
Decomposition Analysis
Globally, from 1990 to 2021, population growth contributed the most to the increasing burden of STOES, followed by aging, while epidemiological changes reduced the disease burden (Figure 4). Population growth contributed 184.7% to DALYs, 68.7% to incidence rates, 71.6% to prevalence rates, and 86.5% to mortality rates. In the 21 GBD regions, aging significantly impacted incidence, prevalence, and mortality in East Asia, contributing 112.3%, 107%, and 307.2%, respectively, and was the primary contributor to DALYs in Andean Latin America at 130.1%. Population growth had the highest contributions to incidence and prevalence in Eastern Sub-Saharan Africa at 197.2% and 196.7%, respectively, and to mortality and DALYs in North Africa and the Middle East at 260.9% and Andean Latin America at 523.5%, respectively. Epidemiological changes most significantly affected incidence, prevalence, and mortality in Eastern Europe, contributing 72%, 78.8%, and 43.2%, respectively, with their greatest impact on DALYs in North Africa and the Middle East at 36178.3% (Figure 4, Supplemental Table 6). Decomposition Analysis of Change in Incidence, Prevalence, Mortality, and DALYs for STOES according to Population-Level Determinants of Population Growth, Aging, and Epidemiological Change From 1990 to 2021 by Global and Regions. STOES, Soft Tissue and Other Extraosseous Sarcomas; DALYs, Disability-Adjusted Life Year
Forecast Analysis for 2030
The BAPC prediction model forecasts a decline in the global ASIR of STOES from 1.16 to 0.99 per 100,000 population by 2030 (Figure 5A). Similarly, the ASPR will decrease from 5.78 to 5.02 per 100,000 population, the ASMR from 0.6 to 0.52 per 100,000 population, and the ASDR from 20.53 to 17.57 per 100,000 population (Figure 5B, Supplemental Figures 10 and 11). During this period, although the disease burden will decline for both sexes, the burden in males will remain higher, with male metrics approximately 1.3 times those of females (Supplemental Table 7). Forecasted Change in Temporal Trends of the Numbers and ASR of Incidence (A) and Mortality (B) for STOES Global by Both Sexes, Males and Females From 2021 to 2030. STOES, Soft Tissue and Other Extraosseous Sarcomas; DALYs, Disability-Adjusted Life Year; ASR, Age-Standardized Rates
Discussion
This study provides the first comprehensive analysis of the incidence, prevalence, mortality, and DALYs of STOES at global, regional, and national levels from 1990 to 2021. In 2021, the highest ASIR and ASPR occurred in high SDI quintiles, while the highest ASMR and DALYs were noted in low SDI quintiles. From 1990 to 2021, while the global disease burden of STOES generally declined, significant increases were observed in Central Asia, Central Europe and Southern Sub-Saharan Africa. Incidence and prevalence rates among males were consistently higher than those among females across all metrics. Decomposition analysis identified global population growth as the primary driver behind these increases. Although projections suggest a decline in the global STOES burden by 2030, rates are expected to remain significantly higher among males. These findings emphasize the critical need for targeted interventions and robust health policies to mitigate disparities and alleviate the global burden of STOES.
This study demonstrates that high SDI regions exhibit higher ASIR and ASPR for STOES compared to other SDI regions. Additionally, the EAPC for ASIR and ASPR shows an upward trend, while the EAPC for mortality and DALYs has decreased. Screening programs in high SDI regions, coupled with elevated levels of education and health awareness, contribute to a more proactive approach toward disease screening, potentially leading to increases in the incidence and prevalence rates. For example, Germany has initiated the BURDEN 2020 project, providing policymakers and public health stakeholders with valuable tools for assessing disease burden at national and regional levels. 21 Additionally, these regions are typically equipped with advanced medical technologies and substantial medical resources, enabling more effective treatment and management of STOES. This advanced capability may contribute to the observed decrease in the EAPC of mortality and DALYs. 22 In contrast, regions with lower SDI exhibit higher ASMR and ASDR compared to other SDI regions, most notably in Eastern Sub-Saharan Africa, which notably ranks fourth among the regions for ASIR and ASPR, and recorded the highest ASMR and ASDR, particularly in Uganda and South Sudan. Previous study indicates that HIV prevalence in these areas far exceeds that of other populations, up to eight times higher than the general populace. 23 The incidence of HIV-related Kaposi’s sarcoma in these regions is significantly higher than in other parts of the world. 24 Although the disease burden of STOES generally shows a declining trend, the actual burden may be significantly underestimated. This underestimation likely results from multiple challenges including insufficient cancer research funding, lack of cancer education, inadequate diagnostic facilities, incomplete cancer registries, and a shortage of medical resources.7,25 Therefore, improving access to and quality of medical services for patients with lower socioeconomic status, as well as enhancing cancer surveillance and health data reporting systems in low SDI regions, are crucial to address these challenges and alleviate the disease burden in these areas.
This study observed that from 1990 to 2021, nearly half of the countries showed an increasing trend in the incidence and prevalence of STOES. While all metrics of the global disease burden of STOES generally increased from 1990 to 1995, a downward trend was observed after 1995. This shift coincides with significant advancements in diagnostic technologies and treatment modalities within the field. Innovations such as improved imaging techniques, more precise surgical instruments, and enhanced therapeutic protocols have likely contributed to more accurate diagnosis and effective treatment of STOES, thereby influencing the observed trends.26-28 Furthermore, about three-quarters of the countries showed a decline in mortality and DALYs, which may reflect the effectiveness of global health interventions. Notably, significant increases in all STOES burden indicators were observed in Central Asia, Central Europe and Southern Sub-Saharan Africa. The increase in STOES burden in these regions is likely due to a combination of factors, including limitations in health infrastructure, population growth and aging, low socioeconomic status, and environmental and occupational exposures.29-31 For instance, in many Southern Sub-Saharan African countries, underdeveloped health infrastructure, limited diagnostic facilities, and a lack of specialized services exacerbate the underdiagnosis and undertreatment of STOES, increasing the observed disease burden. 30 Notably, Georgia, despite being a high-middle SDI region, exhibits significantly higher trends in all STOES disease burden metrics than other countries. Research indicates that despite increasing healthcare expenditures, Georgia continues to fall short of not only the standards established by the World Health Organization (WHO) but also those of many low-income nations. 32 Furthermore, previous research indicates that insufficient awareness of early cancer screening among Georgians is a primary cause of low screening rates, with rural areas lagging behind urban ones in development, which also contributes to low screening and poor early diagnosis. 33 Similarly, in low- and middle-income countries, underdiagnosis and misdiagnosis remain significant challenges. Limited access to pathology services, lack of awareness, and incomplete cancer registration systems may result in an underestimation of the true disease burden. 34 Although mortality and DALYs from STOES have declined globally, reflecting progress in health strategies, persistent challenges like inadequate infrastructure, socioeconomic disparities, and occupational exposures necessitate greater investment in public health and early disease screening, especially in low-income regions with high disease burdens.
Consistent with previous research, 35 this study demonstrates that globally, the disease burden of STOES is consistently higher in males than in females, exhibiting a slow but steady increase over time. The influence of sex hormones on cancer cell metabolism, immunity, and the tumor microenvironment, coupled with males’ more frequent exposure to potential carcinogens at work, may explain the sex differences in cancer incidence rates.1,36 The burden of STOES increases with age, peaking between 65 and 79 years, potentially due to chronic conditions prevalent in the elderly, accumulated genetic damage, diminished immune function, chronic inflammation, reduced physical activity, environmental and occupational exposures.37-41 Based on data from 1990 to 2021, predictions using the BAPC model suggest that although the global disease burden of MNBAC is expected to decline from 2021 to 2030, the burden among males is still projected to remain higher than that among females. Since 1990, advancements in early diagnosis and screening technologies, along with enhanced clinical research and international collaboration, have significantly improved the STOES disease burden in children aged 0-4 years. However, due to the propensity for gene fusions leading to cancer and chemotherapy resistance in this age group, the disease burden remains substantial.42,43 Besides biological mechanisms, entrenched cultural norms in several regions give men preferential access to specialist services, whereas women may face geographic, financial or social barriers; such inequities could inflate the apparent male predominance observed in our study.44,45 As most STOES arise sporadically without identifiable behavioral risk factors, conventional primary prevention strategies are unlikely to yield significant population-level benefits. Consequently, public health efforts should prioritize: (i) strengthening pathology and imaging capacities to facilitate prompt diagnosis; (ii) ensuring timely referrals to multidisciplinary sarcoma centers; and (iii) minimizing avoidable iatrogenic, environmental, and occupational radiation exposures associated with specific histological subtypes. Complementary strategies include targeted outreach for men and older adults, investment in genomic research to illuminate actionable molecular drivers, and pediatric-focused initiatives that promote early recognition and screening. Together, these measures offer the most realistic route to reducing the global STOES burden.
Population growth is identified as the primary driver for the increase in the global STOES disease burden, with a particularly pronounced impact on incidence and prevalence rates in Eastern Sub-Saharan Africa. Although the global population growth rate has stabilized and begun to decline since 2017, rapid population growth continues in low-income countries, primarily in Sub-Saharan Africa, where the scarcity of resources and rapid infrastructure expansion remain critical issues. 46 Additionally, the trend of population growth is expected to soon end, and aging populations will increasingly exacerbate the disease burden of STOES, especially in East Asia and the Andean regions of Latin America, presenting unique challenges that require tailored health interventions. 47 While epidemiological changes have reduced the global STOES disease burden, their impact on DALYs is particularly significant in North Africa and the Middle East, likely due to environmental pollution, unhealthy lifestyles, occupational factors, and genetic predispositions.48-50 These results underscore the importance of developing targeted public health strategies and optimizing resource allocation to effectively address the health challenges in specific regions, particularly considering how to manage population structures, enhance the efficiency of public health interventions, and adapt to socio-economic changes to reduce the disease burden.
This study has several limitations related to the use of the GBD database. First, the GBD classification method aggregates all STOES into a single category, overlooking substantial heterogeneity among tumor subtypes. The GHDx, which supports the GBD, relies on the International Classification of Diseases coding system and predictive modeling to estimate global disease burden. However, STOES subtypes are often grouped under broad diagnostic codes, obscuring important biological and clinical differences. Second, incomplete and uneven cancer-registry coverage—especially in many low- and middle-income countries—can bias burden estimates and trend analyses. Where population-based registries are sparse or absent, models must rely on predictive covariates and data borrowed from neighboring countries, increasing statistical uncertainty. Limited diagnostic capacity and urban-centered reporting further under-ascertain sarcoma incidence and mortality, potentially obscuring true temporal patterns. Third, geographic differences in genetic predisposition, environmental exposures, and healthcare access can influence STOES incidence but are unevenly captured in the GBD framework. Lastly, the reliance on historical datasets and predictive algorithms may limit the GBD’s ability to reflect recent changes in disease patterns or advances in diagnostic and treatment strategies. Therefore, when using GBD data to study STOES, it is essential to integrate other data sources and expert knowledge for a comprehensive analysis.
Conclusion
This analysis outlines the epidemiological trends and disparities in the burden of STOES from 1990 to 2021. While the global burden has generally declined, it has risen notably in Central Asia, Central Europe, and Southern Sub-Saharan Africa. Males and the elderly consistently show higher incidence rates, driven largely by global population growth. Projections for 2030 indicate a continued decrease in overall disease burden, yet disparities, especially among males, are expected to persist. These findings highlight the critical need for region-specific public health strategies and policies to address these disparities and mitigate STOES globally.
Supplemental Material
Supplemental Material - Global, Regional, and National Burden and Trends of Soft Tissue and Other Extraosseous Sarcomas From 1990 to 2021
Supplemental Material for Global, Regional, and National Burden and Trends of Soft Tissue and Other Extraosseous Sarcomas From 1990 to 2021 by Rui Zhu, Ziyuan Shen, Haijuan Zhu, Jisen Zhang, Xing Xing, Shengyou Wang, and Jialiu Fang in Cancer Control
Supplemental Material
Supplemental Material - Global, Regional, and National Burden and Trends of Soft Tissue and Other Extraosseous Sarcomas From 1990 to 2021
Supplemental Material for Global, Regional, and National Burden and Trends of Soft Tissue and Other Extraosseous Sarcomas From 1990 to 2021 by Rui Zhu, Ziyuan Shen, Haijuan Zhu, Jisen Zhang, Xing Xing, Shengyou Wang, and Jialiu Fang in Cancer Control
Footnotes
Ethical Considerations
This study used a public database, so ethical approval and consent forms were not required.
Consent for Publication
As this study did not involve personal data, consent for publication was not required.
Author Contributions
Rui Zhu: Writing - original draft, writing - review and editing, conceptualization, data curation, formal analysis, methodology. Haijuan Zhu: methodology, investigation, formal analysis, data curation, visualization, writing - review and editing. Jisen Zhang, Ziyuan Shen, Xing Xing: Formal analysis, investigation, software, visualization, validation, data curation. Shengyou Wang: Investigation, project administration, resources, supervision, validation, writing - review and editing. Jialiu Fang: Research design, investigation, project administration, resources, supervision, validation, writing - review and editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of Anhui Medical University (No. 2023xkj105).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.