
Abstract
Background
Pediatric cancer significantly affects the quality of life (QOL) of patients and their families/caregivers particularly in low-income countries where there is scarcity of resources. Thus, the purpose of this study was to evaluate the QOL and associated factors among family/caregivers of pediatric patients treated for cancer at Tikur Anbassa Specialized Hospital (TASH), Addis Ababa, Ethiopia.
Method
An institution-based cross-sectional study design was used to collect information from family/caregivers who were present in the pediatric oncology unit at TASH from January 2, 2023 to May 30, 2023. The validated Amharic version of the caregiver oncology quality of life questionnaire (CarGOQOL) was used to collect the data. A random sampling technique was applied to select the study participants. The descriptive and regression analysis were conducted using statistical software SPSS version 27.0.
Results
A total of 350 family/caregivers answered the questionnaire. The overall response rate was 82.7%, and about 55% of the respondents were women. Among the participants, under-35 age made up the majority (60.9%). About 81% of family/caregivers were parents, and 77.7% of family/caregivers were married. More than half of the participants have at least a secondary level education. In addition, about two-thirds of the participants (63%) live in rural areas. Furthermore, more than half of the participants generate less than $17.86 per month. Nearly fifty percent of family/caregivers of pediatric cancer patients had poor QOL. The finding showed that widowed family/caregivers (AOR:5.59, 95%CI: 1.12, 27.79, P-value: 0.03) had poor QOL as compared to married, and those with a monthly income of between $17.87- $89.29 were less likely to have poor QOL compared to those with an income below <$17.87 (P-value: 0.01).
Conclusion
In the current study, poor QOL was high among family/caregivers of pediatric cancer patients. Being widowed and lowest income were significantly associated with the QOL of the caregivers of pediatric patients with cancer.
Plain language summary
Pediatric cancer affects not only the quality of life of cancer patients but also their families/caregivers. The disease significantly affects the financial, social, physical, and emotional obligations of the caregivers of cancer patients. This problem is highly prevalent in low-income countries where resources are scarce. Thus, this study aimed to evaluate the quality of life (QOL) of family caregivers of pediatric patients and associated factors. The study was conducted at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, between January and May 2023. Caregivers in the pediatric oncology unit participated in a survey conducted using the validated Amharic version of the caregiver oncology quality of life questionnaire (CarGOQOL). Participants were selected randomly, and the data were analyzed using the statistical software SPSS. A total of 350 caregivers answered the questionnaire with a response rate of 82.7%, and 55.1% of them were women. Among the participants, those under 35 years of age made up the majority (60.9%). About 81% of caregivers were parents, and 77.7% were married. More than fifty percent of the participants have at least a secondary-level education. In addition, about two-thirds of the participants in this study (63%) live in rural areas. Furthermore, more than half of the participants generate less than $17.86 per month. Nearly fifty percent of caregivers of pediatric cancer patients had below the average QOL. The finding showed that ethnicity, marital status, level of education, and monthly income were significantly associated with the caregiver's QOL. Overall, in this study, a significant number of family/caregivers of pediatric cancer patients had below average QOL. Marital status, educational level, and income were positively associated with low QOL.
Introduction
The World Health Organization (WHO) estimates that 400,000 children diagnosed with cancer each year and around 10 million cancer-related deaths in the year 2020 worldwide. 1 More than 80% of pediatric cancer occurs in developing and low income countries.2,3 Around 42900 pediatrics age group 0-19 years old develop cancer every year. The 5-year survival rate is >80% and <30% for pediatrics in high income countries (HIC) and low-income countries (LIC), respectively. Survival rate increase even for the lethal type of cancers in HIC. 4 The major reason for the high mortality rate and poor survival rate recorded in LIC is due to delayed diagnoses, inadequate access to trained specialists, and high cost of cancer treatment. 5
Ethiopia’s health care system operates on a tiered structure comprising primary, secondary, and tertiary levels, with the majority of the population relying on under-resourced primary care facilities, especially in rural areas where over 85% of people live. The country faces significant challenges, including a shortage of health care professionals, limited infrastructure, geographic and financial barriers, and inadequate integration of palliative care, all of which disproportionately affect family/caregivers of pediatric cancer patients. Despite some health care subsidies, out-of-pocket expenses remain high, exacerbating the financial burden on family/caregivers, many of whom earn less than 1000 ETB (∼$18) per month. Ethiopia’s GDP is approximately $135 billion (2024), with a per capita income of $1,150, reflecting widespread poverty, particularly in rural areas, where access to education and health care is limited. Urban-rural disparities, low public health spending (5%–6% of GDP), and limited literacy rates (51%) further hinder family/caregivers’ ability to navigate health care systems, manage stress, and support their patients effectively.6-8
The most common type of cancer seen in Ethiopia children are leukemia, lymphoma, retinoblastoma, bone, and soft tissue sarcomas. 9 This disease and its management practice have an impact on the quality of life (QOL) of the patients.10,11 Cancer affects not only the patients’ QOL and also the caregiving person’s QOL from different perspectives. 12 Studies conducted on family caregivers of cancer patients showed that more than half of caregivers quit their work or made major life changes to provide care for the 1 they love, lost most of their savings because of diagnosis and treatments, and lost their main source of income. 13 Psychological distress could also be commonly reported among family/caregivers, particularly those caring for patients with advanced diseases like cancer and others. 14 Additional burden variables that affect the QOL of family/caregivers include requiring caregiving assistance, inability to function normally, and altered educational plans. 13
There are also other different factors that affect the QOL of caregivers. These include relationship to the patient, marital status, ethnicity, social support, the health status of the caregiver, types and clinical characteristics of the disease, and progression of the disease.15-18 The assessment of caregivers QOL and the factors associated with it helps to understand the magnitude of the problem and identify the associated factors to provide appropriate intervention. There are different tools used for the assessment of caregivers QOL. Caregiver oncology quality of life questioner (CarGOQOL) is 1 of among commonly used, validated self-completed multi questionnaires with 29 item questioner and 10 dimension assessments (psychological well-being, burden, relationship with health care, administration and finance, coping, physical wellbeing, self-esteem, leisure time, social support and private life).19,20 Family caregivers’ QOL, as well as their health, are significantly impacted by cancer. The QOL of Ethiopian parents who care for children with cancer is not widely recognized yet and no study has been far conducted regarding the assessment of QOL and factors affecting the QOL of caregivers of pediatric cancer patients.
Methods
Study Design and Population
The cross-sectional study design was applied from January 2, 2023 to May 30, 2023 over 5 months. The study was conducted at Tikur Anbassa Specialized Hospital (TASH) pediatric oncology center in Addis Ababa, Ethiopia. TASH is 1 of the largest referral hospitals with more than 700 beds and around 26 beds serving pediatric oncology centers. Annually, TASH receives between 500 and 600 pediatric cancer patients. Since 2010, TASH was the only cancer referral center in Ethiopia with few oncologists to serve the entire country and there was no cancer registry exists yet. 9 The source population was all family/caregivers providing care for pediatric patients in the pediatric oncology center at TASH during the study period. The study population was all caregivers who fulfilled the inclusion criteria, defined as a family member by patients and are responsible for cancer patients, and who spent much of his or her time with cancer patients and caregivers who were available during study periods of January 2 to May 30, 2023 at TASH pediatric oncology center. The inclusion criteria for this research were family/caregivers who were above 18 years old, volunteer for an interview, caregivers who could speak and listen the Amharic language, and were available during the study period.
Sample Size Determination and Sampling Techniques
A sample size was computed based on a single proportion formula, assuming the good QOL a prevalence (P) of 50% as follows, as there was no research conducted on this topic in Ethiopia and neighboring countries. ➢ ➢ ➢ ➢ Percentage confidence level (1.96)-

Considering non-response, a 10% contingent was added and 423 participants were targeted for the current study. A systematic random sampling technique was employed, with all caregivers present in inpatient wards and outpatient clinics awaiting follow-up included in the sampling frame. The sampling frame was organized daily, separately for inpatients and outpatients, and sorted alphabetically by surname (A to Z). The first caregiver was selected using a lottery method. Over a 3-month data collection period (∼60 working days), approximately 7 participants were selected and interviewed each day, ultimately reaching a total of 423 study participants. In random sampling techniques, every single caregiver in the sampling frame has a known and non-zero chance of being selected into the sample. 21
Data Collection and Management
Data were collected using a standardized questionnaire developed by reviewing different literature and validated CarGOQOL. The questionnaire has 2 sections. Section I contains the socio-demographic characteristics of caregivers as well as the clinical and treatment-related characteristics of the patients. Section II was for the caregivers’ QOL questionnaire a CarGOQOL to measure the caregivers of pediatric cancer patients QOL. The CarGOQOL had domains to assess the physical, psychological, and sexual life impact as well as family and friend support.
The CarGOQOL is a 29-item questionnaire. Each item is rated on a 5-point Likert scale (1 – “Never/Not at all”, “2 – Rarely/A little”, “3 –Sometimes/Somewhat”, “4 – Often/A lot”, and “5 – Always/Very much”) with higher scores generally indicating better QOL across domains. Scores are calculated for each item in the domain (psychological well-being (4 items), Burden (4 items), relationship with health care (3 items), administration and finance (3 items), physical well-being (4 items), coping (3 items), leisure time (2 items), self-esteem (2 items), social support (2 items), and private life (2 items)) as well as an overall QOL score. For items that were negatively worded (ie, where higher scores reflect poorer QOL), the responses were reverse-scored before calculation to ensure consistency, so that higher scores uniformly indicate better QOL. The CarGOQOL score is then computed by summing the responses across all items. Finally, scores are categorized based on their deviation from the mean: Good QOL for scores above the mean and Poor QOL for scores below the mean.
The tool, the validity and reliability of the Amharic version of CarGOQOL was assessed. The CarGOQOL is a valid and reliable tool that is widely used, reliable and valid tool for clinical trials and intervention programs to assess QOL in family/caregivers of cancer patients. The CarGOQOL was translated into Amharic using a rigorous forward-backward translation process. Initially, an expert with extensive experience in cancer care and translating psychometric tools into Amharic translated the CarGOQOL from English to Amharic. To verify the translation’s accuracy, a back-translation to English was conducted by a senior consultant oncologist and oncology researcher, who were unfamiliar with the original English version or the research objectives. The translation was then reviewed by 2 senior oncologists and 2 senior researchers, all fluent in both English and Amharic, to ensure consistency, cultural appropriateness, and the tool’s validity for use in the Ethiopian context. Moreover, the reliability of the instrument was examined using Cronbach’s alpha level. The overall Cronbach’s alpha value of the 29 items resulted in 0.833 and with each domain.
A pretest was conducted on 5% of the study population and feedback was considered, and necessary changes were made to the data collection questionnaire. The training was given to the data collectors on the process and how they handle any issue occurring during data collection. Daily, the principal investigator (PI) was closely supervising the data collection process. Then evaluated for the correctness of the filled questionnaire and recorded information at the end of each data collection day to guarantee its accuracy. Even though a total of 423 participants were targeted for the study, only 350 participants were included in the final analysis (Figure 1). Flowchart of participant selection and data inclusion process.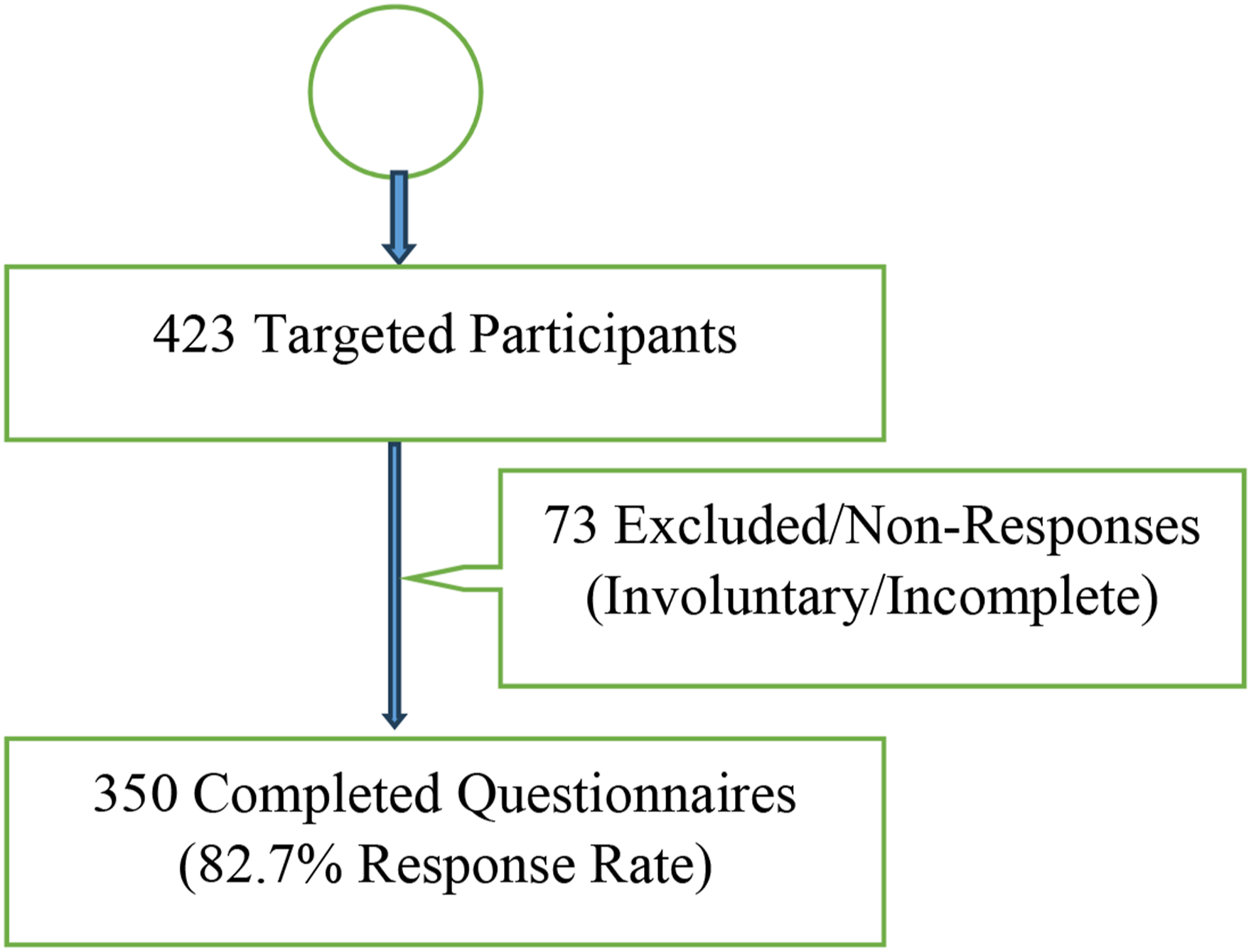
Data Processing and Analysis
The collected data were converted to word excel to clean up the data manually and the collected data was further cleaned, entered, and analyzed by using the Statistical Package for Social Science (SPSS) version 27.0 software. Descriptive statistics were used to summarize the data and logistic regression analysis to determine factors affecting the QOL of family/caregivers of pediatric cancer patients. P-value <0.05 was used to declare a statistically significant association between dependent and independent (predictor) variables. The reporting of this study conforms to STROBE guidelines. 22
Ethical Consideration
The ethics review board of the School of Pharmacy, Addis Ababa University approved the study (Reference number: ERB/SOP/476/15/2023). Information was obtained from each participant after the purpose of the study was explained to the respondent and getting their informed verbal consent. Confidentiality of the information was assured, and privacy of the respondents was maintained. Voluntary participation or withdrawal was ensured at any time without any negative consequence. The raw data were collected without identifiers, were accessible only to the researchers, and were disseminated solely in aggregate form.
Results
Socio-Demographic Characteristics of Caregivers of Pediatric Cancer Patients
Socio-Demographic Characteristics of Caregivers of Pediatric Cancer Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia (N = 350).

Note: SD-standard division; % (percent); N-number of caregivers; ETB: Ethiopian Birr; USD ($): United States Dollar; Other♦: apostles, Catholics, atheists, Adventists and Waqefecha, Other◘: Gurage, Sidama, Walayta, Harar, konso and Gambella; Other©: Gospel preachers, singers, swimming and sports trainers, housewives; Otherº: uncles, aunts, relatives, grandparents, and supporters.
Clinical Characteristics of Pediatric Cancer Patients
Clinical Characteristics of a Pediatric Cancer Patient at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia (N = 350).

Note: SD = standard division, N = number of participants % = percent ALL = Acute lymphocytic leukemia, AML = Acute myelogenous leukemia, NHL = Non-Hodgkin lymphoma, HL = Hodgkin’s lymphoma, RMS = Rhabdomyosarcoma, Osteo = Osteosarcoma, Ewing = Ewing sarcoma, other♦(unspecified cancer types, abdominal related cancer and skin cancer).
Characteristics of Family/Caregivers’ Quality of Life
Characteristics of QOL of Family/Caregivers of a Pediatric Cancer Patient at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia (N = 350).

Factors Associated with the Quality of Life of Family/Caregivers of Pediatric Cancer Patients
Association of Socio-Demographic and Clinical Characteristics and QOL Among Care Giver of Pediatric Cancer Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia (N = 350).

Note: QOL = quality of life, ETB: Ethiopian Birr; $: United States Dollar, COR = crude odd ratio, AOR = adjusted odd ratio, CI = confidence interval, ref = reference, ALL = Acute lymphocytic leukemia, AML = Acute myelogenous leukemia, NHL = Non-Hodgkin lymphoma, HL = Hodgkin’s lymphoma, Others* = unspecified cancer types, abdominal related cancer, and skin cancer.
Discussion
Pediatric cancer can affect the quality of caregiver as it has on patients’ QOL. 11 Lack of medications and enough oncology centers especially in developing countries including Ethiopia increase the magnitude of the problem. The study evaluates the QOL of pediatric cancer caregivers at TASH Addis Ababa, filling a gap in literature on this topic in Ethiopia. In this study, sociodemographic characteristics of study participants such as marital status, educational level and income were associated with the QOL of the caregivers.
In current study, three-fourths of caregivers were married, lived out of Addis Ababa, and did not get financial support. In addition, most of the caregivers were female (55.1%) and most of them were under 35 years. Similarly, in the study that assessed depression among caregivers of pediatric cancer patients in TASH showed that most of the family/caregivers were married, resided out of Addis Ababa, had age between 31-35 and did not get any financial supports. 16 Other studies conducted in 6 university hospitals and national cancer centers in Korea showed most of the caregivers are females and found in age below 40 years. 13 This may be related to the division of responsibilities within the family, with females typically taking on a larger role in caregiving, while males are more commonly involved in supporting and generating the family’s income.
In current study, the prevalence of poor QOL was 48.0%. The study held in Dessie, Ethiopia also reported similar findings, 47.5%. 23 The study conducted in Indonesia reported that nearly sixty percent of caregivers of hospitalized patients had poor QOL, which is higher than the current study. 24 This difference in QOL might be attributed to different factors like the used tools to measure QOL, cultural and economic variety among different countries, and variation in sample sizes. Another study conducted in Turkey to compare the QOL of a mother with cancer children to mother of healthy children showed that mothers of cancer children had poorer QOL and psychological health than mothers of healthy children. 25 Having a cancer patient by itself affect the QOL of caregivers with different dimension including financially, economically, and psychologically. 26 This low QOL in Ethiopia may be attributed to several interconnected factors. The limited availability of health care services outside of TASH creates significant logistical challenges for caregivers, such as long travel distances and increased transportation costs. This not only adds financial strain but also reduces the time caregivers can dedicate to their personal well-being and other responsibilities. Furthermore, the concentration of services at TASH leads to an overwhelming workload for health care professionals, which can compromise the quality of care provided and increase the stress on caregivers. Additionally, the ongoing economic inflation exacerbates financial hardships, making it difficult for caregivers to access necessary resources, such as medications, and nutritional support which may also contribute to the caregivers’ poor quality of life.
The educational level is also another variable that is a significant indicator of the QOL of caregivers. Similarly in the study conducted in Ghana showed that caregivers with no formal education or only primary to junior high school education reported a notably lower health-related quality of life compared to those with tertiary education. 27 Furthermore, the findings from other studies, also suggested that higher education levels correlate with better health-related quality of life outcomes. 28 In current study, more than 1 fourth of the study participants had college and above education level. Even from those who had college and above of education nearly fifty percent had poor QOL. This is caused by a variety of factors, including financial difficulties and the fact that most of them had jobs but were slowed down by the disease. A study conducted in Korea showed that despite most caregivers being highly educated, over half were either did not have a job or had left their jobs to take on caregiving responsibilities. 18
Another variable that is highly significant to caregivers is the clinical diagnosis of patients. Leukemia, particularly acute lymphocytic leukemia (ALL) is among the dominant disease condition in the younger age and is closely associated with significant rates of mortality and morbidity. 29 Similarly in current study ALL accounts for the highest portion of clinical diagnoses. In qualitative study conducted in TASH revealed that the main causes of stress in caregivers of pediatric cancer patients are the severity of their children’s illness, the expectation of poor treatment outcomes, the unavailability of cancer treatment, and the lack of social support. 30
In this study, a lowest monthly income of the caregivers was negatively association with the QOL. Similar study also supports that monthly income of caregivers also have great impact of QOL of caregivers. 20 Other studies on economic burden and QOL of cancer patients showed most family caregivers who have poor income and poor health status plus who paid high medical expenses decrease the QOL of caregivers. 13 Similarly, in the current study, more than sixty percent of participant had lowest monthly income (<$17.86) and 32.3% of them had poor QOL. Even though the majority of the participant’s monthly income was low, most of them did not get any support. Similar study in Brazil also showed that low income highly associated with QOL of caregivers. 31 This suggests that those who provide care for children with lower monthly incomes may face greater financial (economic) hardships in managing the expense of medical care and gaining access to facilities for treatment particularly in developing countries like Ethiopia.
In current study, the socio-demographic characteristics such as age, occupation, place of residence, relationship with the patient, patient type did not appear to be related with QOL. This is in contrast to study done in other contexts, which indicated that the QOL of cancer families was influenced by factors like age, occupation, residence, relationship with patient, and patient type.20 31 The disparity could be attributed to the use of various measurement tools used for the assessment of QOL. The CarGOQOL tool was employed in the current investigation, while in other studies have measured the QOL of family caregivers using the Malay Caregiver Quality of Life scale (MCQOL), the caregiver quality of life Index–cancer (CQOLC) and Caregiver Strain Index-Malay (CSI-M).
Furthermore, even though it was less likely in the current study, other research has showed that time of caregiving, duration of treatment, clinical diagnosis and type of treatment the patient is taking have great impact on the QOL of family/caregivers of pediatrics cancer patients. 30 Extended caregiving hours and prolonged treatment periods can lead to caregiver burnout, financial strain, and emotional exhaustion. Additionally, the severity and prognosis of the clinical diagnosis, along with the complexity and side effects of treatment regimens, can further exacerbate the psychological and physical burden on caregivers, ultimately impacting their quality of life.32,33
This study revealed important findings regarding the QOL among family/caregivers of pediatric cancer patients at Tikur Anbessa Specialized Hospital (TASH). However, it is important to acknowledge the limitations. The cross-sectional design limits our ability to establish causal relationships and track changes in QOL over time. The relatively small sample size also restricts the generalizability of our findings to the wider population of family/caregivers in Ethiopia. Additionally, reliance on self-reported data introduces the potential for social desirability bias and common method variance. Despite these limitations, this study makes a significant contribution to the existing literature. To the best of our knowledge, this is the first study to investigate the QOL of family/caregivers of pediatric cancer patients specifically within the Ethiopian context. This establishes a crucial baseline for future research in this understudied area. While previous research has explored family/caregivers QOL in other countries and contexts34,35 this study addresses a critical gap by providing context-specific data for Ethiopia. For example, previous studies may have focused on factors like access to specialized care or financial resources in high-income settings, which may differ significantly from the challenges faced by caregivers in Ethiopia. This study identifies specific factors influencing QOL within the Ethiopian context, such as low education level, low monthly income, large family size, lack of job, rural residency, and lack of financial support. This context-specific understanding is crucial for developing targeted interventions and support programs. This research adds to the literature by highlighting the unique challenges faced by caregivers in low-resource settings and provides a foundation for future research exploring longitudinal trends, intervention effectiveness, and cross-cultural comparisons. These findings can inform policy and practice aimed at improving the well-being of these essential family/caregivers.
Conclusion
Overall, in the current study QOL of the family/caregivers of pediatric cancer patients was low. Marital status, educational level and income were positively associated with the poor QOL the family/caregivers of pediatric cancer patients. The findings of this study have important implications for further study and intervention as family/caregivers’ QOL has an impact on treatment outcome of the patients as well as adherence to the follow up. To address these challenges, health care policymakers in Ethiopia should prioritize reforming health care policies to incorporate comprehensive support systems for family/caregivers, including psychosocial support, financial assistance, and access to palliative care services. Furthermore, there is a pressing need to promote awareness and build capacity in rural areas where the burden is greatest. Future research should explore the development and implementation of evidence-based interventions aimed at improving family/caregivers QOL and fostering better health outcomes for pediatric cancer patients. Collaborative efforts between policymakers, health care providers, and community stakeholders are essential to creating sustainable solutions that address these pressing issues.
Supplemental Material
Supplemental Material - Quality of Life and Associated Factors Among Family/Caregivers of Pediatric Patients Treated for Cancer at Tikur Anbessa Specialized Hospital: Institution-Based Cross-Sectional Study
Supplemental Material for Quality of Life and Associated Factors Among Family/Caregivers of Pediatric Patients Treated for Cancer at Tikur Anbessa Specialized Hospital: Institution-Based Cross-Sectional Study by Zenebe Negash, Eden M. Kinfe, Urji Zerihun, and Atalay M. Fentie in Cancer Control
Footnotes
Acknowledgments
The authors would like to thank all data collectors, participants, and other staff of the Tikur Anbessa specialized hospital. The authors would also like to thank all those who helped facilitate the research and provided constructive feedback.
Author Contributions
ZN, EMK, UZ and AMF made major contributions to the reported work, including the concept and methodology of the study, execution, data collection, analysis, and interpretation; involved in the drafting, revision, or critical review of the manuscript; gave final approval of the version to be published; agreed on the journal to which the study was submitted; and accepted responsibility and accountability for the contents of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.