
Abstract
Background
An older age contributes to the development of bladder cancer. However, the relationship between advanced age at the diagnosis and prognosis of bladder cancer has been few reported. This study aimed to determine the effect of age on survival in bladder cancer with different subgroups.
Methods
117,275 patients with bladder cancer, identified from the Surveillance, Epidemiology, and End Results database during 2004-2015 in America, were divided into 4 age groups (≤54, 55 to 64, 65 to 74, and ≥75 years). Multivariable Cox proportional-hazards model and competing risk model were conducted according to different age groups. Heat maps were plotted to show the impact of age on survival in subgroups classified by other clinicopathological variables. Moreover, restricted cubic spline was used to model the association between age and the risk of death.
Results
Patients aged ≥75 years had shorter overall survival in comparison with those aged ≤54 years (hazard ratio [HR] = 5.36, 95% confidence interval [CI] = 5.13-5.59). Compared with patients aged ≤54 years, patients older than 75 years experienced a decreased rate of bladder cancer-specific survival (subdistribution HR = 2.15, 95% CI = 2.04-2.25). Heat maps also showed that older ages were associated with worse overall cumulative mortality and bladder cancer-specific cumulative mortality. Similarly, restricted cubic spline verified the impact of age on survival of bladder cancer.
Conclusions
Age at diagnosis of bladder cancer was found to be a significant predictor for the worse overall survival and bladder cancer-specific survival even in an era with more effective therapies. Exploring the reasons why older age contributes to poor outcomes for bladder cancer will be the focus of future research.
Introduction
Bladder cancer is the tenth most common malignancy in the world. According to statistics, in 2020, there were 573,278 new cases and 212,536 deaths worldwide. Bladder cancer is mainly a male tumor, as the incidence is up to four times that in women. 1 While to some extent, this difference can be attributed to tobacco consumption. 2 In the US, bladder cancer causes 4% of deaths in men and 2% in women. Although men are four times more likely to develop the disease than women, the death rate is only twice as high. 3
The mean age at diagnosis of bladder cancer is 73 years old, which is older than the average age (65 years old) at diagnosis of all cancers. 4 In the US, 90% of bladder cancer diagnoses are made in people over 55, and 80% are made in people over 65. 5 Also, we found that bladder cancer was the fourth leading cause of cancer deaths in American men over the age of 80 years. 3 Previous studies have shown that the 3-year overall survival rate for bladder cancer was 70%, whereas the 10-year overall survival rate was only 42%. The age of patients was divided by 60, and the 10-year overall survival rate of patients younger than 60 years old was 74%, while that of patients older than 60 was only 35%. 6 Thus, advanced age is one of the risk factors for bladder cancer. 7 This can be explained as exposure to carcinogens such as tobacco and an age-related decline in the ability to repair DNA. 8
Current studies showed that immune checkpoint inhibitors could significantly prolong survival time in patients with advanced urinary tract tumors. The addition of immunomaintenance therapy to first-line chemotherapy has also demonstrated significant efficacy, but mainly in patients with positive PD-L1 expression.9-11 However with the growth in the aging population, treatment and management of bladder cancer in the elderly can be expected to become a major challenge. Indeed, little research has been done on the association of the effect of age on bladder cancer prognosis. In this study, the age of patients with bladder cancer was subdivided, and the prognosis of patients with different ages and stages of bladder cancer were discussed.
Materials and Methods
Surveillance, Epidemiology, and End Results Database
This retrospective study used the Surveillance, Epidemiology, and End Results (SEER) Database, which covers about a third of the US population (https://seer.cancer.gov/). It contains a total of 18 cancer registries, 9 of which have been in existence since 1973. The SEER database records tumor-related information for each cancer patient, such as tumor location, stage, size, and distant metastases, as well as patient social information, such as age, sex, marriage, race, income, residence, etc. In addition, the survival and death status of patients are recorded. The SEER database is a public database, in which information about patients is anonymous. Therefore, our research did not require ethics approval.
Patient Identification
Patients diagnosed with bladder cancer from 2004 to 2015 were extracted from SEER 18 utilizing the SEER*Stat software. All data was cleaned and valuable information was left to analyze. The inclusion criteria were set as follows: (a) diagnosed as bladder cancer (C67.0-67.9, Histologic Type ICD-O-3) with positive histological confirmation. (b) complete data were available with age, survival time, cause of death and follow-up time. The included indicators were social information (age, race, sex, marital status, median annual family income, and county type of residence), tumor-related information (grade and stage), treatment information (radiation, chemotherapy, and surgery), outcome-related information (survival status, survival and follow-up time).
Statistical Analysis
We calculated the proportions of bladder cancer patients with different ages (≤54, 55-64, 65-74, and ≥75 years old) according to characteristics including race (white, black, other, and unknown), sex (female, male), marital status (married, unmarried, and unknown), median annual family income (<$66,610, ≥$66,610), county type of residence (metropolitan, nonmetropolitan), grade (I, II, III, IV, and unknown), 6th AJCC TNM staging (0is, 0a, I, II, III, and IV), surgery (no/unknown, yes), radiation (no/unknown, yes), survival status (alive, dead of this cancer, and dead of other cause), median follow up time.
We used Schoenfeld residuals to test proportional hazards hypothesis by the cox.zph function of R (version 4.1.1) package “survival” in two included models (Cox proportional-hazards model and the Fine-Gray subdistribution hazard model).
12
Based on the finegray function, the Fine-Gray subdistribution hazard model can be fit by first creating a special data set and fitting a weighted Cox proportional-hazards model to the result, and then the cox.zph function could be used to test proportional hazards hypothesis of the Fine-Gray subdistribution hazard model.13,14 Cox proportional-hazards model was subsequently conducted to analyze overall survival (OS) and competing risk model was conducted to analyze cancer-specific survival (CSS). For Cox proportional-hazards model, bladder cancer death was labeled
Results
Patient Characteristics
Characteristics of All Whole Cohort and Different Age Groups.

Outcome Data
Cox Proportional-Hazards Model Analysis of Bladder Cancer Patients.

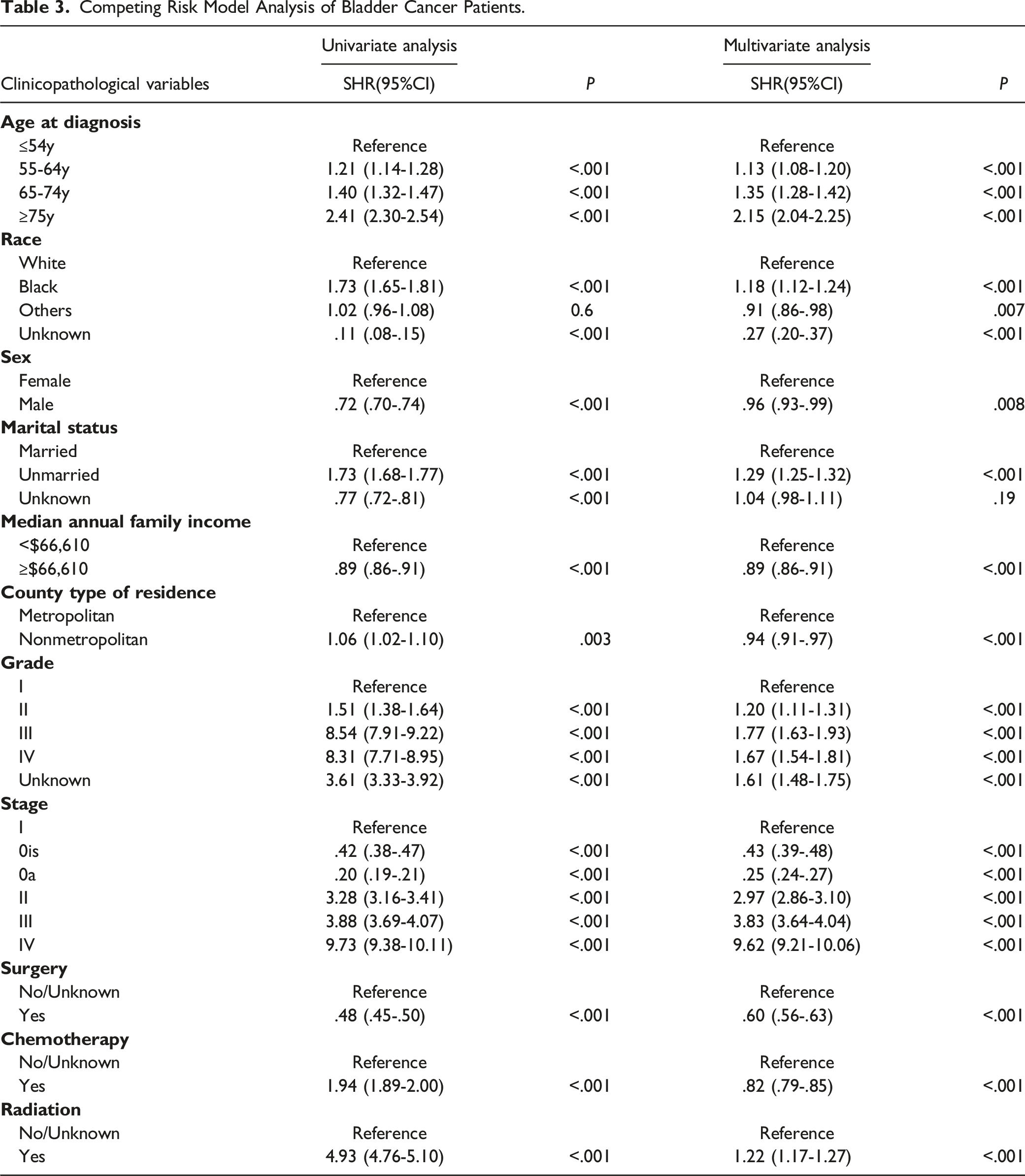
Competing Risk Model Analysis of Bladder Cancer Patients.
In Figure 1, we found that the risk of all-cause of death and cancer-specific death increased with age. Patients aged 75 years or older with bladder cancer had a significantly higher risk of death than those aged 54 years or younger, especially in terms of all-cause of death (Figure 1A). We subdivided the bladder cancer patients according to AJCC staging. We found that age played a significant role in patients with early-stage bladder cancer. In stage IV patients, however, the difference between age and mortality risk was not significant (Figures 2 and 3). The risk of all-cause of death (A) and cancer-specific death (B) increased with age. The risk of all-cause of death increased with age about different stage bladder cancer. The risk of cancer-specific death increased with age about different stage bladder cancer.


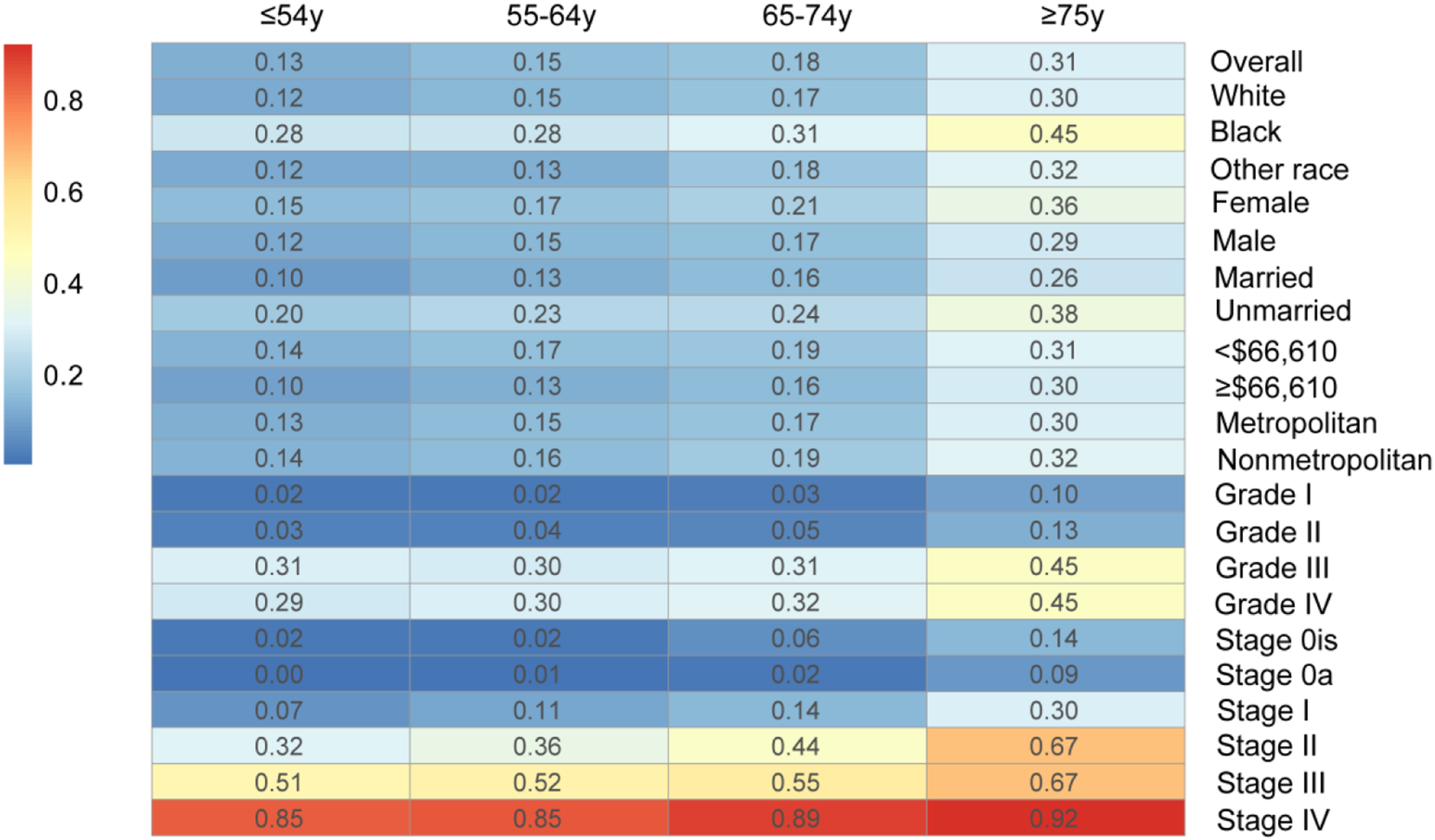
In Figures 4 and 5, we used heat maps to visually show the 5-year total mortality and cancer-specific mortality of patients with bladder cancer. We found that the 5-year total mortality for bladder cancer patients aged over 75 years old was generally greater than 50%, while for those who aged younger than 54 years old was less than 30%. Of course, among patients with advanced bladder cancer, the mortality was higher at all ages (≥86%). In addition, we found that the cancer-specific mortality in patients with bladder cancer aged over 75 years was generally greater than 30%. This ratio was lower than the total mortality. The cancer-specific mortality continued to increasing age, even in stage IV cancer patients. The heat map of 5-year total mortality of patients with bladder cancer. The heat map of 5-year cancer-specific mortality of patients with bladder cancer.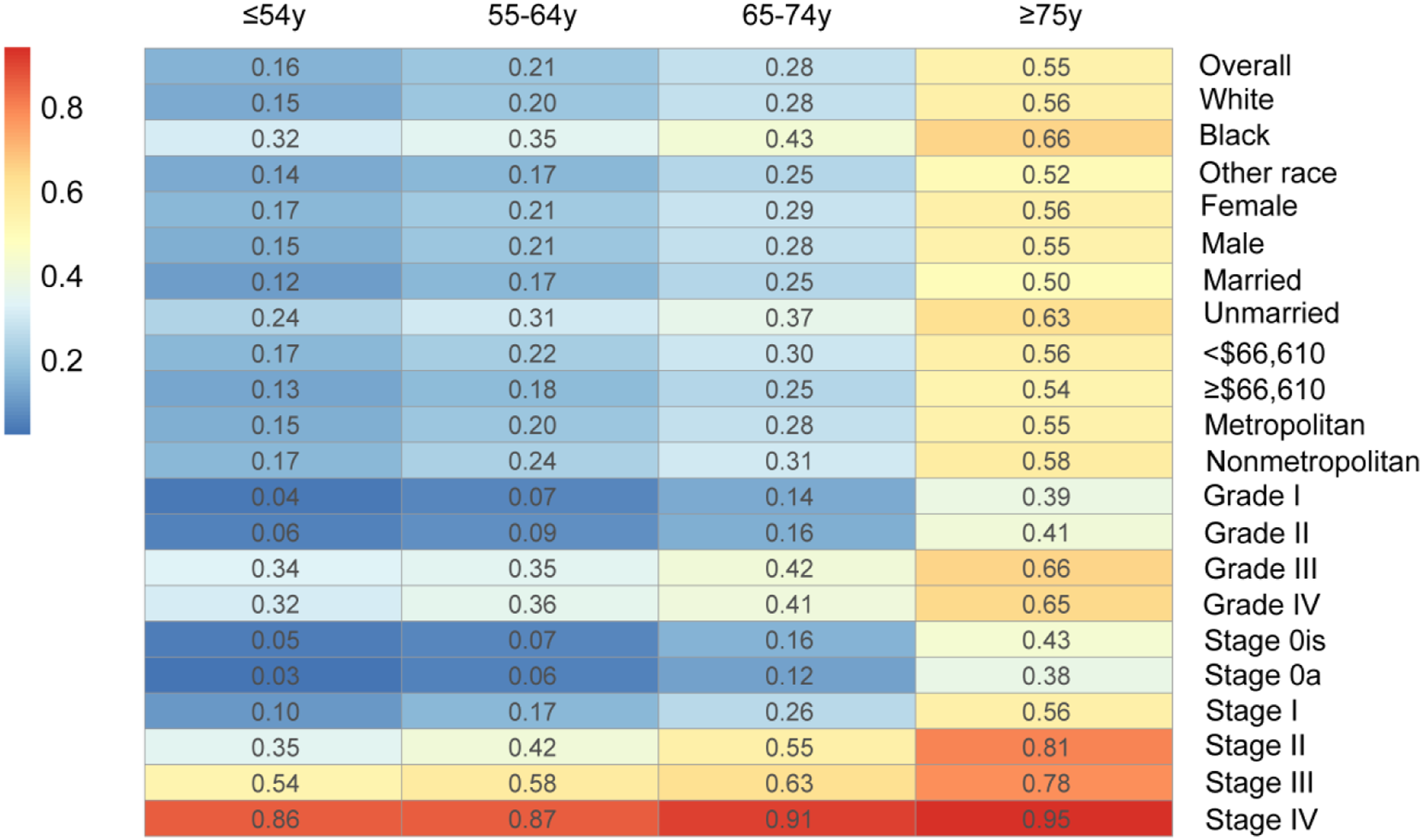
Similarly, in Figures 6 and 7, we found that the 10-year total mortality was generally greater than 70% for patients aged over 75 years old, and the cancer-specific mortality was generally greater than 35%. However, both overall and cancer-specific mortality were lower in patients younger than 54 years of age (<30%). In patients with advanced bladder cancer, both overall mortality and cancer-specific mortality were generally above 90%. In conclusion, the prognosis of patients with bladder cancer was related to age. The heat map of 10-year total mortality of patients with bladder cancer. The heat map of 10-year cancer-specific mortality of patients with bladder cancer.

3, 5, 10-Year Overall Cumulative Mortality and Bladder Cancer-Specific Cumulative Mortality in All Whole Cohort and Different Age Groups.

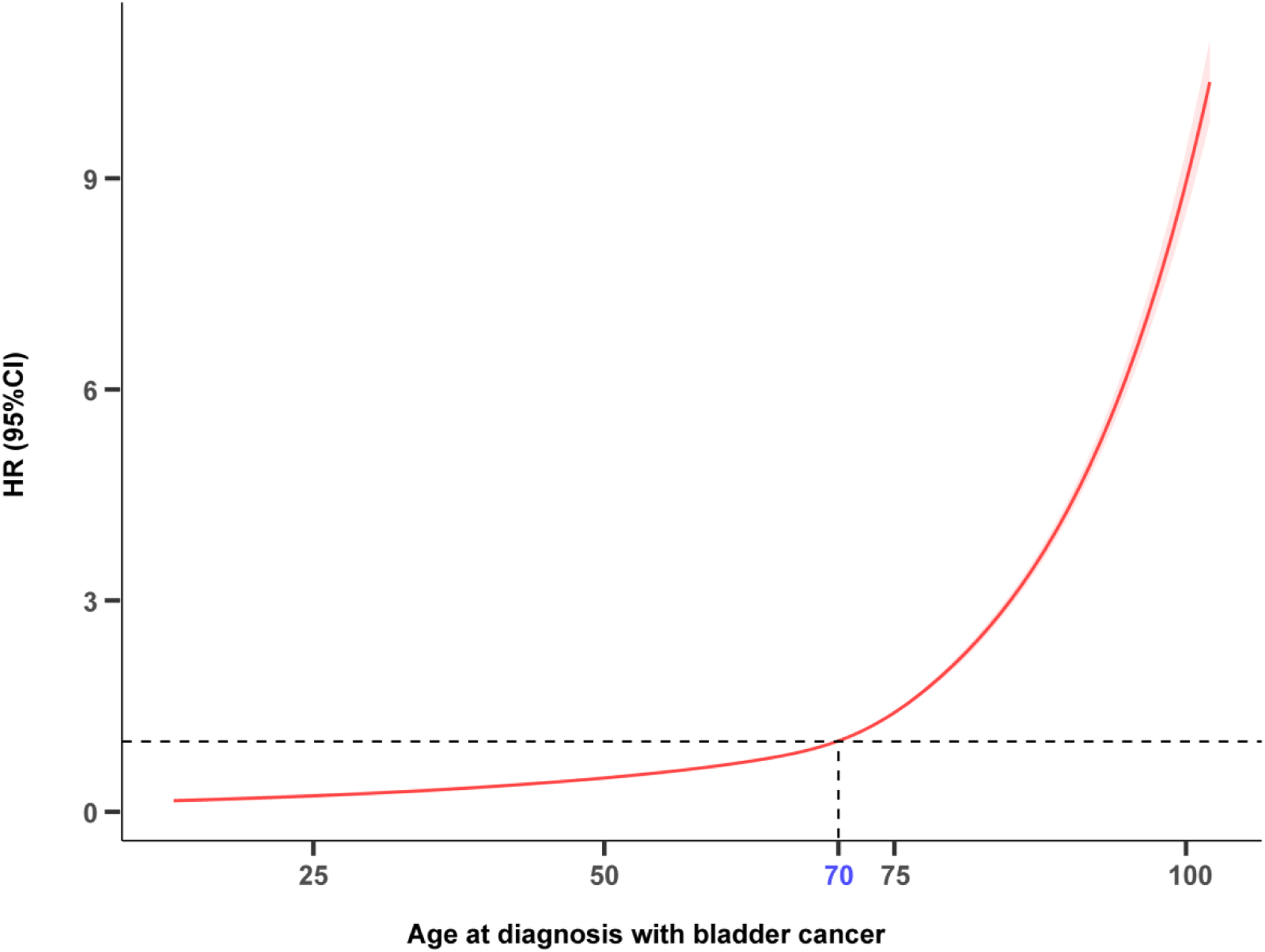
Restricted cubic spline curves showed the risk of death increases with age.
Discussion
This study showed that bladder cancer was more likely to occur in older patients. The incidence of bladder cancer increased with age (≤54 to 55-64 to 65-74 to ≥75) from 12.1% to 21.4% to 22.1% to 38.4%, respectively. Moreover, consistent with our hypothesis, older patients also had poorer prognosis. At 5 years, the OCM and BCSCM in elderly patients with bladder cancer were 55.0% and 30.7%, while in young patients (≤54) were as low as 15.7% and 12.8%, respectively. Also during the 10-year follow-up period, the OCM and BCSCM of older patients were significantly higher than those of younger patients (77.8% vs 20.3%, 38.7% vs 25.6%, respectively).
Previous studies have shown that age was a risk prognostic factor in patients with bladder cancer, especially in untreated patients.6,15-17 Luzzago et al explored the effect of age on prognosis by different disease stages and found that in patients with regional and metastatic bladder cancer, older age was associated with lower cancer-specific mortality. 18 However, our study found that in patients with advanced bladder cancer, both 5-year and 10-year cancer-specific survival and overall survival increased with age, but not significantly.
Tobacco is a rich source of carcinogenic compounds, including polycyclic aromatic hydrocarbons, aromatic amines, heterocyclic amines and N-nitroso compounds. This chemical carcinogen causes large adducts, base damage and DNA strand breaks in bladder epithelial cells. Therefore, smoking is an important factor associated with bladder cancer, and its harm increases with the intensity and duration of smoking.19,20 Smoking may also influence the development of bladder cancer, as reflected in disease-specific mortality among smokers. 21 Smoking is more common among men than women, and the accumulation of chemical carcinogens in the bladder increases with age.22,23 At the same time, there is a delay time between exposure factors and the occurrence of outcomes, the clinical expression of malignant tumors requires a certain amount of time. 24 This is one of the reasons for the increased incidence and mortality of bladder cancer in older men.
In addition to external exposure factors, the internal factors also can not be ignored. In recent years, cancer has come to be regarded as a disease of the elderly. In the US, about two-thirds of malignancies occur in people over 65 years old. Patients older than 65 years old are 15 times more likely to die than those younger than 65 years old. 3 Recently, people have gradually realized that there was an inseparable relationship between aging and malignant tumors. With age, the ability of neutrophils and macrophages to engulf pathogens decreases, leading to immune disorders that promote the development of tumors. 25 In addition, telomeres shorten as cells age, leading to the possibility that aging cells are less able to repair mutations in their DNA.26,27 Several studies have shown that bladder cancer tended to differentiate well in younger patients. Actually, elderly patients are more likely to be diagnosed with advanced stages and non-organ confined diseases.28-30 In younger patients, nearly 40% of cases are papillary urothelial neoplasms with low malignancy potential, and this proportion decreases with age. 31 As a result, younger patients have lower rates of disease recurrence and progression and higher survival rates.
Of course, the difference in outcomes between older and younger patients may also be due to the fact that older patients are less active in treatment and less tolerant to it. First of all, the basic conditions of elderly patients are poor, such as cardiovascular disease, diabetes and other diseases, which make some surgical treatments impossible. 32 Second, post-treatment complications, such as fever, infection and blood clots, also complicate the situation in older people than in younger ones. 33 Third, the presence of liver and kidney disease may affect the optimal dosage of chemotherapy drugs, thus affecting efficacy. 34 Age may also influence the use of immune checkpoint inhibitors, thereby affecting patient outcomes. 35 Intravesical immunotherapy with Bacillus Calmette-Guerin (BCG) is a type of effective treatment for non-muscle invasive bladder cancer. 36 The effectiveness of BCG, however, depends on the ability of the immune response, which declines with age and so does the effectiveness of BCG. 37
Simultaneously, our study found that the cancer-specific mortality in older patients was higher than the overall mortality. According to the statistics, cardiovascular disease is the leading cause of death in the US population, accounting for 23% of all deaths, and cancer is the second leading cause of death at 21%. 3 In addition to cardiovascular diseases, other diseases, such as respiratory diseases and cerebrovascular accidents, are basically more common in the elderly. Therefore, non-cancer mortality also accounts for a certain proportion of the aged.
Elderly patients with bladder cancer is a population that needs attention, and doctors need to tailor treatment for them. By studying the relationship between age and bladder cancer, this article can make doctors pay more attention to the elderly group. Necessary assessment and supportive care for older patients before treatment may lead to better survival outcomes for them. Of course, to find more suitable treatment for elderly patients is the direction of current efforts, and the efficacy of immune checkpoint inhibitors is also being gradually explored in this population. At the same time, further understanding of the molecular and histological subtypes of bladder cancer and their potential prognostic outcomes will also have a certain impact on decision-making.
The effect of age on the prognosis of bladder cancer was carefully discussed in this study. However, some limitations should not be ignored. First of all, this is a retrospective and descriptive study, and there are some unavoidable factors of bias, such as the accuracy and completeness of data recording. Second, the SEER database lacks important treatment information, like the use of intravesical therapies, specific radiotherapy, chemotherapy and surgical treatment, or any other information related to treatment intensity. In addition, some factors that can affect the prognosis of patients, such as smoking, weight, physical status are absent. Third, no information regarding diabetes, hypertension and other comorbidities is available in the SEER database. Most importantly, our data comes from a public database and lacks further validation with external data.
Conclusion
In conclusion, our study provides more clarity on the effect of age on bladder cancer. The high incidence and poor prognosis of bladder cancer are associated with increasing age. Elderly bladder cancer is a progressive phenomenon. Because of its particularity, it faces great clinical challenges. The treatment of older patients needs to strike a balance between undertreatment and overtreatment, focusing on therapeutic efficacy while not neglecting complications and quality of life. Therefore, it is urgent to carry out a large observational study on elderly patients with bladder cancer and conduct clinical management in a scientific way.
Supplemental Material
Supplemental material - Impact of Age at Diagnosis of Bladder Cancer on Survival: A Surveillance, Epidemiology, and End Results-Based Study 2004-2015
Supplemental material for Impact of Age at Diagnosis of Bladder Cancer on Survival: A Surveillance, Epidemiology, and End Results-Based Study 2004-2015 by Wu Lin, Xuming Pan, Bochun Ye, and Jia Song in Cancer Control
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Zhejiang Medical and Health Science and Technology Project (2022KY926); Zhejiang Traditional Chinese Medicine Science and Technology Project (2023ZL440).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.