
Abstract
Objective
To investigate the risk factors for complications in breast cancer patients with totally implantable access ports (TIAPs).
Methods
This retrospective case-control study involved 471 breast cancer (BC) patients who received TIAPs during chemotherapy. We compared the demographic and clinical characteristics of patients with complications to those without, analyzed independent risk factors using binary logistic regression, and identified differences in complication rates based on catheterization site.
Results
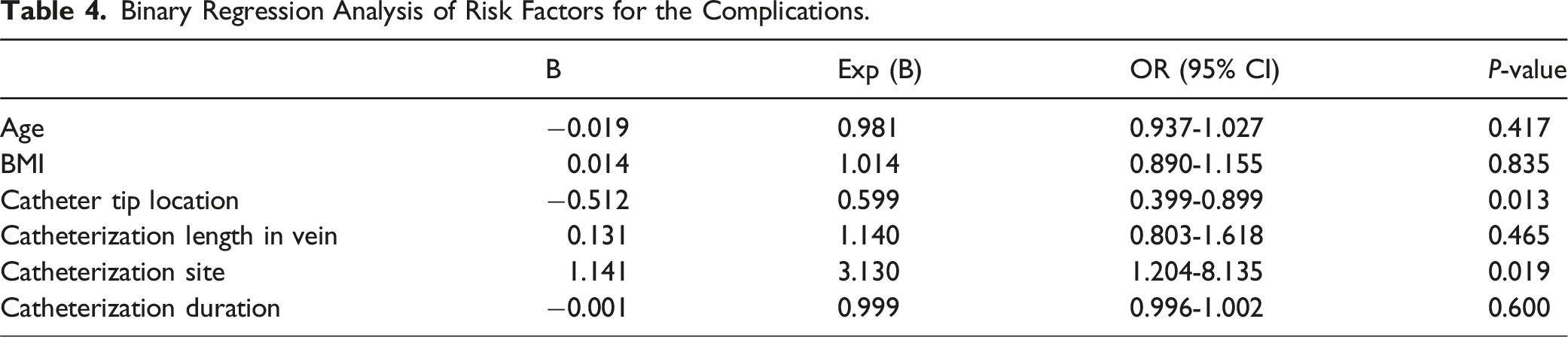
The most frequent complication was catheter malposition, followed by infection, thrombosis, hemothorax, and port rotation. Complications were more common in right-side BC cases (P = .026) and with left-side insertions (P = .012). Binary logistic regression identified independent risk factors for complications: catheter tip location (OR = 0.599, P = .013), and catheterization site (OR = 0.319, P = .019). Notably, left-side insertion significantly increased the risk of overall complications and catheter malposition compared to right-side insertion (OR = 3.534, P = .008; OR = 5.624, P = .004, respectively).
Conclusion
Catheter tip location and catheterization site independently affect complications and catheter malposition. For TIAPs implantation, particularly on the left side, a lower catheter tip location is advised to reduce complications and enhance safety.
Introduction
Breast cancer (BC) remains the most prevalent and the second lethal malignancies for women. 1 Today’s BC treatment involves a series of complex and systemic strategies. 2 Chemotherapy is a key component of systemic treatment for BC patients and significantly reduces the risk of recurrence.2-4 In recent clinical practice, the use of totally implantable access ports (TIAPs) offers a less invasive and more reliable method for administering chemotherapeutic agents via a central venous route. 5 Furthermore, compared to alternative methods such as peripherally inserted central catheters (PICCs) or temporary internal jugular vein catheters, TIAPs demonstrate superior performance in the long-term treatment and management of patients with solid tumors, 6 particularly those, including BC patients, who undergo chemotherapy for durations exceeding 6 months.7-9
TIAP complications include early issues during port implantation, such as catheter malposition, hemothorax, pneumothorax, arterial puncture, and bleeding, as well as late complications like infection, thrombosis, catheter rupture, and port rotation.10,11 Previous studies have reported TIAP complication rates in oncology patients ranging from 1.8% to 30.2%12,13 with studies specific to BC reporting rates of 10.2%.7,8 Notably, while several studies suggest that TIAP complications are unrelated to tumor type, those with a higher proportion of BC patients report higher complication rates (16.1% 14 and 22.4% 15 ) compared to studies with fewer BC patients (4.8% 13 and 8.3% 16 ). However, based on our clinical experience, we have not observed a high rate of TIAP complications in BC patients, and the main complication (about 75%) was concentrated on catheter malposition. Consistent with our findings, a study reported a catheter malposition rate of merely 1.06% associated with TIAP among 1504 BC patients, although it did not consider other complications. 17 Similarly, a randomized trial involving 27 BC patients assigned to the TIAP group over a 2-year period identified only one instance of infectious complication. 18
In addition, most research has examined the safety, cost, and patient satisfaction of TIAPs,5,6,16,19 with limited attention given to complication risk factors in BC patients. Besides the uncertainty surrounding the actual complication rate, a notable issue is the scarcity of guidelines for managing TIAP complications in oncology, including breast cancer. This study retrospectively analyzed 3 years of medical records of BC patients with TIAPs during chemotherapy at our center to assess complication risk factors, validate our findings, compare with past research, and improve clinical practice.
Materials and Methods
Study Population
Clinical and follow-up data were collected from 476 BC patients who received implantation of totally implantable access ports (MEDCOMP® CT Implantable Port) for chemotherapy between March 2016 and March 2019 in the Department of Breast Surgery, Women’s Hospital, Zhejiang University School of Medicine. The inclusion criteria for this study were patients with BC who required TIAP chemotherapy at our hospital. A total of five patients were excluded due to missing data or loss to follow-up. Ultimately, 471 patients were included in the study. The studies involving human participants were reviewed and approved by the Research Ethics Board of Women’s Hospital, Zhejiang University School of Medicine (IRB-20190043). Informed consent was waived from the board as this was a retrospective chart review.
TIAP Implantation and Complication Management
Experienced doctors performed the TIAP implantation following a multidisciplinary consensus. 20 The surgical site was prepared, and local anesthesia was administered. A 0.5 cm incision was made to puncture the internal jugular vein under ultrasound guidance. A guide wire and catheter sheath were then inserted. A 2.0-2.5 cm incision was made to create a pocket for the port, and a tunnel was formed leading to the puncture site. The catheter was adjusted and inserted into the vein, with blood aspiration and saline injection confirming its patency. The tube was sealed with heparin saline, and a chest X-ray was taken to verify the position of the catheter tip.
Manual reduction was preferred for port rotation, with surgical intervention available as a backup. Antibiotics were used to treat port infections, with removal necessary in severe cases. Hemothorax was managed with thoracentesis and drainage, while anticoagulants were administered for thrombosis, with the port removed once the thrombus stabilized.
Clinical Parameters and Complications
All pertinent clinical and TIAP parameters, such as age, height, weight, body mass index (BMI), breast cancer location, neoadjuvant chemotherapy, catheterization site, catheterization length within the vein, duration, and catheter tip location, were extracted from the medical records database. Subsequently, five early or late complications—catheter malposition, infection, thrombosis, hemothorax, and port rotation—were observed and analyzed to identify the associated risk factors.
All parameter choices were based on the literature7,8,12-16 and our clinical experience. The diagnosis and management of early and late complications fully adhered to existing guidelines, 20 with final follow-up for each patient conducted 3-6 month after the removal of TIAP.
Statistical Analysis
Statistical analyses were conducted utilizing SPSS version 22.0. Continuous variables are expressed as mean ± standard deviation. For measurement data following a normal distribution, the independent sample t-test or one-way ANOVA was employed, whereas non-parametric tests were utilized for data not conforming to a normal distribution. Proportional data were compared using the chi-square test. Variables identified as significant in univariate analyses, along with potential confounding factors, were incorporated into a binary logistic regression model. A stepwise backward elimination method was applied within the binary logistic regression framework. Statistical significance was determined at a two-sided P-value threshold of <.05.
Results
Baseline Information
A total of 471 patients were included in this analysis, with the majority being female (99.8%) and one patient male (0.2%). The mean age of the participants was 49.79 ± 9.33 years, with a mean height of 158.82 ± 4.71 cm, a mean body weight of 59.09 ± 8.44 kg, and a mean BMI of 23.41 ± 3.07 kg/m2. Of the patients, 229 (48.6%) were diagnosed with left-sided breast cancer, 235 (49.9%) with right-sided breast cancer, and 7 patients (1.5%) had bilateral breast cancer. Fifty-two patients (11.0%) received neoadjuvant chemotherapy, while 419 patients (89.0%) were treated with postoperative chemotherapy.
Baseline Information

Data are presented as mean ± SD unless otherwise specified.
Tip site(T)refers to the level of the thoracic vertebra.
Composition of Complications and Its Relationship With Catheterization Site
In total, 26 complications were observed in 25 patients, comprising catheter malposition in 19 cases, infection in 2 cases, thrombosis in 2 cases, hemothorax in 1 case, and port rotation with co-infection in 1 case (Figure 1A). Among the 19 patients who underwent left-sided catheter insertion, complications included 16 instances of catheter malposition, 2 instances of infection, 1 instance of thrombosis, and 1 instance of hemothorax. In the right-sided catheterization group, complications included 3 cases of catheter malposition, 1 case of thrombosis, and 1 case of port rotation with co-infection. The incidence of complications was significantly higher in the left-sided catheterization group compared to the right-sided group (8.5% vs 2.6%, P = .008, Table 2 and Figure 1B). Catheter malposition was the most prevalent complication, occurring in 19 cases (76.0%), with a significantly higher incidence in the left-sided catheterization group compared to the right-sided group (6.8% vs 1.3%, P = .004, Table 2 and Figure 1B). And as shown in Table 2, left-side insertion significantly increased the risk of overall complications and catheter malposition compared to right-side insertion (OR = 3.534, P = .008; OR = 5.624, P = .004, respectively). Composition of Complications and Its Relationship With Catheterization Site. (A) The Percentage of Cases Based on Five Complications - Catheter Malposition, Infection, Thrombosis, Hemothorax, and Port Rotation (by Different Color Marker) in Left-Side or Right-Side Insertion (by Orange or Grey Marker) Breast Cancer Patients With Complications. (B) Bar Chart Separately Presents the Distribution of Cases for the Complications in Left- and Right-Side Catheterization Group. Complications Proportion in Left-Side and Right-Side Catheterization Group. Inc.: incidence.

Univariate and Binary Logistic Regression Analysis of Risk Factors for the TIAPs Complications in BC Patients
Univariate Analysis of Risk Factors for the Complications.
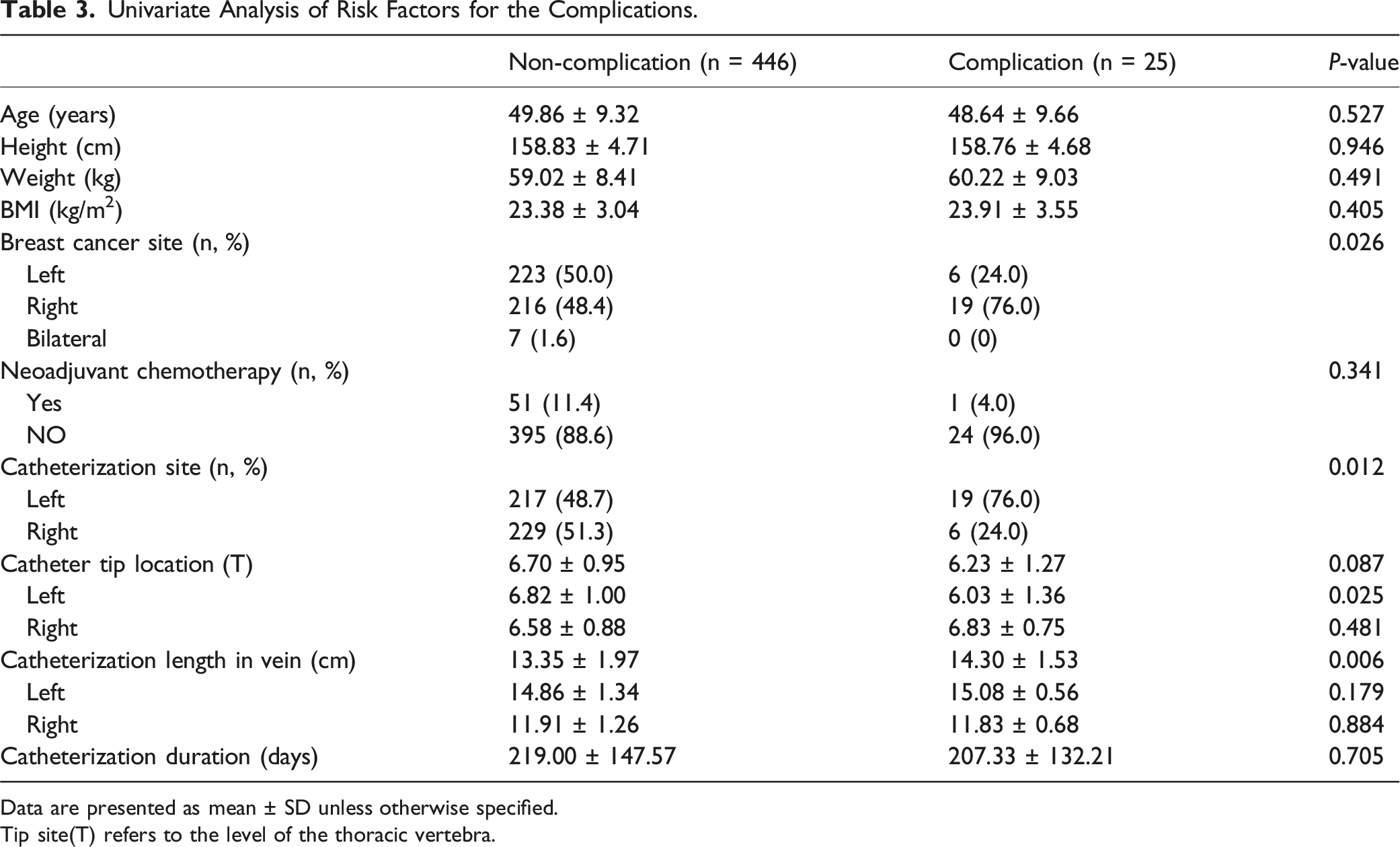
Data are presented as mean ± SD unless otherwise specified.
Tip site(T) refers to the level of the thoracic vertebra.
Binary Regression Analysis of Risk Factors for the Complications.
Discussion
This study identified left-side catheterization and higher catheter tip location as independent risk factors for overall TIAP complications in BC patients. Additionally, left-side insertion was closely associated with catheter malposition. Catheter malposition occurs when the tip is not properly positioned in the superior vena cava, with reported rates between 0.2% and 11.2%.14,21-27 This study found a 4.0% malposition rate overall, with 6.8% for left-sided and 1.3% for right-sided insertions. Limited data exist on malposition rates by insertion site. Schummer et al’s study 28 showed higher left-side misplacement (12%) compared to the right (4.3%), attributing this to anatomical differences: the left internal jugular vein path to the superior vena cava is more complex than the right, involving two curves and additional branches.
Therefore, skilled operation and technical assistance (such as the ultrasound-guided approach) are required when performing puncture procedures on the left internal jugular vein in clinical practice. Hourmozdi et al 26 found that ultrasound-guided TIAPs had a low complication rate, with only one out of 1322 cases resulting in peripheral organ damage (pneumothorax). Ultrasound guidance improves venipuncture accuracy, allowing the catheter to reach the vein’s center, reducing puncture attempts, accidental arterial punctures, and vein penetrations, thus minimizing peripheral organ injury risk. Bademler et al 13 also showed that fewer puncture attempts lead to fewer complications due to ultrasound use. In our study, TIAPs were inserted under ultrasound guidance, yielding an overall complication rate of 5.3%, with only one intraoperative complication (hemothorax), corresponding to a low incidence rate of 0.2%. Furthermore, the procedures were conducted by highly experienced surgeons, which is consistent with the observed low complication rate.
Our study aimed to position the catheter tip between the T5 and T7 vertebrae, with the cavoatrial junction as the ideal location.29,30 Few studies have examined the link between catheter tip position and malposition. Our findings suggest that a higher catheter tip position is an independent risk factor for TIAP-related complications, mainly catheter malposition. This previously unreported insight could improve TIAP safety and success. Possible reasons for this risk include a high puncture point and the natural length of the blood vessel, the latter needing further investigation. What about the catheterization length in the vein? There was a notable difference in catheterization length between the complication and non-complication groups. However, no significant difference was found when analyzing by catheterization site, and logistic regression showed that catheterization length wasn’t an independent risk factor for complications after TIAPs. This is likely due to the complication group having more left-side catheterizations, which require longer lengths. Therefore, we concluded that catheterization length in the vein doesn’t impact the risk of TIAPs-related complications.
In their investigation of infections in patients with tumors post-TIAP implantation, Wang et al 31 identified that individuals with hematological malignancies or head and neck cancers exhibit a heightened risk of infection following TIAP implantation compared to those with other cancer types, with hazard ratios of 4.00 and 4.11, respectively (both P < .001). Using TIAPs for both parenteral nutrition and chemotherapy may also raise infection risk. Our study, which used ports only for chemotherapy and targeted therapy, found a low infection rate of 0.6%. While Hsieh et al 32 linked increased infection risk to age, Ji et al 33 found lower risk in younger patients. However, Ignatov et al 21 and Narducci et al 14 saw no age-related risk. Our study also found no age-related risk, and logistic regression showed age wasn’t a risk factor for complications in BC patients with TIAP. Due to few infection cases, age’s impact on infection remains inconclusive, indicating a need for further research.
Thrombosis is a potential cause of catheter obstruction, with cancer patients being at an elevated risk, particularly during chemotherapy. 34 This study documented two instances of catheter thrombosis in the internal jugular vein; however, chemotherapy was successfully continued with the administration of anticoagulant therapy. Following the completion of treatment, the port was removed, and anticoagulation therapy was briefly maintained. Notably, no intraluminal thrombosis was detected. Moreover, improper positioning of the catheter tip can exacerbate the risk of thrombosis.21,29,30,35 In our clinical practice, repositioning the catheter may compromise the vascular endothelium, thereby increasing the risks of thrombosis and infection. Our findings indicated no significant difference in complication rates between patients with and without catheter malposition. Among the 19 patients with malposition, there was one case of infection and no occurrences of thrombosis. Furthermore, correcting catheter malposition can lead to increased costs and patient discomfort from reoperation, without influencing patient prognosis.
This study has several limitations: (1) Given the relatively low complication rate observed (5.3%, 25/471), further validation of these findings is necessary through future multicenter randomized controlled trials with larger sample sizes; (2) This single-center study, with a small sample size in the complication group, will result in unavoidable statistical biases (such as patient selection, institutional practices, etc.), and the conclusions may not be widely extrapolated until further validation in the future; (4) As a retrospective analysis, the study may have incorporated unmeasured confounding variables; (5)Additionally, certain potential factors, including catheter type, chemotherapy regimen, and duration of surgery, were not considered in this study, which may introduce statistical bias.
Conclusion
In comparison to the non-complication group, the complication group exhibited a higher incidence of right-sided BC cases, more frequent left-side insertions, and elevated catheter tip locations. Both catheter tip location and catheterization site were identified as independent risk factors for overall complications. This conclusion remains consistent even when catheter malposition is analyzed separately. An elevated catheter tip location is correlated with an increased risk of complications associated with TIAPs implantation and catheter malposition, particularly in the left-side catheterization group. Consequently, a lower catheter tip location is preferable, suggesting that when determining the catheter length within the vein, a longer catheter is advantageous over a shorter one. Additionally, greater attention should be given to procedures involving left-side TIAPs implantation.
Footnotes
Acknowledgments
The authors thank for the support of the fund, thanks for the help of everybody in this study.
Statements and Declarations
Author Contributions
All authors contributed to the conception, design, data collection, analysis and drafting of the manuscript; all authors critically reviewed the manuscript and approved the final submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the General Scientific Research Project From Education Department of Zhejiang Province (Y202454712 and Y202455370).
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.