
Abstract
Objectives
This study aims to analyze urinary bladder cancer (UBC) incidence rates in Lebanon over a 12-year period (2005-2016) and compare them with rates in other countries. It also discusses UBC risk factors in Lebanon.
Introduction
Lebanon has one of the highest estimated age-standardized incidence rates (ASIRw) of UBC worldwide.
Methods
Data on UBC were obtained from the Lebanese national cancer registry for the years 2005-2016. The study calculated age-standardized incidence rates (ASIRw) and age-specific rates per 100 000 population. It also estimated the population attributable fractions of smoking, water pollution, and air pollution for UBC incidence in Lebanon in 2016. However, limited data precluded sensitivity analyses, potentially affecting the robustness of the estimates.
Results
During this period, UBC ranked as the third most common cancer in males (12.9% of all new cancer cases) and the eighth most common in females (2.8% of all new cancer cases), excluding non-melanoma skin cancer. The average ASIRw was 28.8 in men and 6.6 in women, placing Lebanon among the countries with the highest UBC incidence rates globally. UBC incidence rates increased with age. Estimates indicated that 46.4% of UBC cases in the Lebanese population were attributed to current smoking, 8.6% to water pollution with disinfection byproducts, and 6.0% to air pollution with PM2.5.
Conclusion
This study underscores the urgent need to mitigate UBC risk in Lebanon through tobacco control and by reducing exposure to preventable environmental and occupational risk factors, including tobacco smoking, water pollution, and air pollution.
Background
Cancer is the second leading cause of death globally. 1 Urinary bladder cancer (UBC) is among the most prevalent and costly cancers due to its high recurrence and extensive diagnostic and treatment needs.2-5 In 2020, UBC ranked 10th globally in cancer incidence (6th in males), with 573 000 new cases and 213 000 deaths. 5 Males are 3 to 4 times more likely to develop UBC, with global age-standardized incidence rates (ASIRw per 100 000 population, adjusted to the world population) of 9.5 for males and 2.4 for females in 2020. 5
UBC is most prevalent in countries with very high Human Development Index, with the highest rates reported in Europe and North America (ASIRw: 19.4 per 100 000 males and 4.6 per 100 000 females).5,6 South-central Asia, Central America, and sub-Saharan Africa have the lowest UBC incidence rates.5,6
Several risk factors contribute to UBC development.5,7-12 Tobacco smoking is the leading contributor to geographic and sex disparities, as well as for temporal patterns in UBC incidence and mortality rates worldwide.5,9-13 Cigarette smoking accounts for about 50% of all UBC cases, particularly urothelial cell carcinoma (UCC).14-16 Occupational exposure to aromatic amines and other hazardous chemicals used in firefighting or in paint processing, dye, rubber, metal (e.g., aluminum), and petroleum products is the second most significant risk factor.7,8,10,11 Environmental pollution, especially drinking water contaminated with arsenic or chlorine/trihalomethanes and possibly ambient air pollution, also contributes to UBC risk.7-11 Chronic inflammation of the urinary tract, particularly with Schistosoma haematobium (S. haematobium) in regions of northern and sub-Saharan Africa, further elevates the risk.5,8-13 Genetic predispositions and mutations, particularly when combined with smoking, can also increase susceptibility.8,10,11 To reduce UBC-specific morbidity and mortality, primary prevention is key, particularly through avoiding exposure to carcinogens such as tobacco smoke, the leading risk factor.11-17 Despite advancements in diagnostics, there is no consensus on cost-effective screening methods for high-risk groups.11,18-22
The World Health Organization (WHO) projects that the Eastern Mediterranean region will experience the highest increase in cancer incidence among all regions over a 15-year period beginning in 2012. 23 In this region, lung and bladder cancers are the most prevalent among men, while breast and colorectal cancers are the most common among women. 23 Unfortunately, the majority of cancer patients in this region seek treatment at an advanced stage, which significantly reduces the effectiveness of even the best available treatments. 23
This study analyzes the 12-year incidence rates and temporal trends of invasive UBC in Lebanon. It also compares the incidence rates of UBC in Lebanon to those in the Middle East and North Africa (MENA) region and other countries/regions worldwide. Furthermore, the study discusses the various factors contributing to the UBC age-standardized incidence rates in Lebanon and concludes with recommendations for effective UBC prevention and screening.
Materials & Methods
Lebanon
Lebanon, a developing country in the Middle East with a population of 6.3 million in 2016 (including about 1.6 million refugees, displaced persons, migrants, and refugees), 24 achieved a Human Development Index (HDI) of 0.757 in 2017 (the time corresponding to the data of this manuscript). 25 In 2015, life expectancy at birth in Lebanon was 76.0 years. 24
The Lebanese National Cancer Registry (NCR)
In 2002, following years of conflict, Lebanon’s Ministry of Public Health (MoPH) reinstated the national cancer registry (NCR). The NCR records for new cancer cases in Lebanon are almost complete (over 90%) but exclude in-situ lesions. 26 All sites involved in diagnosing and treating cancer report new cancer cases to the NCR through CanReg5. This WHO-recommended tool is an open-source software that facilitates the input, storage, validation, and analysis of cancer registry data. There are two ways that the MoPH constantly collects data: the capture system passively receives data from doctors’ reports, and the recapture system actively collects data from histopathological and hematological laboratories to verify the capture system input.26,27 Cancer incidence data, covering the years from 2005 to 2016, is available on the MoPH website. 27
Twelve-Year Trend Analysis from 2005 until 2016
In this study, data encompass diagnoses of invasive UBC (C67) as classified by the International Classification of Diseases, 10th revision (ICD-10). This study examined the ranking of UBC among all cancers in males and females during the study period (2005-2016). The age-standardized incidence rate (ASIRw), adjusted to the world-standard population by Doll as a reference population 28 and the age-specific incidence rates 29 per 100 000 population were calculated using figures published by the Lebanese NCR on the MoPH website for the years 2005-2016. 27
The Joinpoint Regression Program (JRP) version 4.7.0.0 was utilized to analyze trends in the observed cancer ASIRw. 30 Joinpoint regression applies a Monte Carlo permutation method to identify statistically significant changes in trends (joinpoints) and the rate of change (annual percent change) in each trend segment. 30 The JRP calculated the average annual percent change (APC) of UBC incidence rates among males and females over the years. Additionally, it computed the APC for age-specific UBC incidence rates. A P-value of less than 0.05 was deemed statistically significant. 30
Comparison of UBC Incidence Rates in Lebanon to Other Countries
This study compares Lebanon’s UBC ASIRw and age-specific rates with t regional and global estimated data from the Global Cancer Observatory (Cancer Over Time), published by the International Agency for Research on Cancer (IARC), which is affiliated with the WHO. 31 The Observatory reports age-standardized incidence rates (ASIRw), adjusted to the world-standard population using Doll’s reference, based on high-quality, population-based cancer registries. 28
Estimation of the Population Attributable Fraction (PAF) of Smoking, Water Pollution with Disinfection Byproducts, and Air Pollution with PM2.5 on UBC Incidence in Lebanon, 2016
We conducted a retrospective data analysis to investigate the relationship between exposure to a specific risk factor and UBC incidence. We employed the population attributable fraction (PAF) to estimate the effect of trihalomethanes (THMs) on bladder cancer incidence in Lebanon.
The PAF indicates the proportion of disease cases that could be prevented if the population were not exposed to a particular risk factor. This measure accounts for both the prevalence of exposure and the increased risk it entails. Therefore, PAF estimates are useful for planning and prioritizing strategies to reduce the population’s cancer burden.
To calculate the PAF of a risk factor’s cancer burden, two key components are required: the prevalence of the population exposed to the risk (Pe) and the relative risk of cancer associated with that risk factor (RRe). Usually, cancers arising from exposure to a risk factor result from prolonged exposure over an extended period, with a 10-year latent period generally being adequate for most cancer risk factors. 32
We used a standard formula: PAF = Pe (RRe−1) / [1 + Pe (RRe−1)] if a risk factor is present at a single exposure level. 33
We applied a modified version of the Levin formula: PAF = Pe1 (RRe1-1) + Pe2 (RRe2-1) / 1 + [(Pe1 (RRe1-1) + Pe2 (RRe2-1)] in the case where the risk factor shows more than one exposure level (e.g., in tobacco smoking: former smokers, current smokers). 33
Our analysis primarily relied on WHO estimates, population-based reports, and studies with representative samples of the Lebanese population. These sources identified the proportion of the population at risk approximately a decade ago, considering that the impact of the risk factor is not immediate and requires a 10-year lag to draw meaningful conclusions. 32 The study used the WHO’s estimate of the prevalence of current tobacco smoking in Lebanon in 2005 (35.1% in males and females, 41.1% in males, and 28.7% in females), supplemented with the WHO’s STEP estimate of former tobacco smoking prevalence in Lebanon in 2009 (6.9% in males and 3.3% in females), as there was no prior data on the prevalence of former smokers in Lebanon.34,35,
A study on THM contamination levels in drinking water revealed that 94.1% of the networks investigated in Lebanon exceeded the United States Environmental Protection Agency (USEPA) range of concern for increased carcinogenic risk from THM. 36 According to the Central Administration for Statistics (CAS), Lebanon’s drinking water sources are either underground water or surface water. 37 Therefore, we can consider bottled water, originating from either ground or surface water, to be representative of both. Lebanon’s ambient air pollution with particulate matter that is 2.5 microns or smaller in size (PM2.5) exceeds WHO guidelines.38-42 In this analysis, we considered that at least 90% of the population in Lebanon has long-term exposure to ambient air pollution with PM2.5.
We used multiple adjusted UBC relative risks (RRe) from meta-analyses of epidemiological studies for each risk factor: current smoking (3.47 in males and females, 3.44 in males and 3.56 in females), former smoking (1.92 in males and 2.04 in females), THM pollution in water (1.1), and PM2.5 pollution in the ambient air (1.07), to estimate the corresponding PAF.15,16,43,44
Results
Twelve-Year Trend Analysis (2005-2016)
Over the study period (2005-2016), excluding non-melanoma skin cancer, UBC was the third most common cancer in males (12.85% of all new cancer cases) and the eighth most common cancer in females (2.82% of all new cancer cases).
We computed the APC for all study participants to reflect trends in the ASIRw of UBC among males and females throughout the 12-year study period. With a 0 Joinpoint model, the UBC ASIRw among both males and females decreased non-significantly from 2005 to 2016 (APC: −2.35 and −2.13, respectively, P-value > .05) (Figure 1). However, the best Joinpoint model identified three trends in the Lebanese ASIRw of UBC in males and two trends in females. In males, there was a significant increase in the period 2005-2009 (APC: 7.60, P-value < .05) with a peak in 2009 (37.7), followed by a significant decrease in the period 2009-2013 (APC: −10.68, P-value < .05), and then a non-significant increase in the period 2013-2016 (APC: 3.85, P-value > .05), reaching 25.2 in 2016 (Figure 2). In females, there was a significant increase during the period 2005-2008 (APC: 11.48, P-value < .05), with a peak in 2008 and 2009 (8.9), followed by a non-significant decrease in the period 2008-2016 (APC: −5.32, P-value > .05), reaching 5.70 in 2016 (Figure 2). Age-Standardized Incidence Rates (World Population) per 100,000 Population for Bladder Cancer (ICD10: C67) in Lebanon for the Years 2005-2016. (Model: 0 JoinPoint). Age-Standardized Incidence Rates (World Population) per 100,000 Population for Bladder Cancer (ICD10: C67) in Lebanon for the Years 2005-2016. (Final Selected Models: 2 Joinpoints in Males, and 1 JoinPoint in Females).

UBC incidence rates increase with age. Figure 3 illustrates the increasing UBC incidence rates in Lebanon with age in the years 2005-2016. Age-Specific Incidence Rates (per 100 000 Population) for Bladder Cancer (ICD10: C67), Lebanon 2005-2016.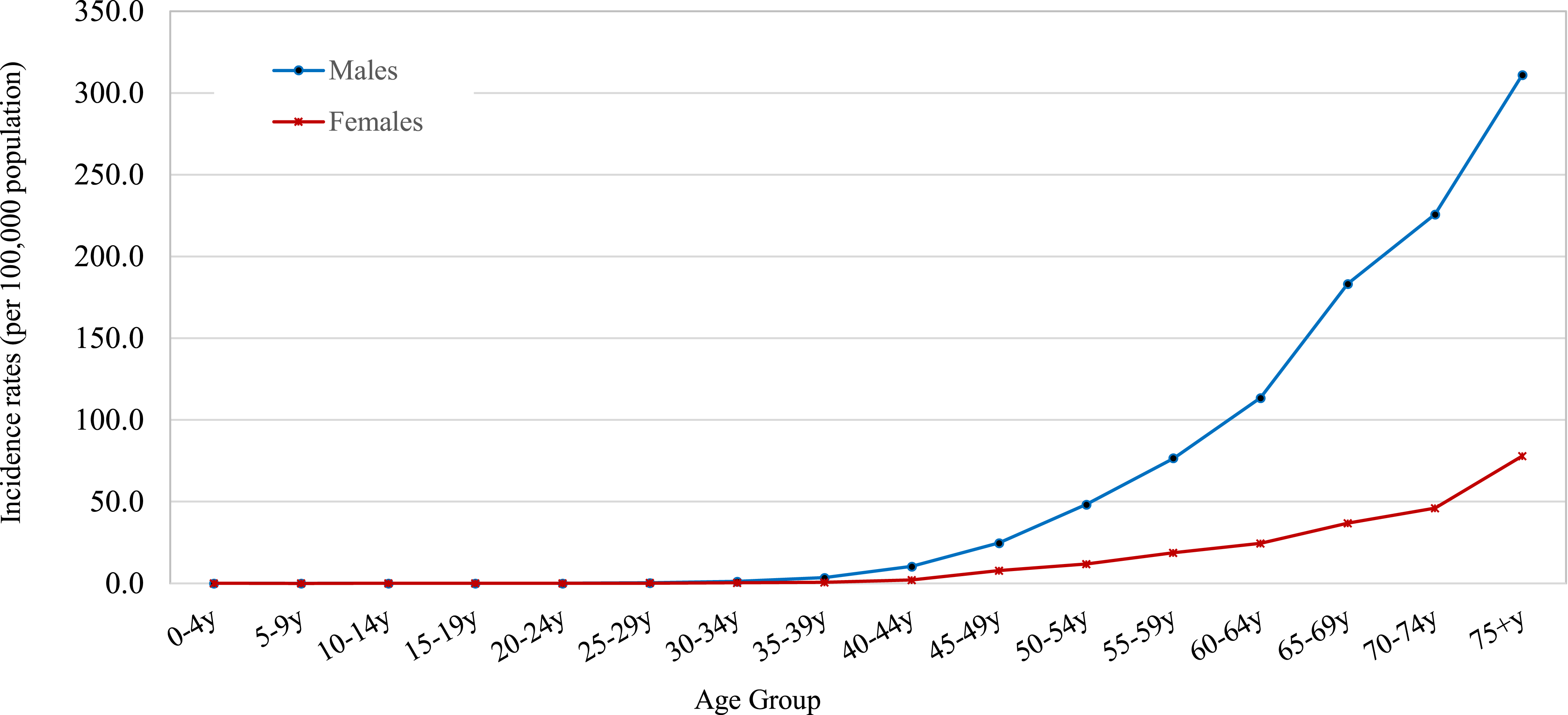
Bladder Cancer (ICD10: C67) Age-Standardized Incidence Rate (World Population) and Age-specific Incidence Rates in Lebanon in the Years 2005-2016.

Abbreviations: ASRw, Age-Standardized Incidence Rate (World Population); APC, Annual Percent Change.
*Indicates that APC is significantly different from zero at the alpha = 0.05 level.
Results from Global Cancer Observatory, Cancer Overtime Statistics (2012-2016)
The Global Cancer Observatory’s Cancer Overtime Statistics website provides data for the UBC ASIRw in various countries from 2012 to 2016 (5 years), but it does not include Lebanon.,
31
This allows for a comparison with Lebanon’s national registry data, which also uses ASIRw. Figure 4 reveals that Lebanon’s UBC ASIRw is among the highest worldwide, ranking sixth for men and 10th for women compared to other reported countries and territories. GLOBOCAN Estimates for Bladder Cancer (ICD10: C67) Age-Standardized Incidence Rate (World) per 100 000, Males and Females, [2012-2016].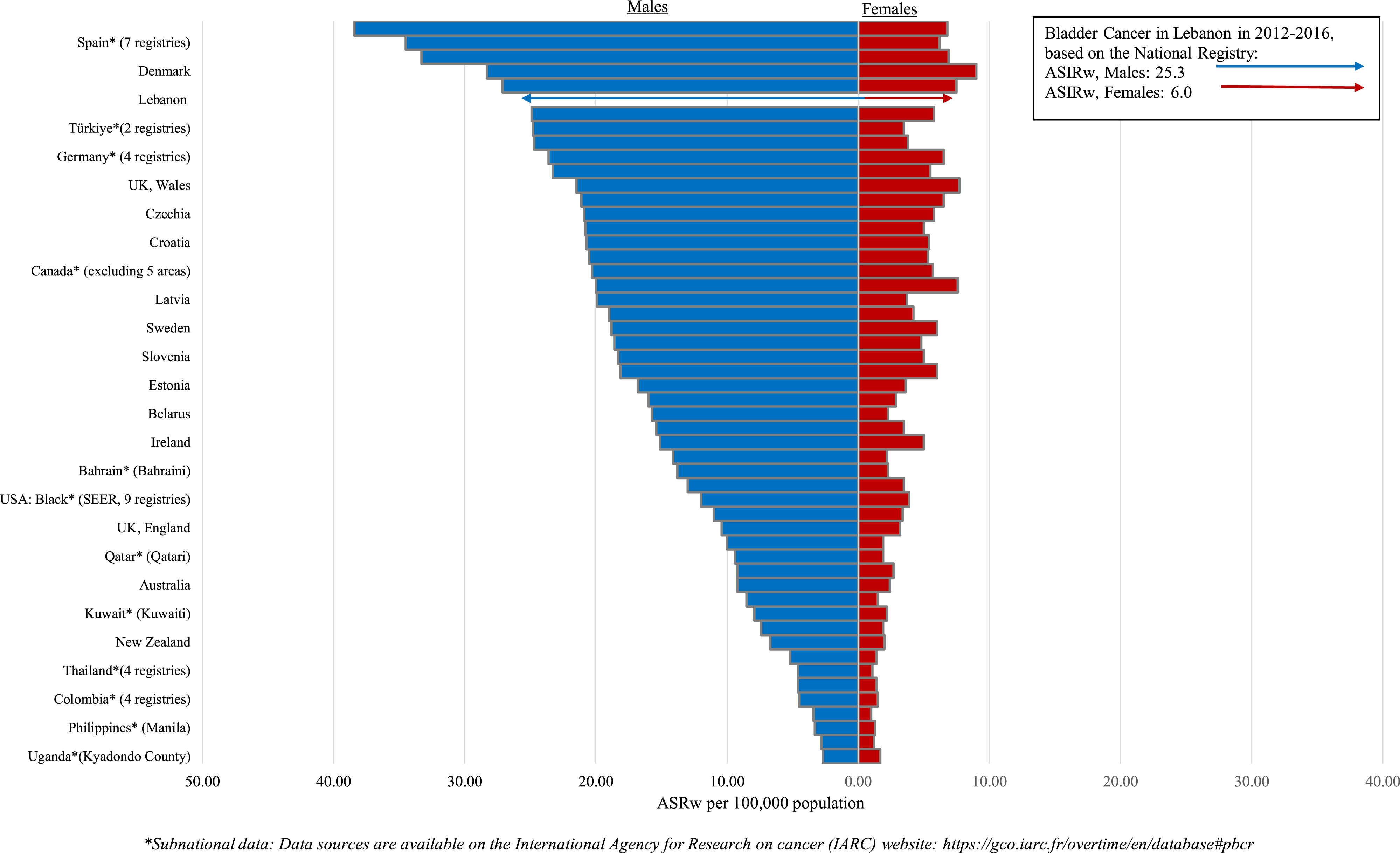
Estimation of the Population Attributable Fraction (PAF) of Smoking, Water Pollution with Disinfection Byproducts, and Air Pollution with PM2.5 for UBC Incidence in Lebanon, 2016
Smoking
Percentage Attributable Fraction (PAF) of Smoking, THM, and Air Pollution With PM2.5 on Bladder Cancer (UBC) Cases in Lebanon.
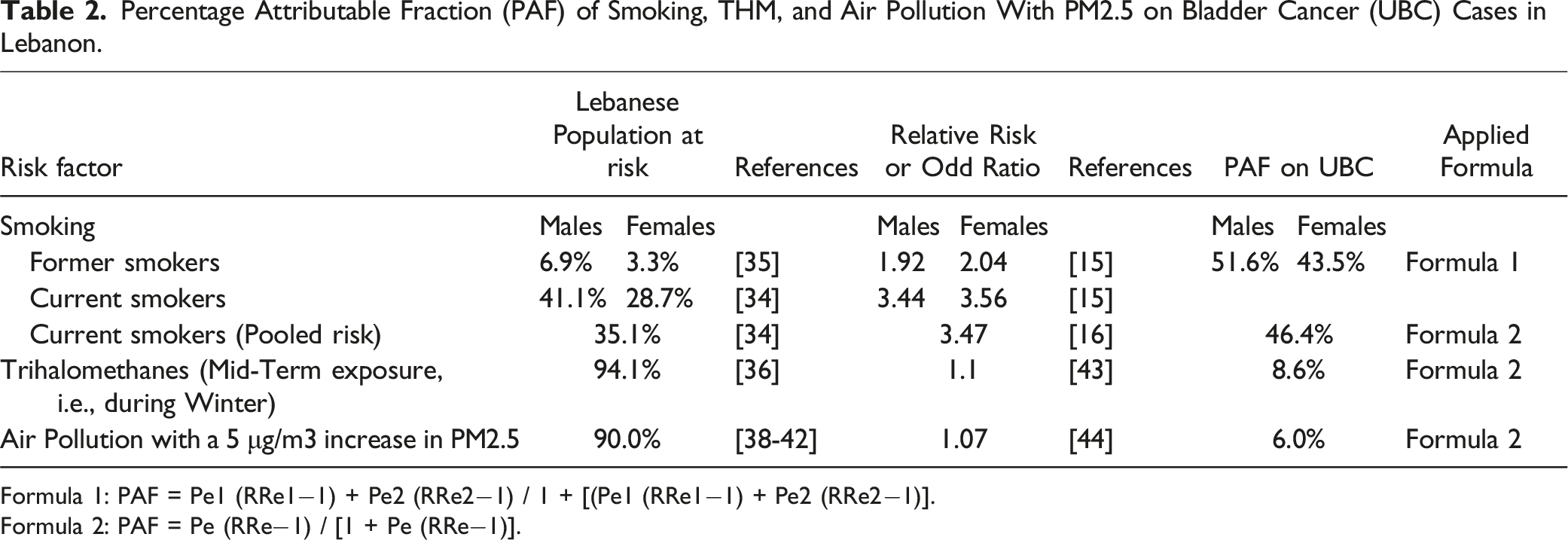
Formula 1: PAF = Pe1 (RRe1−1) + Pe2 (RRe2−1) / 1 + [(Pe1 (RRe1−1) + Pe2 (RRe2−1)].
Formula 2: PAF = Pe (RRe−1) / [1 + Pe (RRe−1)].
Water pollution with disinfection byproducts (DBPs) from chlorination, specifically trihalomethanes (THMs): We estimated that 8.6% of UBC cases in Lebanon in 2016 were attributed to water pollution with THMs across all age groups and both genders.
Ambient Air Pollution with PM2.5
We estimated that 6.0% of UBC cases in Lebanon in 2016 were attributed to air pollution with PM2.5 across all age groups and both genders.
Discussion
The Global Cancer Observatory (Cancer Over Time) does not report cancer incidence rates for Lebanon. 31 Using the MoPH’s NCR and world standard population, Lebanon had one of the highest UBC incidence rates (ASIRw) globally. The Global Burden of Disease (GBD) 2019 report, using a different standardized population, ranked Monaco (31.9) and Lebanon (30.2) as having the highest global UBC ASIRs per 100 000. 45 UBC also imposes a significant economic burden in Lebanon.46,47
A 2020 study by Teoh et al. examined international UBC trends over a decade, noting declining incidence and mortality in Oceania and the Americas, rising incidence but declining mortality in Europe, and decreasing incidence but increasing mortality in Asia. 13 In this study, tobacco use correlated positively with UBC incidence (r = 0.20 in men and r = 0.67 in women) and mortality rates (r = 0.38 in men and r = 0.22 in women). 13 Lebanon saw a slight decline in UBC ASIRs between 2005 and 2016, aligning with mildly reduced tobacco use, though mortality data remain unavailable.48-51
Geographic variations in UBC incidence are linked to tobacco use, environmental and occupational risks, as well as healthcare disparities. 52 In Africa, late-stage presentations limit treatment options. 52 While UBC diagnoses are expected to increase with global population growth and aging, the overall risk may not necessarily rise. Globally, life expectancy increased from 66.8 years in 2000 to 73.3 years in 2019, and in Lebanon, from 74.6 to 76.4 years. 53 The United Nations (UN) projects a global population of 9.7 billion by 2050, with the 60-plus population more than doubling, thereby increasing the burden of late-onset diseases like UBC, particularly in Africa, where the population is expected to nearly double between 2017 and 2025. 54
Prevention is key: primary prevention targets risk behaviors like tobacco use, secondary prevention focuses on early detection in high-risk groups, and tertiary prevention aims to prevent complications. UBC is rising in various MENA countries (Figure 5), largely due to tobacco smoking.
55
The following discussion highlights primary prevention efforts in Lebanon, while also recognizing the complex etiology of UBC. Globocan Estimates for Bladder Cancer Incidence Rates (ASRw) for the Year 2022 in the MENA Countries.
Primary Prevention of UBC
Understanding modifiable risk factors is key for cancer prevention. While age and male gender are non-modifiable, factors such as tobacco use, exposure to carcinogens, and chronic urinary inflammations (e.g., S. haematobium) are preventable. Although Genome-Wide Association Studies (GWAS) highlight genetic susceptibility, its role in public health remains unclear.
Tobacco Smoke
Tobacco smoke from cigarettes, waterpipes (shisha), cigars, or pipes contains carcinogens that damage the Deoxyribonucleic Acid (DNA), significantly increasing UBC risk.7-16 Smoking remains the leading global UBC risk factor,12-16 with secondhand smoke contributing to a lesser extent.15,16,56 Similar to our study, tobacco smoking has a PAF of around 50% for UBC in the United States of America (USA) (50-65% in men and 20-30% in women), reflecting its significant impact on UBC incidence.14,57,58
Despite a global decline, tobacco is rising in North Africa and the Middle East, including Lebanon, where smoking rates in 2025 are projected to be among the highest worldwide: 55.4% (men) and 37.7% (women).48,49 Weak anti-smoking policies and industry interference hinder control efforts, necessitating stronger enforcement to mitigate cancer risks.59-61
Water and Vegetables Chemical Pollution
Arsenic in drinking water is a known risk factor for UBC.7-11,62-68 Most high-income countries adhere to WHO guidelines, limiting arsenic levels to 10 μg/L. 62 Chronic exposure to arsenic, even at low concentrations (10 μg/L), increases cancer risk and other health issues.62,64 Exposure to 10 μg/L of arsenic in drinking water can double the UBC risk or increase it by approximately 40%. 64 Cadmium, primarily sourced from food in non-smokers, is a probable UBC risk factor. 69 Prolonged exposure to chlorinated domestic water, through disinfection byproducts (DBPs) like trihalomethanes (THMs), also increases UBC risk.7-11,70-75 Exposure to THM levels above 25 µg/L causes a 35% or higher risk for men. 74 DBPs account for 10% of UBC cases in the USA and 23.2% in Europe, with an average of 4.9%, despite laws and monitoring.72,73
Lebanon’s aging water infrastructure, cross-contamination, and industrial pollution cause fecal coliforms, excessive heavy metals (e.g., arsenic and cadmium) levels, and pesticides.36,37,76,77 Population growth, the Syrian refugee crisis, economic instability, and climate change worsen water shortages and contamination, 78 increasing UBC risks. Arsenic and cadmium contamination of coastal water, agricultural soil, and cops in Lebanon further compound the public health risks. 78
Environmental Risk Factors for UBC - Ambient Air Pollution
Ambient air pollution from industry, power generation, transportation, and domestic burning can cause systemic inflammation, oxidative stress, and DNA damage, potentially increasing UBC risk.44,79-83 While strongly associated with lung cancer, long-term PM2.5 exposure is probably associated with UBC.44,79-86 A 5 μg/m3 increase in PM2.5 raises UBC risk by 7%, and a 10 μg/m3 increase in NO2 raises it by 4%. 44 The role of polycyclic aromatic hydrocarbons (PAHs) in ambient air as a UBC risk factor remains unresolved. 44 Air pollution and tobacco smoking may have a synergistic effect on UBC rates.
Ambient air pollution is a major issue in Lebanon.87-93 Lebanon had the highest per capita air pollution rate in the Middle East, along with Egypt, with 2700 premature deaths in 2018 costing $1.4 billion (2% of GDP), according to a 2020 Greenpeace research study. 92 From 1990 to 2019, Lebanon’s mean annual exposure to PM2.5 air pollution surpassed 18.0 μg/m3, above the earlier WHO guideline of 10 μg/m3, which was lowered to 5 µg/m3 in 2021 to reduce health hazards and save millions of lives, according to the GBD 2019.38,93,94 Greater Beirut studies reveal PM10, PM2.5, and NO2 exceed earlier WHO guidelines.38-42 Unregulated private diesel-fueled generators and heavy traffic, especially in Greater Beirut, pollute Lebanon.90,93 Small enterprises and uncontrolled power plants also contribute to pollution. The 2020 Beirut blast and diesel generators ongoing operation owing to power grid failures further worsened air quality, resulting in around 24.2 μg/m3 PM2.5 annual mean levels in Lebanon. 93 Despite Lebanon’s 2018 WHO-based air quality law, the country has taken little action to mitigate the growing air pollution. In 2013, Lebanon’s Ministry of Environment launched the national air quality monitoring network (AQMN), which expanded in 2017. AQMN reports over the past decade reveal that NO2, PMs, and volatile organic compounds (VOCs) levels consistently exceed WHO annual limits. 92
Occupational Exposure to Pollutants
Workplace exposure to carcinogenic chemicals, such as aromatic amines (e.g., 2-naphthylamine, 4-aminobiphenyl, benzidine) and 4,4-methylenebis (2-chloroaniline), accounts for 20%-27% of UBC cases in industrialized countries.7,8,17,95,96 These hazardous exposures are common in dye, paint, fungicide, rubber, plastics, metals (e.g., aluminum), and petroleum industries.7,8,17,95,96
Lebanon has thousands of small- to medium-sized industries, most of which operate without proper safety measures. 97 Many businesses produce agrifood products, construction materials, chemicals (pharmaceuticals, plastics, paints and derivatives, soaps, and detergents), printed materials, furniture, wood products, and natural stones. 98 Additionally, occupational exposure to diesel or fuel combustion emissions in Lebanon’s cities is an independent UBC risk factor. 99 Recent large epidemiologic studies back up the IARC’s finding that diesel exhaust exposure raises UBC risk.80,100 Although regulatory measures exist, weak enforcement underscores the need for stronger public health interventions. 101
Infection with Schistosoma Haematobium
Schistosoma haematobium causes most UBC squamous cell carcinoma (SCC). SCC dominated UBC in schistosomiasis-endemic countries like Egypt for years, but not anymore because of successful schistosomiasis control. 102 In Egypt, SCC cases dropped from 78% in 1980 to 27% in 2005, while transitional cell carcinoma (TCC) rose from 22% to 73%. 103 Public health measures and the Aswan High Dam’s construction replaced S. haematobium with S. mansoni, reducing infection rates, except in Minya.104,105
Lebanon has eradicated schistosomiasis with no new cases reported in recent years. 106 In fact, the majority of UBC cases are non-SCC.26,99
Genetic Susceptibility
Inherited mutations such as BRCA and Lynch syndrome, along with acquired genetic variations discovered in genome-wide association studies (GWAS), influence UBC.11,107 Family history of UBC increases risk, suggesting a genetic predisposition beyond environmental influences. 107 DNA mismatch repair genes (e.g., MSH2, MSH6, MLH1) in Lynch syndrome are the only established hereditary UBC risk factors. GWAS have identified many acquired genetic mutations (28 susceptibility loci) associated with UBC risk.17-19,108 These include NAT2 and GSTM1 gene modifications that repair and detoxify DNA. These changes can increase cancer risk, especially along with tobacco smoking, environmental pollution, and certain occupational hazards.17-19,108 The MENA region is understudied because most GWAS studies have focused on populations in Europe, the USA, and Asia.17-19,108 Novel evidence suggests that bladder carcinogen THMs interact with specific genotypes (e.g., rs907611). 109
In Lebanese patients, a case-control study found no associations between UBC and known genetic variants, like NAT1 rs4986782. 110 Previous studies found that Lebanese UBC patients had higher NAT1*14A concentrations than controls, which is in line with findings from Michigan Lebanese communities.111,112 To identify preventive targets, these findings suggest integrating genetic data with tobacco smoking, environmental pollution, and occupational toxins.
Early Detection of UBC in High-Risk Populations
Most medical organizations do not recommend UBC screening for asymptomatic, average-risk adults.18-21 The European Society for Medical Oncology and the United States National Cancer Institute advise prompt attention to bladder symptoms as the best early detection method.18,19 While early detection is crucial, hematuria dipstick testing has low predictive value. 113 Some urinary biomarkers could be used for early UBC diagnosis, 114 but more research is necessary to evaluate their cost-effectiveness in screening asymptomatic high-risk groups. 11 The IARC’s uTERTpm urine biomarker assay shows promise in early UBC detection, particularly for high-risk groups like smokers. 115 It detects TERT gene promoter mutations non-invasively by testing two separate urine samples. 115
Raising Public Awareness
Public awareness is also crucial in reducing UBC incidence and mortality. Studies in Lebanon have shown significant gaps in public knowledge about the disease, its symptoms, and its link to tobacco use, underscoring the need for targeted awareness campaigns. 116
Improving Access to Timely Diagnosis and Care
Timely access to imaging (e.g., CT urography), cystoscopy, and biopsy, is crucial for accurate diagnosis and treatment, especially in underprivileged patients. Up-to-date care and genetic profiling help tailor treatment options and identify potential therapeutic targets.
Improving Cancer Data and Monitoring
Lebanon, like many countries in the MENA region, lacks comprehensive cancer registries and electronic medical record systems that hinder effective cancer surveillance and control. 117 Population-based cancer registries are essential for tracking new cases, deaths, and survivals to evaluate cancer control strategies. 118 However, inconsistencies in cancer registration and coding practices complicate incidence and mortality comparisons. Accurate coding plays a crucial role in differentiating between invasive and non-invasive (in situ) UBC, which makes up 75% of cases and has a favorable prognosis but also carries a high risk of recurrence.5,9,119 Outcomes research is also crucial to evaluate and improve intervention strategies.
Limitations of the Study
This study estimated the PAFs for UBC associated with smoking, water pollution with THMs, and air pollution with PM2.5 as potential risk factors. However, limited data prevented sensitivity analyses for these calculations, potentially affecting the robustness of the estimates due to variations in the underlying assumptions and data inputs. Additionally, limited data excluded other UBC risk factors (e.g., secondhand smoke, water and vegetable contamination, other air pollutants, occupational exposure to other carcinogens, family history of UBC) and covariates (e.g., dietary habits, body mass index, socioeconomic status) from the analysis, which may have introduced bias. Cancer data from Lebanon’s MoPH website, though improved between 2014 and 2016, remains incomplete, lacking information on precancerous and in situ conditions, as well as mortality and survival rates. Notably, the MoPH has not published any cancer-related data since 2016, posing a risk to the progress of the NCR.
Conclusion
Lebanon has one of the highest UBC rates globally, primarily driven by tobacco smoking and, to a lesser extent, by water and air contamination. Strengthening tobacco control, investing in cessation programs, and raising awareness are crucial. Improving water and air quality must also be a priority, with clear goals for long-term progress. These measures are essential for reducing UBC rates and protecting public health.
Footnotes
Statements and Declarations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.