
Abstract
Background
Scarce data exist about colorectal cancer (CRC) presentation and outcomes in Lebanon. The aim of this study is to describe the characteristics of Lebanese patients diagnosed with colorectal cancer, particularly the method of detection, age of onset, stage at presentation, treatment modalities, and survival.
Methods
This is a retrospective study of a cohort of patients with CRC, diagnosed between 2005 and 2010, admitted to 6 major university-affiliated medical centers in Lebanon.
Results
The total sample consisted of 586 patients (median age: 64 years; M:F ratio: 1.25). The most common presenting symptoms were changes in bowel habits, abdominal pain, and blood per rectum. Only 3% had been diagnosed by screening colonoscopy. Of the patients diagnosed with CRC younger than 50 years of age, 72.5% had a positive family history (P = .07). More than two-thirds of patients had an advanced stage of the disease III and IV at presentation. The Kaplan–Meier–estimated survival rate was 0%, 44.5%, 70.2%, and 78.5% for those with stage IV, III, II, and I, respectively (P = .0001), and did not vary by age nor gender of the patient. There was no differential in survival estimate for patients with stage II and III by number of chemotherapy cycles received. However, there was a significant difference in median survivorship for patients with metastatic stage IV disease; those who received less than or equal to 9 cycles had a median survivorship of 2 years (CI: 1.31–2.68) compared to 4 years (CI: 2.36–5.63) for those who received more than 9 cycles (P = .047). The cox regression showed while controlling for age and gender that patients diagnosed at stage IV had a hazard ratio of 8.81 (3.20–24.22) compared to those who were diagnosed at stage I (P = .047).
Conclusions
Lebanese patients affected by colorectal cancer tend to present with advanced disease stages, leading to poor prognosis and survival.
Keywords
Background
Colorectal cancer (CRC) is one of the most common cancers worldwide, with higher incidence in developed countries (60% of reported incident cases). CRC is more common among men than women (rate ratio: 1.4:1). 1 Survival from CRC depends on the stage of disease at diagnosis and response to treatment. 2 CRC has a 5-year survival rate exceeding 90% for stage I, as opposed to less than 15% for stage IV, a clear testimony to the importance of early detection. Despite the relatively high survival rate, CRC is the second-to-third leading cause of cancer-related deaths in developed countries such as the United States.3,4 Surgery is one of the important modes of treatment, including primary colorectal resection as well as resection of metastatic lesions from liver and/or lungs, along with neoadjuvant and adjuvant chemo- and radiotherapy.5,6
Lebanon is a Middle Eastern middle-income country with a population of about four million that experienced a protracted civil war for almost two decades, from 1975–1990. 7 Collection of demographic and surveillance data in Lebanon has long been impeded by political and organizational obstacles. The National Cancer Register (NCR), established in 1995, did not become operational until 2002. Notifications of cancer cases became mandatory through a passive system where the diagnosing physician routinely completes and forwards a standard form to the NCR. Data collected through passive reporting are complemented by active collection of case reports gathered from histopathology and hematology laboratories. NCR annual reports typically rank this type of cancer second in women after breast cancer and fourth in men. On average, 630 new cases of CRC are diagnosed annually, with a slow upward trend noted since the inception of the NCR. 8 Colorectal cancer in Lebanon ranks second among all cancers: fourth in men after prostate, lung, and bladder cancer, and second among women after breast cancer. The age-adjusted incidence rate for CRC was 25.1 for men and 20.6 for women per 100,000. In 2015, CRC constituted 16.9% of all registered incident cases of cancer in Lebanon, 55.6% among males and 44.4% among females. The mean age of diagnosis was 61.5 years among men and 62.9 years among women.
Data on the stage of CRC at presentation, quality of life after diagnosis, and survival or outcome are lacking from Lebanon’s NCR. The Lebanese Ministry of Health (MOH) has recently published national guidelines for early detection of CRC, based primarily on non-invasive fecal immunological assays, leading to a subsidized system for comprehensive care of CRC patients. 9
The aim of this study is to describe the characteristics of Lebanese patients diagnosed with CRC and their continuum of care through treatment modalities to survival or death. The effect of demographic characteristics and stage at presentation on the survival of CRC patients has been assessed. This epidemiological analysis and the computation of survival rates presented here are done for the first time in Lebanon. It will provide vital data needed to support the recent screening recommendation, not yet implemented across the board in Lebanon, and to advance policies on reimbursement and treatment cost for future years. This may also serve as benchmarks for similar research in the neighboring Arab countries.
Methods
Study Design and Sampling
This is a retrospective study of a series of CRC patients diagnosed between 2005 and 2010 in six major hospitals in Lebanon who agreed to participate in the study. Four hospitals are located in the capital city Beirut
The study-retrieved charts of all inpatients with ICD-10 diagnostic codes C18–C20, which cover colon, recto sigmoid, and rectal cancers. The paper charts of the above-identified cases were reviewed in order to select eligible patients who fulfilled the following study inclusion criteria:
1. Charts Started in the Period 2005–2010
2. Primary Cancer Histologically Confirmed
3. Cancer Invasive at Diagnosis
Data planned for retrieval from the medical records included patient characteristics (demographic data, prior personal and family medical history), disease characteristics (site, pathology, and clinical stage), management (surgery, chemotherapy agents, and radiotherapy), and outcomes (recurrence, follow-up, and disease-free survival).
The research team contacted all patients not reported as dead in the clinical chart in 2015 to inquire about their survival status. The treating physician secured an oral consent in Arabic from each respondent at the time of the first follow-up phone call. The study proposal was approved by the Lebanese American University (LAU) Institutional Review Board (IRB), as well as the IRBs of all participating hospitals.
Statistical Analysis
All analyses were conducted using the Statistical Package for Social Sciences (SPSS; version. 27). Categorical variables were presented as frequencies and percentages, and continuous variables as means, medians, and standard deviations (SD). The chi-square test was used to assess differences in proportions of categorical variables. Survival curves were generated using the Kaplan–Meier method, using the log-rank test to assess differences in survival between various sub-groups. Statistical significance was set at P-value ≤ .05. Multivariate analysis was performed using the Cox hazard regression model.
Results
Demographic Characteristics
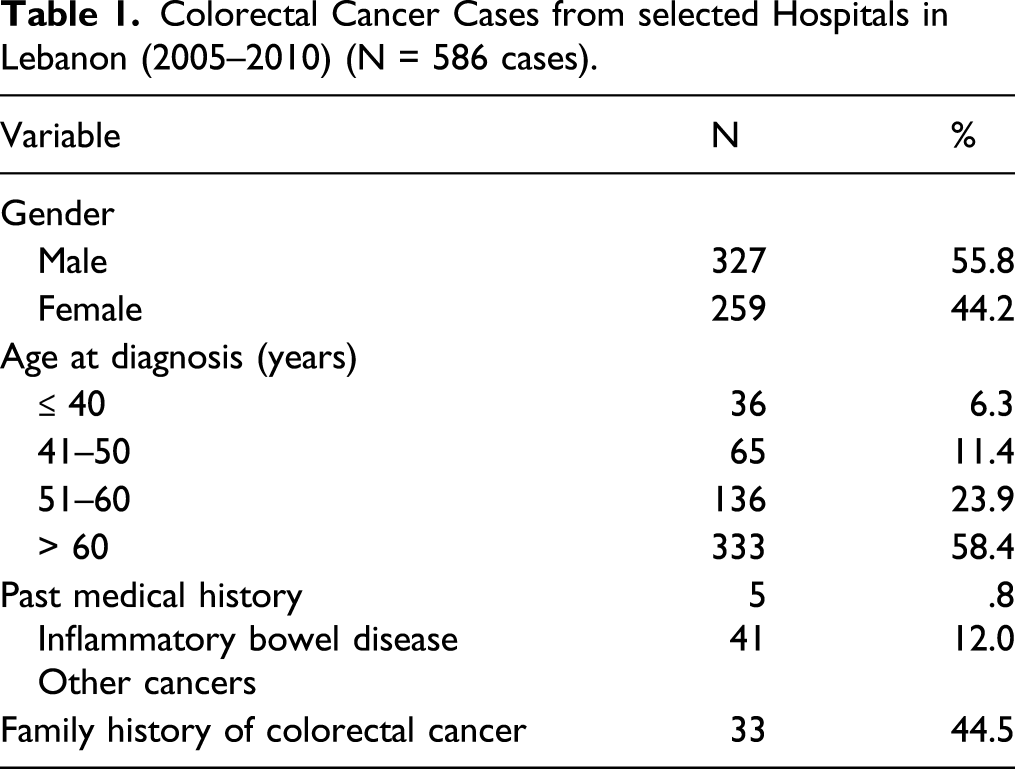
Colorectal Cancer Cases from selected Hospitals in Lebanon (2005–2010) (N = 586 cases).
Clinical Characteristics
The number of patients with rectal cancers was 83 out of the total sample of patients. Table 1 shows that 41 patients reported to have had other cancers; among those, only 19 patients had the type of other cancer specified in their medical chart. The cancer types recorded included leukemia, breast, lung, prostate cancer, and one case of cholangiocarcinoma.
The most frequently reported presenting symptom was “change in bowel habits” followed by abdominal pain and blood per rectum (Figure 1). The most frequent site of involvement was the sigmoid (35.6%), followed by the rectum (25%). Histological confirmation was done via colonoscopic biopsies (92.7%) or CT-guided biopsy (4.7%). Diagnosis following incidental colonoscopy was reported among only 3% of CRC patients (Figure 2). . Survival curves by stage of diseases at time of diagnosis. Distribution of presenting symptoms for colorectal cancer among all patients.

Tumor differentiation by TNM clinical classification showed that 6.2% of patients had stage I CRC (n = 23); 20.6%, stage II (n = 77); 36.6%, stage III (n = 137); and 36.6%, stage IV (n = 137). Primary metastases were observed among 35.1% of the patients at the time of diagnosis. About 60 patients underwent a KRAS testing as this test had not been introduced in Lebanon until 2008. Of those with test results, 39 had a wild gene and 13 a mutated gene. Complete pathological characteristics of the tumors were not uniformly entered in all the medical records. Vascular invasion was mentioned in 35.5% out of 366 records, micro-perforation in 47% out of 340 records, and positive surgical margins in 5% out of 358 records.
Management Modalities
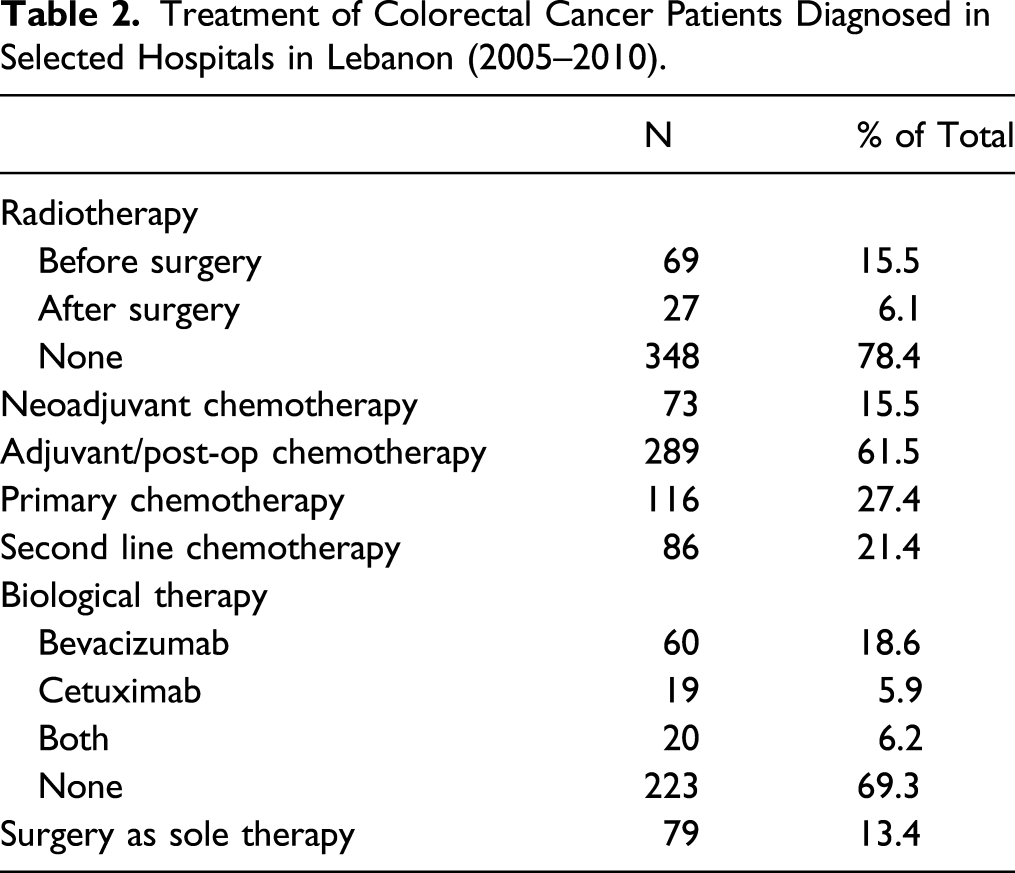
Treatment of Colorectal Cancer Patients Diagnosed in Selected Hospitals in Lebanon (2005–2010).
Survival Analysis
The median follow-up for our CRC patient cohort was 6 years with a 95% confidence interval of (4.61–7.38). The overall survival was 23.8% within a 10-year follow-up period, with significant differences related to the tumor stage at time of diagnosis. Survivorship with stage IV was 0%, 44.5% with stage III, 70.2% with stage II, and 78.5% with stage I (P-value < .001). The mean survival time in years was 8.37 for stage I, 7.35 for stage II, 5.94 for stage III, and 2.3 for stage IV (Figure 1). There was no significant difference in the survival rates by age nor gender of the patient.
The relationship between receiving the optimal number of cycles for adjuvant or neoadjuvant therapy and CRC survival rates by disease stage was also explored. For patients categorized as stage II and III, there was no significant difference in median survival by number of cycles using as a cut-off point less or equal to 4 (median 6.8 years CI (5.39–8.22)) and more than 4 cycles (median 6.53 years CI (5.94–7.13); P-value = .935). (Figure 3A). Survival curves by number of treatment cycles for patients with stage II and III. (B) Survival curve by number of treatment cycles for patients with stage IV.
For patients with metastatic cancer stage IV, there was a significant difference in median survival by number of cycles using as a cutoff point less or equal to 9 [median 2 years CI (1.31-2.68)] and more than 9 cycles [median 4 years CI (2.36-5.63)]; P-value= .047 (Figure 3B).
Hazard Ratio (HR) of the Probability of Dying by Stage of Colorectal Cancer, Gender, and Age of the Patient.

*Significant P-values.
Discussion and Conclusions
CRC incidence in Lebanon is expected to increase due to the slow aging of the population.11-13 The disease presents with few differences in Lebanon compared to more advanced nations. The disease occurrence in men is similar to what has been reported in the United States and worldwide. 1 The relative annual proportion of CRC in Lebanon is similar to the USA (≈8% of all incident cancers). However, the average age at diagnosis is significantly younger in Lebanon compared to the United States. The average age at diagnosis for men is 68 and for women is 72 in the United States, while in Lebanon, it is 65 in females and 66 in male. CRC can occur in young adults and teenagers, but the majority of CRC occur in people older than 50. Recent studies are showing that the CRC incidence rate for ages 20–49 was 9.3 per 100,000 in 1975 and now is up to 13.7 per 100,000 in 2015, a percentage change of 47.3%, whereas incidence rates in age groups 50 years and above have steadily decreased.14,15 Cases among those less than 60 years old represent 10% of the US cases vs more than 40% in Lebanon.3,8 This can be largely attributable to the younger-age distribution of the population in Lebanon. 7 However, differences in cultural and lifestyle risk factors should also be explored.16,17 On the other hand, age-specific incidence rates show that the peak is in fact reached later than elsewhere. 8 This is probably linked to the traditional Lebanese diet, rich in fibers and anti-oxidants and the calcium-rich hard drinking water predominant in the country, two protective factors contributing to delaying progress to CRC. 18 Those factors should be actively maintained, while risk factors, such as sedentary lifestyles, obesity, and increased daily intake of red meat, should be prevented and controlled.19,20
The current study indicated that sex and age at diagnosis did not affect the survival outcome. Findings confirmed that the stage at diagnosis is a major determinant of better prognosis. Data from the US published in 2018 by the American Cancer Society show that the 5-year survival rate of people with localized stage colorectal cancer is 90%. About 39% of patients are diagnosed at this early stage. If the cancer has spread to surrounding tissues or organs and/or regional lymph nodes, the 5-year survival rate is 71%. If the cancer has spread to distant parts of the body, the 5-year survival rate is 14%. However, for patients who have just one or a few tumors that have spread from the colon or rectum to the lung or the liver, surgical removal of these tumors can eliminate the cancer, which greatly improves the 5-year survival rate for these patients. 20
Of concern in our data from Lebanon is that about 75% of cases are seen initially at already advanced stages, which automatically reduces their survival likelihood, especially if the treatment is not very aggressive. There is some evidence in the literature regarding the beneficial effects of aggressive chemotherapy and surgical management. 21 In this analysis, metastasectomy to treat the metastasis to the lungs or the liver was rarely performed. Reasons for under-performance may include lack of clear national guidelines and possibly lack of awareness among practitioners regarding the positive impact of such an intervention on the disease prognosis. It should be noted that the management of cancers in Lebanon is not subject to local guidelines and often relies on the NCCN, ASCO, or ESMO guidelines.
There are several limitations to our study inherently related to the retrospective nature of the data collection. The main limitation of the study regarding the overall survival of CRC patients in Lebanon is that the specific characteristics of type of treatment, adverse effects, and lines used, as well as the pathological characteristics of the tumors 22 in different hospitals were not consistently recorded in all the medical charts. This is a main drawback of retrospective data; however, it is worth noting that the type of cancer treatment is pretty uniform in the hospitals included in our review. Actually, oncologists affiliated to teaching hospitals in Lebanon do follow the same protocol for CRC treatment. Moreover, the Lebanese Ministry of Public Health is the main distributor and provider of cancer medication in the country. The strength of this study includes the adequate follow-up to ascertain the survival status of the patient and detailed information on cancer stage. Our study also contributes to the scarce follow-up literature on CRC survival in Lebanon and the Arab countries.
In conclusion, the cost of covering invasive confirmatory tests such as colonoscopy must be weighed against the increasing costs of anti-cancer drugs in general and with more severe stages in particular. 23 Similarly, the adoption of a national set of treatment modalities including the number of chemotherapy cycles for those with locally advanced disease stage II and III vs metastatic disease stage will undoubtedly contribute to a better prognosis of CRC patients in Lebanon.
Footnotes
Acknowledgments
We are very grateful to Mr. Abed Sabra from Roche International for his kindness and constant support. Our special thanks for Dr. Roger Khater, Dr. Fadi Farhat, Dr. Nabil Chamseddine, and Dr. Walid Moukadem for their contribution to data acquisition from their respective hospital records. We acknowledge with gratitude the effort of Ms. Mariana Salamoun in data entry and data analysis. We are also extremely grateful for the valuable contribution of Ms. Sarah Assad to survival data analysis.
Author Contributions
All authors listed have contributed sufficiently to the project to be included as authors, and all those who are qualified to be authors are listed in the author byline. RC and MD contributed to the study conception and design; RC, JM, AM, GN, LN, ES, and MD contributed to data collection, data analysis, and interpretation and writing of the article; MD performed and supervised all the statistical analysis; all authors contributed to editing, reviewing, and final approval of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: F. Hoffman-La Roche funded the research. The funding body was not involved in the design or conduct of the study, collection, management, analysis or interpretation of data, preparation, or review of the article.
Ethical Approval and Consent to Participate
The follow-up data on CRC patients survival status were collected through phone calls by the authors of the articles as interviewers, and data were gathered only from those who consented orally. The Lebanese American University Institutional Review Board (IRB) committee reviewed and approved the study. The article entails original research and has not been submitted / published earlier in any journal and is not being considered for publication elsewhere. The article has been submitted with full responsibility, following due ethical procedure, and there is no duplicate publication, fraud, plagiarism, or concerns about animal or human experimentation.
Consent for Publication
Not applicable
Data Availability
The data set used and analyzed during the current study is available from the corresponding author on reasonable request.