
Abstract
HER2-mutated non-small lung cancer (NSCLC) in China represents a substantial patient population characterized by an unfavorable prognosis. However, at present, the main clinical treatment options are relatively limited. HER2 mutations in Chinese NSCLC (2019-2024) demonstrated 3.8%-5.6% prevalence via NGS, exceeding global baselines, with superior detection vs PCR (4.5% vs 3.1%). In addition, more attention was paid to molecular analysis and the detection rate of HER2 genomic alterations in NSCLC patients in eastern and northern China compared to other parts of China, which might be related to regional economic differences and geographic differences in lung cancer epidemiology. The evolving therapeutic landscape has established new-generation TKIs (pyrotinib) and antibody-drug conjugates (ADCs) like trastuzumab deruxtecan (T-Dxd) as targeted strategies for HER2-mutant NSCLC. Despite late research initiation, China rapidly advanced from retrospective analyses to pioneering new drug trials. In general, the incidence of HER2-mutated NSCLC in the Chinese population seems to be higher than the world average, and there is a large number of missed HER2-mutated NSCLC patients in China. In this field, ADCs and novel TKIs are being developed and researched in spurts, and new drugs are moving from back-line therapy to front-line therapy, and from single-drug regimens to combination regimens.
Introduction
Non-small lung cancer (NSCLC) is a heterogeneous disease, which accounts for approximately 85% of total lung cancer cases globally, 1 and the 5-year survival rate for advanced NSCLC is less than 10%. 2 Platinum-based chemotherapy has been the standard therapeutic method for a long time. 3 Currently, with the unstopped exploration for the molecular mechanism of lung cancer, driver genes with therapeutic value have been continuously studied, and targeted drugs and immune checkpoint inhibitors have made a rapid breakthrough. 4 NSCLC patients with positive driver genes (EGFR, ALK, ROS1, etc.) have longer survival and better prognosis.
In recent years, HER2 alterations have been a hot topic and a great challenge in lung cancer treatment, and HER2 mutation is the main type. 5 Before the era of targeted therapy, chemotherapy has been the standard treatment for lung cancer patients with HER2 mutation. However, clinical outcomes with first-line chemotherapy monotherapy in this population demonstrated inferior efficacy compared to NSCLC patients harboring other driver mutations such as ALK/ROS1 rearrangements (PFS: 5.1 vs 9.2 months). 6 With the emergence of precision treatment, a variety of new anti-tumor drugs have been developed, including classic tyrosine kinase inhibitors (TKIs), new-generation TKIs, and antibody-drug conjugates (ADCs), which has made the landscape of HER2-targeted therapies increasingly complex. A pivotal milestone in 2024 was achieved with the FDA (Food and Drug Administration) approval of the ADC trastuzumab deruxtecan (T-Dxd) for HER2-mutant NSCLC. This breakthrough therapeutic agent subsequently gained distinction as China’s first ADC approved in lung cancer, while demonstrating unprecedented clinical efficacy paired with a manageable safety profile. In China, the incidence of HER2 mutations is higher than the global average, and the living habits, economic conditions, and environmental factors differ significantly from those in Europe and the United States. Therefore, it’s particularly important to study the treatment progress of HER2 mutations in China. We review the epidemiologic characteristics, pathogenic mechanisms, clinicopathological features, and current therapeutic drugs of HER2 mutations in NSCLC in the world, especially in China.
Epidemiologic Characteristics of HER2 Mutations
HER2 alterations were first found in patients with breast cancer, and subsequent studies have shown that it is widely present in various types of tumors such as stomach, lung, pancreatic and kidney cancers. HER2 alterations are considered a rare molecular subtype in NSCLC, which include HER2 mutations, HER2 amplification, and HER2 overexpression. 5
Frequency of HER2 Mutations for Studies by Different Regions of China.

Biological Functions, Pathogenic Mechanisms, Diagnostic Methods, and Clinicopathological Features of HER2 Mutations
The human epidermal growth factor receptor (HER) family, also called the Erb-B family of type I receptor tyrosine kinases, has four members, including ErbB1/EGFR/HER1, ErbB2/HER2, ErbB3/HER3 and ErbB4/HER4. 11 All receptors contain three domains, 12 including an extracellular domain (ECD), a transmembrane domain (TMD), and an intracellular tyrosine kinase domain (TKD). After ligands bind to HER receptors, homodimer or heterodimer and autophosphorylation are increased, thus triggering a variety of downstream signaling pathways related to proliferation, differentiation, and apoptosis, such as mitogen-activated protein kinase (MAPK), 13 phospholipid inositol 3-kinase (PI3K)/ protein kinase B (AKT), 14 protein kinase C (PKC), 15 and signal transducer and activator of transcription (STAT), 16 which have been demonstrated in preclinical models.17-19 However, unlike the other three receptors, HER2 has no direct ligands and acts primarily as a co-receptor to participate in dimer formation and thus downstream signal transduction. 20
The 2024 National Comprehensive Cancer Network (NCCN) recommends testing for HER2 mutations in all patients with advanced or metastatic NSCLC,
21
and currently the most common methods for testing HER2 mutations are NGS and ARMS-PCR. Our analysis of 61 840 Chinese NSCLC patients who had undergone genetic testing showed (Figure 1A) that NGS yielded a higher rate of HER2 mutation detection than PCR (4.5% vs 3.1%). In addition, our findings demonstrated that compared with other regions in China, the eastern and northern regions of China pay more attention to molecular profiling of NSCLC patients and detection rates of HER2 genomic alterations, which may be related to regional economic disparities coupled with geographical variations in lung cancer epidemiology (Table 1). At present, only 50% of Chinese NSCLC patients accepted the testing for HER2 mutation, and about 60% of those were detected by PCR (Data from IQVIA investigation report 2023 and 3rd party IVD providers). However, compared to PCR, NGS has a relatively wider spectrum, which means comprehensively covering the coding sequence and identifying known or unknown variant types. This indicates that there are still a large number of undetected NSCLC patients with HER2 mutation in China, posing a challenge for clinical work. In 2023, the first clinical diagnosis and treatment expert consensus of HER2-altered NSCLC in China preferentially recommended NGS for mutation detection and strongly recommended tumor tissue samples as detection objects.
22
Liquid specimens such as blood and cytological specimens such as pleural effusion were also recommended when tumor specimens were not available. (A) Frequency of HER2 Mutations Detected by Different Assays in China. (B) Distribution Patterns of HER2 Mutation Sites in American and Chinese Populations. (C) Current Drugs for HER2- Mutated NSCLC.
HER2 mutations can occur in three domains and exon 20 insertions in TKD are the dominant forms. 23 HER2 mutations drive oncogenesis and tumor progression through structural and functional alterations of the HER2 protein. Different mutation types of HER2 have distinct pathogenic mechanisms. Studies24-26 reveal that previous studies have shown that intracellular TKD alterations, such as the Y772_A775dupYVMA mutation, can enhance HER2 kinase activity, thereby activating downstream signaling pathways. In contrast, mutations occurring in the ECD, like S310F/Y mutation, make the HER2 protein more prone to form homodimers or heterodimers, thus activating signaling pathways. In lung cancer, HER2 mutations often occur in the kinase domain, specifically the TKD. This abnormal HER2 pathway is unique to lung cancer because mutations in the HER2 kinase domain are relatively rare in other types of tumors, 9 such as breast cancer (4.3%), gastric cancer (5.0%), and colorectal cancer (2.9%), indicating tissue-dependent carcinogenic mechanisms. According to a large retrospective study, 27 the distribution pattern of mutation sites in Chinese and American populations is similar, with Y772_A775dupYVMA subtype occurring most frequently, followed by G776delinsVC/LC/VV and S310F/Y subtype (Figure 1B). In addition, HER2 mutations in NSCLC are often considered mutually exclusive with other driver gene mutations, and the most common co-mutation is the TP53 mutation, followed by mutations in the PI3K/AKT/mTOR pathway. 28 Studies 29 indicated that NSCLC with HER2-TP53 co-mutations tended to respond less well to targeted therapy and are more likely to brain metastases. Changes in the domain lead to conformational changes in the ATP-binding pocket, which enhance signaling and limit the binding of drugs, thereby reducing drug activity. 30 Therefore, some traditional targeted drugs cannot meet the needs of patients with HER2 mutations. In the following, we review the emerging HER2-mutated NSCLC drugs (Figure 1C) and summarize some problems in the clinical application of this field in China.
Progress and Confusion in the Treatment of HER2-Mutated NSCLC
Chemotherapy and Monoclonal Antibodies
Before the era of targeted therapy, chemotherapy as the main treatment has dominated the field of anti-tumor therapy for decades, but HER2-mutated NSCLC patients are insensitive to chemotherapy. Several studies revealed that HER2 gene copy number had no association with response to first-line chemotherapy in NSCLC. 31 A retrospective study 32 from a European center reported that the overall response rate (ORR) and median progression-free survival (PFS) of conventional chemotherapy in HER2-mutated NSCLC patients were 43.5% and 6 months for first-line treatment. In recent years, a series of retrospective studies6,33-37 in China have shown that patients with first-line chemotherapy had ORR of 11.5%-36.0% and PFS of only 4.3-5.9 months, suggesting that the response of the Asian NSCLC population with HER2 mutation to first-line chemotherapy might be slightly lower than that of European and American populations. However, some studies33,36 also reported that chemotherapy shows similar or even higher activity than HER2-targeted TKIs. Chemotherapy is far from meeting the therapeutic needs of HER2-mutated NSCLC patients, and traditional TKIs have failed to improve the effect. Therefore, new strategies and drugs for HER2-mutated NSCLC patients are urgently needed to change the current treatment pattern.
Trastuzumab can block dimer formation and inhibit downstream signal transduction by binding to HER2 ECD, thereby being used to treat breast cancer and gastric cancer with HER2 overexpression. Disappointingly, the ORR of HER2-positive NSCLC patients treated with trastuzumab monotherapy was almost 0. 38 Ghosh R et al 39 pointed out that it could not prevent the formation of ligand-induced heterodimers such as EGFR/HER2 or HER2/HER3, and therefore could not achieve complete interruption of HER2 signaling. Pertuzumab can block the formation of heterodimers, and its combination with trastuzumab can provide a complete HER2 signaling blockchain. 40 Therefore, a European prospective study 41 in 2022 combined trastuzumab, docetaxel, and pertuzumab, also a HER2 monoclonal antibody, into a triple therapy regimen. The ORR and mPFS were 29% and 6.8 months, and the effect of the regimen appeared to be better than that of a single monoclonal antibody or chemotherapy. However, the regimen still needs further clinical validation. We haven’t seen any clinical studies of HER2 monoclonal antibody alone or in combination in the Chinese population with HER2-mutated NSCLC so far.
Immune Checkpoint Inhibitors (ICIs)
ICIs combination therapy has been recommended as the preferred treatment for advanced NSCLC patients with HER2 mutation. 21 However, this rare mutation often presents with a relatively low PD-L1 positive expression rate and tumor mutational burden, 42 which may contribute to poor response to ICI monotherapy. International retrospective studies43,44 showed that the effect of ICIs alone or in combination in the treatment of HER2-mutated NSCLC was not impressive. A retrospective study 44 from France showed that patients treated with ICI monotherapy had an ORR of 27.3% and mPFS of 2.2 months. However, a study 45 based on the Cancer Genome Atlas of the Chinese Population suggested that HER2 mutations might change the tumor microenvironment to support immunotherapy and that the ORR of the HER2 mutated NSCLC patients was higher than that of the wild type in 321 patients treated with ICIs (44.4% vs 25.7%). Recently, a large real-world retrospective study 46 (CHAPTER Study) included 309 Chinese NSCLC patients with HER2 mutations, among which the first-line patients receiving chemotherapy combined with ICIs had mPFS of 9 months, which was higher than chemotherapy alone and chemotherapy combined with bevacizumab. These findings suggest that ICI monotherapy has limited efficacy in patients with HER2-mutated NSCLC, but for Chinese patients, first-line treatment with chemotherapy combined with ICIs can significantly extend survival. As the first-line therapy for Chinese NSCLC patients with negative driver genes, although the therapeutic accuracy of the combination regimen is relatively lower than that of targeted therapy, the efficacy of this regimen in HER2-mutated NSCLC patients is still worthy of recognition.
Tyrosine Kinase Inhibitors (TKIs)
HER2 mainly relies on other receptors in the HER family to play a carcinogenic role. TKIs are drugs that specifically target tyrosine kinase domains. By binding to the TKD of HER2 or other HER receptors, these agents effectively block downstream signal transmission, thereby inhibiting tumor occurrence, proliferation, and metastasis. They were widely used for the treatment of HER2-mutated NSCLC before the advent of antibody-conjugated drugs (ADCs).
First-Generation Non-Selective TKIs
Afatinib was first used in NSCLC with EGFR mutations, 47 while its efficacy in patients with HER2 mutations was frustrating. 36 In European and American countries, the ORR of Afatinib monotherapy for HER2-mutated NSCLC ranges from 7.7% to 40%. 48 A large retrospective study 49 on the Chinese population suggested that the ORR of NSCLC patients with HER2 mutations treated with afatinib monotherapy was only 17%, and the PFS was only 2.6 months, far less effective than chemotherapy. Therefore, Afatinib was not routinely recommended as a targeted drug for patients with HER2-mutated NSCLC. Dacomitinib is a pan-HER irreversible TKI, primarily used in the first-line treatment for locally advanced or metastatic NSCLC with EGFR mutations. 50 A cohort study 51 revealed that mPFS was only 3 months after treated with Dacomitinib. The performance of Neratinib in clinical studies was similarly disappointing, with an ORR of only 3.8% for monotherapy. 52 The performance of irreversible TKIs can be described as dire in the treatment of HER2-mutated NSCLC, and some studies suggested that it might be related to the narrowing of the drug binding pocket, therefore TKIs with novel structure were subsequently developed.
Second-Generation Selective TKIs
Poziotinib has a smaller size and more flexible drug structure, which can better bind to the domain. A phase Ⅱ trial 53 showed that patients treated with poziotinib had an ORR of 27%, but TRAEs were present in 97% of patients. Although poziotinib has shown efficacy in patients with HER2-mutated NSCLC, its safety concerns have limited its clinical use and subsequent development. Exploring suitable combination therapy for poziotinib may be the direction to break the situation.
Pyrotinib, an orally available small-molecule irreversible tyrosine kinase inhibitor (TKI) targeting HER2 developed in China, 54 received approval from the National Medical Products Administration (NMPA) in 2018 for use in combination with capecitabine to treat chemotherapy-pretreated HER2-positive breast cancer. 55 Recently, its therapeutic potential has been evaluated in multiple clinical trials involving HER2-mutant NSCLC patients. The efficacy of pyrotinib in the European and American populations was not outstanding, with results from a Phase I basket trial 56 showing that pyrotinib monotherapy in patients with HER2 mutated NSCLC who had previously received other treatments had an ORR of only 19% and mPFS of 5.4 months. However, it has shown promising clinical activity in the treatment of the Chinese population. A meta-analysis 57 showed that ORR was as high as 35% in Chinese patients treated with pyrotinib monotherapy after previous chemotherapy failure. Subsequently, a large retrospective study 35 in China demonstrated that patients who had failed first-line therapy could benefit more from pyrotinib. Although pyrotinib has a probability of causing grade 3 or higher diarrhea, 58 prophylactic drugs or its combination with other agents such as thalidomide 59 or loperamide 60 may reduce the incidence of pyrotinib-associated diarrhea, and decrease the incidence of discontinuation or reduction.
New Generation Small Molecule TKIs
BAY 2927088 is an oral reversible TKI. The SOHO-01 trial 61 observed that the ORR and mPFS were up to 72.1% and 7.5 months in the dose-increment/compensation portion, respectively, and AEs (grade ≥ 3) were reported in 43.2% of the patients. As a result, the drug received breakthrough therapy designation from the FDA in 2024.
Zongertinib (BI1810631) is also an oral TKI. Currently, the Beamion LUNG-1 Phase Ib trial 62 indicated that ORR in the zongertinib 120 mg/day cohort was as high as 71%, and TRAEs (grade ≥ 3) was only 17%. No treatment-associated interstitial lung disease (ILD) has been observed. More than 50% of the trial population was Asian. The drug received breakthrough therapy designation from the FDA and the CDE in 2024 for the treatment of adults with advanced NSCLC who had an active HER2 mutation and have previously received systemic therapy.
Other TKIs such as tarloxotinib and mobocertinib are also in clinical studies. The new generation of TKIs show higher activity than the previous generation, while the safety problems also deserve researchers to consider how to improve the structure and strengthen clinical management to overcome toxicity. The development and application of TKIs in the field of HER2 mutant NSCLC is still a blue ocean.
Antibody-Drug Conjugate (ADC)
ADCs are anti-tumor drugs that pair specific monoclonal antibodies with effective cytotoxic payload, 63 and have the characteristics of high selectivity, high efficiency, and high safety compared with traditional drugs. 64 Its mechanisms include recognizing and binding to the ECD of tumor-specific transmembrane proteins, internalizing ADC-protein complexes by the endocytosis pathway, and releasing cytotoxic payloads that ultimately kill malignant cells. 65 Preclinical studies66,67 have shown that HER2 mutations could promote receptor internalization and intracellular uptake of the HER2 receptor-ADC complex. After the successful treatment of breast and gastric cancer, the application of ADC in HER2-mutated NSCLC is gradually receiving attention.
Trastuzumab Emtansine (T-DM1)
T-DM1 is an anti-HER2 ADC composed of trastuzumab and Emtansine (DM1) which is an inhibitor of microtubule aggregation. 68 The efficacy of T-DM1 in European and American populations is inconsistent. A Phase II basket trial 69 suggested the clinical activity of ADC in this type of patient, which reported a partial response rate of 44% and mPFS of 5.0 months for T-DM1 in patients with HER2-mutated NSCLC who had previously received systemic therapy. However, a retrospective study 70 in 2022 showed that the ORR of T-DM1 monotherapy was 0%, possibly due to the small sample size. No clinical trial results of T-DM1 in the Chinese HER2 mutant NSCLC population have been found so far. In conclusion, more studies are needed to evaluate the efficacy of T-DM1 in patients with HER2-mutated NSCLC.
Trastuzumab Deruxtecan (T-Dxd, also Known as DS-8201a)
T-Dxd consists of trastuzumab, a novel topoisomerase I inhibitor (Dxd), and an enzymable peptide chain. 71 Its mechanism is similar to T-DM1, however, T-Dxd has a higher drug antibody ratio (8 vs 3.5) and a bystander effect, which can kill low-expression HER2 or even HER2-negative cancer cells near the target cell. 72 The highly stable linker and load ensure the blood drug concentration, thus reducing adverse reactions. 73
Efficacy of T-Dxd and Pyrotinib in Patients With HER2-Mutated NSCLC.
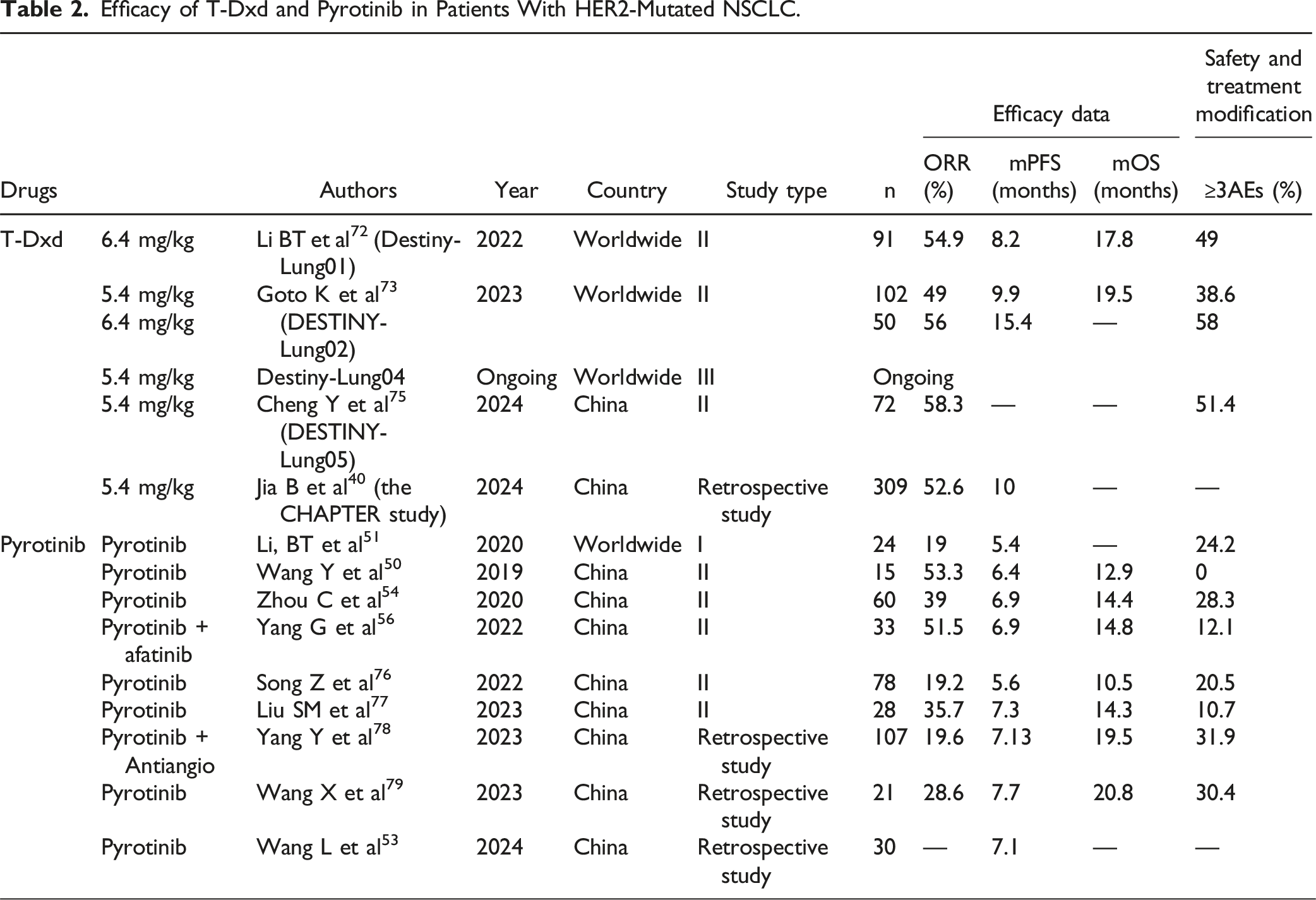
Although both trials included the Asian population, the DL01 and DL02 trials did not separately analyze the reactivity of T-Dxd in Chinese. As a bridging study of DESTINY-Lung02, the DESTINY-Lung05 82 evaluated the efficacy and safety of T-Dxd in Chinese patients with advanced NSCLC with HER2 mutation who had previously received treatment. The dose was 5.4 mg/kg, and a total of 72 patients were enrolled, with an ORR of 58.3%. The mPFS assessed by the investigators was 10.8 months. In terms of safety, the incidence of TRAEs (grade ≥ 3) in the trial was 51.4%, the probability of discontinuation or reduction was 22.2%, and the incidence of ADC-associated ILD was 9.7%. The efficacy and safety of the DESTINY-Lung05 were not found to be significantly different from those of the DESTINY-Lung02, which further supported the benefit of T-Dxd in HER2-mutated NSCLC and provided new evidence for its application in Chinese. In October 2024, T-DXd received regulatory approval from NMPA for treating unresectable locally advanced or metastatic NSCLC harboring HER2 mutations in adults with prior systemic therapy exposure. The CHAPTER study, the first real-world study of T-Dxd in HER2-mutated NSCLC, showed that patients treated with T-Dxd on second-line therapy had a mPFS of 10 months, which was longer than other anti-HER2 regiments, and for all patients treated with posterior line therapy, T-Dxd had an ORR of 52.6% and mPFS of 8 months. This study confirms from a real-world perspective that T-Dxd can be the preferred treatment for advanced NSCLC patients with HER2 mutation on second-line therapy in China. At the same time, the scope of research is also expanding, and a first-line trial comparing T-Dxd monotherapy with chemotherapy plus pembrolizumab in patients with HER2-mutated NSCLC (DESTINY-Lung04) is underway, and we expect the results to provide strong evidence for T-Dxd as first-line treatment options.
SHR-A1811
SHR-A1811 is a novel ADC developed in China that connects Trastuzumab with DNA topoisomerase I inhibitor (SHR169265) via a cleavable tetrapeptide-based linker.83,84 The most recent Phase 1/2 study 85 in the Chinese population of HER2-mutated NSCLC reported the ORR was 41.9% and mPFS was up to 8.4 months long in the 4.8 mg/kg cohort, but 46% of patients had TRAEs (grade ≥ 3). Although SHR-A1811 demonstrated good activity in clinical trials, it is still necessary to adjust the safe dose and monitor the occurrence of AEs.
GQ1005
GQ1005 is also a new type of ADC developed in China. Its payload drugs and antibodies are highly similar to T-Dxd, but it adopts a unique enzymatic fixed-point coupling technology and has a stable open-loop linker, which greatly improves the stability of the drug and achieves a balance between efficacy and safety. Preclinical studies have shown that GQ1005 exhibited antitumor effects comparable to T-Dxd in a variety of tumor models, with no obvious toxicity and a higher therapeutic index. In the FIH study of GQ1005 led by Chinese scholars, 86 the ORR and mPFS were 20.0% and 7.2 months in patients with HER2 mutations, and the incidence of TRAE was 14%. More data are still being studied.
BB-1701
BB-1701 is also a new type of ADC independently developed by China, which is connected by monoclonal antibodies against HER2 and eribulin through a valine-citrulline connector, and has also entered the clinical trial stage. At the 2024 ESMO meeting, the results of the Phase II clinical trial of BB-1701 led by Chinese scholars in the treatment of HER2-mutated/amplified NSCLC were partially presented, and the ORR was 41.7%. 87 More data are still under study.
In addition, there are many ADCs for HER2-mutant NSCLC that are in the trial stage and have not published results, such as TQB2102, GQ1001, JSKN003, etc. The research of ADC drugs in the treatment of HER2-mutated NSCLC has made rapid progress, and a large number of clinical trials of Chinese-developed ADCs targeting the Chinese population are carried out. However, we currently lack a universal biomarker that can predict the therapeutic response and toxicity of ADCs because of few clinical trials. Although the efficacy of ADCs is better than that of history, the mechanism of drug resistance of ADCs and the choice of follow-up treatment are still worthy of further consideration. In addition, since NSCLC patients with HER2 mutations are more likely to develop brain metastasis, and the survival of patients with brain metastasis is significantly shorter than that of patients without brain metastasis, subsequent clinical trials still need to design a specific endpoint and regularly monitor intracranial activity and central nervous system imaging. Currently, results of ADCs have shown high ORR and unsatisfactory mPFS. Further improving the structural design of ADCs to optimize anti-tumor activity and minimize toxicity may be a potential strategy to achieve a breakthrough in the treatment of HER2-mutated NSCLC.
Exploration and Research of HER2-Mutated NSCLC in China
Studies on HER2 mutant NSCLC started late in China. Unlike other countries, the research on HER2-altered NSCLC in China was first carried out in 2004, while the focus on the diagnosis and treatment of HER2-mutated NSCLC patients in China began after 2010 (Figure 2). Before this, the treatment of relevant domestic patients was referred to the treatment protocols of foreign patients with HER2 mutant NSCLC. In 2014, Feng SD et al
88
retrospectively evaluated a large cross-sectional cohort of NSCLC patients and noted that HER2 mutations are uncommon in Chinese NSCLC patients. Subsequently, a retrospective study
89
supplemented the clinicopathological features of the Chinese HER2-mutated NSCLC population, noting that Chinese patients in the HER2-insertion group were significantly associated with never smoking, female, adenocarcinoma, and under 60 years of age. The Progression of International and Chinese Research on the Treatment of HER2-Mutuated NSCLC.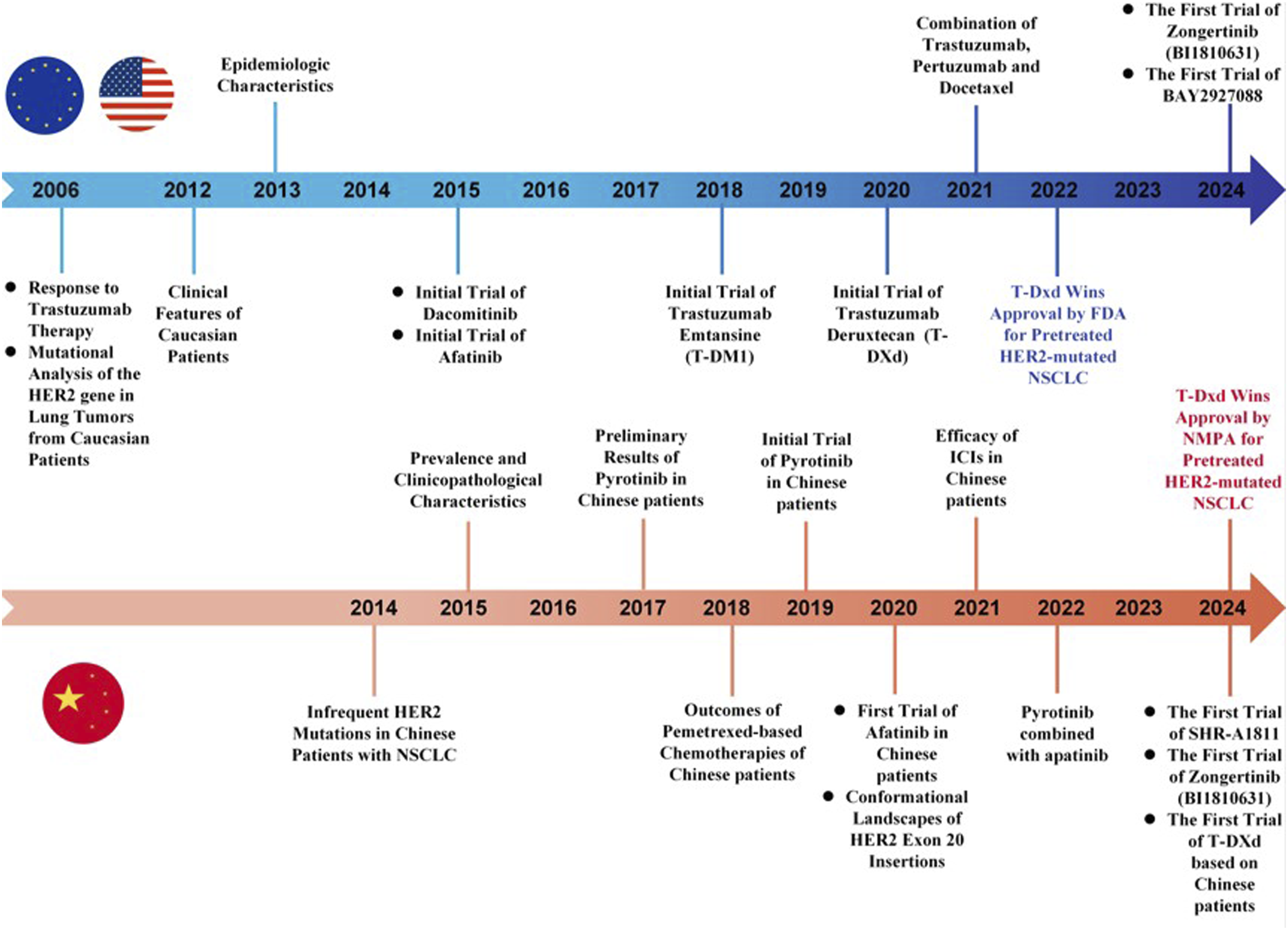
After 2017, researchers in China began to systematically study the response of HER2-mutated NSCLC patients to chemotherapy and TKIs represented by afatinib and pyrotinib. Studies revealed that HER2-mutant NSCLC demonstrated reduced chemosensitivity relative to other oncogene-driven NSCLC subtypes, while TKIs such as afatinib and osimertinib paradoxically exhibited inferior clinical outcomes compared to conventional chemotherapy regimens. Therefore, Chinese scholars conducted genomic analysis 78 on Chinese lung cancer patients with HER2 mutations to explain the molecular dynamics of drug resistance. YVMA insertion induced spatial binding disorder and formed steric hindrance to afatinib binding, but pyrotinib was not affected by this. Multiple prospective and retrospective studies35,54,58,76,77,79,90,91 from 2019 to 2024 have shown that pyrotinib in Chinese patients with HER2-mutated NSCLC had an ORR of 19.2%-53.3% and mPFS of 5.6-7.7 months. The incidence of TRAEs (grade≥ 3) was 0%-30.4% (Table 2). Moreover, data from several combination treatments showed that pyrotinib combined with anti-angiogenic therapy could not improve the efficacy. Although pyrotinib combined with Afatinib could improve the ORR, the survival of patients did not show significant prolongation.
Efficacy of ICIs-Based Combination Therapy in Chinese HER2-Mutated NSCLC Patients From 2019 to 2024.

The therapeutic landscape of HER2-mutant NSCLC is garnering increasing attention, but critical knowledge gaps persist. Emerging priorities include systematic retrospective analysis of existing therapies, clinical exploration of next-generation agents (ADCs, bispecific antibodies, and novel TKIs), and mechanistic investigations into resistance patterns and toxicity profiles that constrain therapeutic windows. Notably, Chinese populations exhibit distinct therapeutic responses to regimens such as chemoimmunotherapy, suggesting unique molecular characteristics of HER2 variants in this demographic. However, comprehensive epidemiological profiling remains lacking, with insufficient documentation of mutation subtypes and sites, necessitating large-scale population studies. Furthermore, the heterogeneous oncogenic mechanisms across HER2 mutation sites demand rigorous evaluation of potential site-specific therapeutic vulnerabilities. Pharmacokinetic/pharmacodynamic (PK/PD) profiling of anti-HER2 agents, particularly novel compounds, is imperative given their divergent efficacy/safety profiles. Additionally, the high incidence of CNS metastases warrants both mechanistic studies on blood-brain barrier interactions and implementation of standardized neurocognitive surveillance protocols. While monotherapies demonstrate preliminary efficacy, strategic combinatorial approaches with anti-angiogenics, HER2-targeted antibodies, or cytotoxic agents may unlock synergistic clinical benefits, underscoring the need for trials evaluating therapeutic synergism.
Conclusions and Future Perspectives
Epidemiological data indicates that the incidence of HER2-mutated NSCLC in the Chinese population is higher than the world average level, and there are a large number of undetected HER2-mutated NSCLC population in China because the current detection methods of HER2 mutation have not been well-popularized and improved. In summarizing therapeutic drugs, we analyzed the results of clinical trials and discovered that HER2-mutated NSCLC patients in the Chinese population had a poor response to chemotherapy alone. However, they showed a significant benefit from combination therapy involving chemotherapy. This may be related to the higher positive rate of PD-L1 expression, more stable genome, and fewer genetic changes in the Chinese NSCLC population. In addition, we found that the therapeutic effect of ADCs was significantly higher than that of TKIs, which may be related to the wider targeting range of ADCs. Although the research on HER2 mutant NSCLC in China started late, the research progress is fast. The development of treatment for HER2-mutated NSCLC in China is from early studies on mutation frequency and clinicopathological features of Chinese patients to prospective or retrospective studies on the efficacy of various treatments such as pyrotinib, chemotherapy, and chemotherapeutic immunotherapy. At present, we are actively developing and carrying out clinical trials of new drugs such as T-Dxd, SHR-A1811, and BB-1701 in the Chinese population.
Traditional chemotherapy cannot bring greater survival benefits to Chinese NSCLC patients with HER2 mutation, and traditional TKIs and ICI monotherapy cannot meet the needs of these people for survival benefits. A new generation of highly selective and small-structure drugs may be a new choice. New TKIs, especially zongertinib, have shown higher activity and a well-controlled safety profile. We look forward to publishing more data on zongertinib in the future. ADCs represented by T-Dxd are revitalized in the field of NSCLC treatment, and the survival data of the Chinese population is also very impressive. In general, in the field of HER2-mutated NSCLC treatment, ADC drugs and novel TKIs are being developed and researched in spurts, and new drugs are moving from back-line therapy to front-line therapy, from single-drug regimen to combination regimen. In short, we look forward to the publication of more research data in China in the future, to further improve the benefits of Chinese NSCLC patients with HER2 mutation, and to provide more accurate, efficient, safe, and personalized treatment strategies for the clinic.
Footnotes
Ethical Statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
Data are available upon reasonable request. The data supporting this study’s findings are available from the corresponding author upon reasonable request. All data generated or analyzed during this study are included in this published article.