
Abstract
Introduction
Total pelvic exenteration (TPE) for clinical T4b colorectal cancer (CRC) is associated with significant morbidity. Short (0-30 days)- and intermediate (31-90 days)-term temporal analysis of complication onset is not well described, yet needed, to better counsel patients considering TPE.
Methods
A retrospective cohort study of consecutive patients with primary or recurrent clinical T4b pelvic CRC undergoing open TPE between 2014 and 2023 was conducted. Clinicopathologic variables were collected for each patient. Postoperative morbidity was classified according to the Clavien-Dindo (CD) grade system and stratified by time of onset within 90 days of surgery. Pearson’s Chi-square test, Fisher’s Exact test, and the Mann-Whitney U test were used to compare primary vs recurrent patient groups, and logistic regression assessed predictors of postoperative morbidity. Statistical analysis was performed using R with two-sided significance set at <0.05.
Results
Twenty-seven patients were identified of which 24 (88.9%) were male with a median age of 60.4 years (interquartile range [IQR]: 56.3-70.5). Seventeen (63.0%) patients had primary disease and 10 (37.0%) had recurrent CRC. Twenty-three (85.2%) patients experienced at least one complication within 90 days of surgery, but no mortality was observed. Ten (37.0%) patients experienced a CD ≥ 3 event, of which 40% took place beyond 30 days. The most common complication overall was anemia requiring transfusion, while the most common major complication was pelvic abscess. No clinicopathologic variables analyzed were predictive of major postoperative complication within 90 days of TPE.
Conclusion
TPE for clinical T4b CRC carries a high risk of postoperative morbidity in both the short- and intermediate-term after surgery, with a significant proportion of complications occurring after 30 days. Given the magnitude of operation, an extended recovery with high risk for complications is common. Although a single-center series, this annotated postoperative complication profile may assist patients and clinicians when reviewing informed consent for TPE.
Introduction
Colorectal cancer (CRC) is the third most common cancer globally and the second most common cause of cancer death. 1 For locally advanced or recurrent tumors, extended resection including exenteration may be necessary to obtain a complete, negative surgical margin for curative intent. 2
Total pelvic exenteration (TPE)—which encompasses en-bloc removal of the entire pelvic viscera including the bladder, anorectum, and reproductive organs—was first reported by Brunschwig in 1948. 3 Perioperative mortality in pelvic exenteration procedures has improved drastically since the first case series, now consistently less than 2% reported in multi-institutional investigations.4,5 Despite its high absolute risk, perioperative morbidity has similarly improved with advancing surgical technique and peri-operative care. 6 In the last 20 years, the reported rate of major complications has decreased from around half of patients undergoing pelvic exenterations,2,7 to approximately one in three patients.4,5,8,9 Given the risk for severe morbidity following pelvic exenteration, contemporary disease specific studies may best provide physicians and patients with accurate complication profiles to provide an informed operative consent.
The objective of the present study is to provide a contemporary, annotated postoperative risk profile of TPE in CRC patients. The type and extent of major complications taking place within 90 days of TPE were captured, to further characterize longer-term peri-operative morbidities. Secondarily, we explored clinical and treatment related variables association to major postoperative complication events.
Methods and Materials
Study Design
On April 27th, 2023, the Advarra IRB reviewed the study proposal and determined that the investigation was exempt from IRB oversight given the Department of Health and Human Services regulations outlined in 45 CFR 46.104(d)(4) (IRB# 00000971). Subsequently, a retrospective cohort study of consecutive patients with either primary or recurrent clinical and or radiographic T4b CRC who were treated at a single tertiary care center between 2014 and 2023 was conducted. T4b encompassed invasion into secondary genitourinary and or gynecologic organs. 10 Similar to previous investigations, the study defined TPE as the collective removal of the bladder and rectum, prostatectomy or hysterectomy salpingo-oophorectomy, and pelvic lymph nodes. 11 Importantly, limited anterior or posterior two compartment resections were not included in the study. Study size was driven by patients who met this eligibility criteria. The primary outcome of the study included postoperative complications, both in the short (0-30 days)- and intermediate (31-90 days)-term following surgery. Secondary outcomes of the study included recurrence free survival (RFS) and overall survival (OS) following TPE. Of note, the reporting of this study conforms to STROBE guidelines. 12
Data collection was performed between July and October of 2023. For each patient, relevant clinicopathologic characteristics were collected from electronic chart review including surgical history (e.g., preoperative fecal or urinary diversion), preoperative lab values, American Society of Anesthesiologists (ASA) classifications, neoadjuvant therapies, intraoperative metrics, and pathologic disease features. Each postoperative complication within 90 days of operation was documented and classified both by time of event (i.e., short term or intermediate term) and the Clavien Dindo (CD) grade system. 13 In the present study, those complications graded 3a and higher were defined as major. Identification and classification of complications was validated by two independent, blinded abstracters. Discrepancies on complication grade were reconciled with a third reviewer. Data concerning disease recurrence dates, vitality status, date of death if applicable, and follow up were also recorded. Date of last follow up was defined as the last date in which the patient was seen in office or the hospital. Following data collection, all patient data were de-identified prior to analysis to ensure anonymity.
Surgical Technique
The open TPE surgical technique employed by the surgeons at the study institution has previously been described by our group. 11 In accordance with modern recommendations, each procedure was conducted with a multidisciplinary team of providers including a urologist, colorectal surgeon, and frequently a plastic surgeon. 14
Statistical Analysis
Statistical analysis was performed using R (version 2023.06.0+421) with a two-sided level of significance of 0.05. The patient cohort was summarized using descriptive statistics. Median measures were provided for continuous variables while frequency counts were displayed for categorical data. Pearson’s Chi-square test was used to compare categorical variables between primary and recurrent groups—for observed counts less than five, Fisher’s exact test was employed to compare groups. Alternatively, the Mann-Whitney U test was applied for comparison of non-parametric, continuous variables. Additionally, clinical and pathologic characteristics of patients experiencing a CD ≥ 3 complication were compared to those with CD < 3 complications using logistic regression analysis. Subsequently, a limited multivariable logistic regression analysis was performed, accounting for the small sample size, to identify significant predictors of perioperative major complications. Separately, overall survival and recurrence free survival were estimated with Kaplan Meier (KM) analysis.
Results
Clinicopathologic Characteristics
Baseline Clinicopathologic Data for 27 Clinical T4b CRC Patients Undergoing TPE.

aPercents add up to greater than 100 due to combined organs of invasion.
IQR = Interquartile range. TPE = Total pelvic exenteration.
Perioperative Data for 27 Clinical T4b CRC Patients Undergoing TPE.
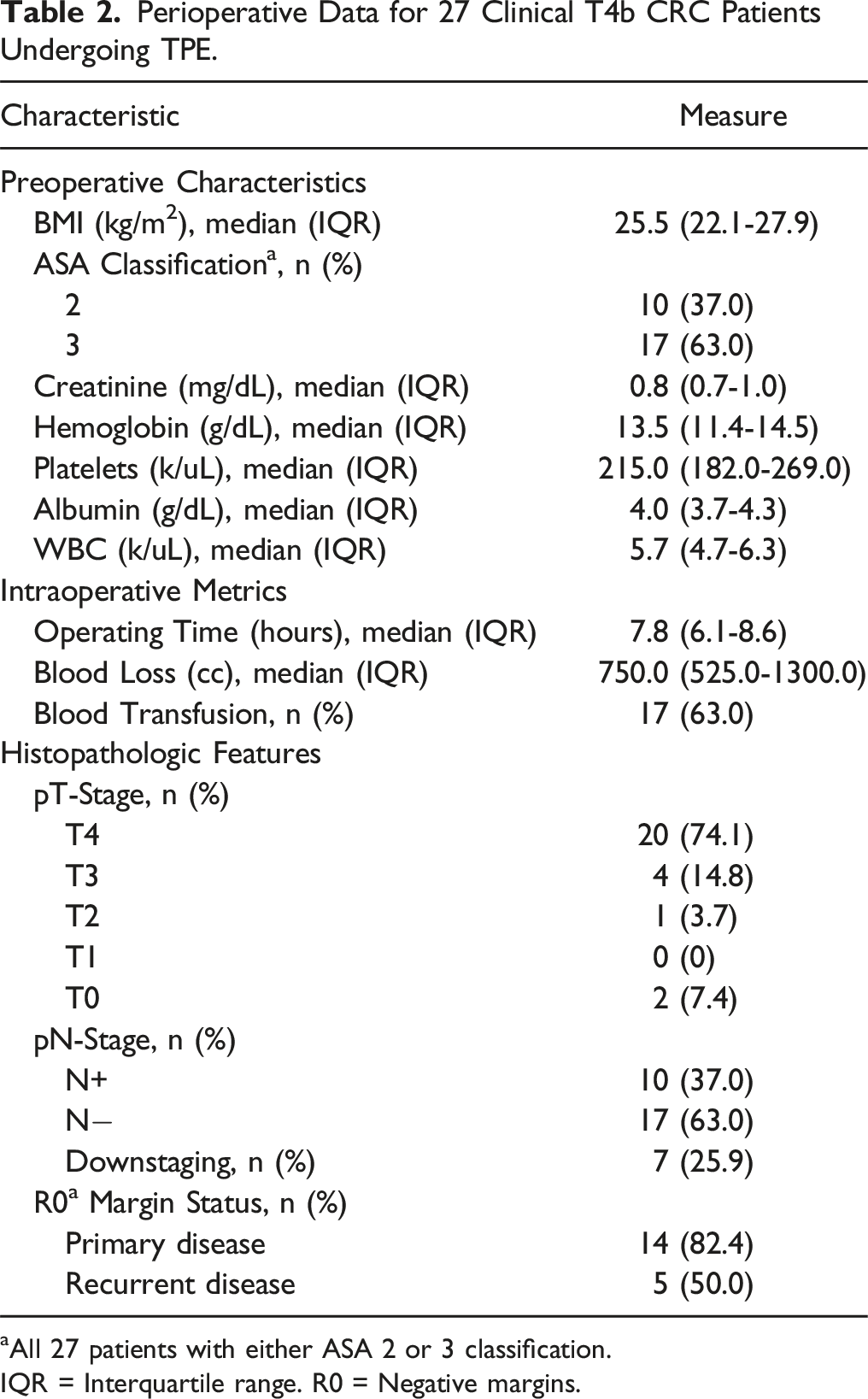
aAll 27 patients with either ASA 2 or 3 classification.
IQR = Interquartile range. R0 = Negative margins.
Histologically, 20 (74.1%) patients had pT4b disease, 4 (14.8%) T3 disease, 1 (3.7%) T2 disease, and 2 (7.4%) pT0, indicating 7 (25.9%) patients experienced pathologic downstaging. All patients with pathologic downstaging had primary disease prior to TPE and underwent neoadjuvant chemotherapy and radiation. Among patients with histological T4b disease, the prostate (n = 17) and bladder (n = 10) were most commonly invaded. Pathologic nodal disease was present in 10 (37.0%) patients. The margin was microscopically positive (R1) in 8 (29.6%) patients, of which 5 were recurrent tumors and 2 did not receive preoperative radiation therapy. Nineteen (70.4%) patients had moderately differentiated disease, 4 (14.8%) had poorly differentiated disease, and 4 (14.8%) were unable to be assessed.
Postoperative Course and Complications
The median index length of stay was 9 days (IQR: 7-12). During the study period, 9 (33.3%) patients were readmitted within 90 days following initial discharge. In total, 23 (85.2%) patients experienced at least one complication within 90 days of their operation (Figure 1). Stratification of all complications by time of event revealed that 79.2% and 20.8% of these complications occurred within 0-30 days or 31-90 days postoperatively, respectively. The median number of complications experienced by any patient was 2 (IQR: 1-3) and there was no difference between those with recurrent CRC and those with locally advanced primary CRC (P = 0.9). See Supplemental Table 1 for a detailed list of complications experienced by each patient. Total number of complications experienced by each patient, stratified by CD grade. Four patients (3, 18, 25, and 26) did not experience any CD complication.
Of those experiencing any complication, 10 patients (37.0%) had a major CD complication (Figure 1) with 5 (18.5%) requiring a reoperation within 90 days of TPE. See Supplemental Table 2 for a detailed list of reoperations performed. In all, 40% of major complications took place in the intermediate term between 31 and 90 days following the operation. There was no difference in rate of major complications between those with recurrent CRC and those with locally advanced primary CRC (P = 0.2). The most common major complication amongst patients was an abdominal or pelvic abscess (n = 6). Other major complications recorded included small bowel obstruction (n = 2), hydronephrosis (n = 1), hernia (n = 1), gastrointestinal anastomotic leak (n = 1), bleeding (n = 1), ileus (n = 1), perineal wound infection (n = 1), and respiratory failure (n = 1). There were no perioperative mortality events during the 90-day study period.
Oncologic Outcomes
RFS and OS for all 27 Patients With Clinical T4b Disease Undergoing TPE.

RFS = Recurrence Free Survival. OS = Overall Survival. CI
Logistic Regression
Multivariable Logistic Regression Predicting Major Postoperative Complications.

CI: 95% confidence interval.
Discussion
In this study, we descriptively annotated short and intermediate postoperative complications by Claviden-Dindo classification of 27 CRC patients undergoing TPE for clinical T4b CRC. Several important findings regarding the contemporary complication profile of this high-risk procedure emerged which may estimate morbidity to better inform patients preoperatively when providing informed operative consent.
Our institution’s experience with TPE for clinical T4b CRC demonstrated significant postoperative morbidity, but no mortality. Approximately 85% of patients experienced at least one complication, however, this also includes non-interventional postoperative complications that may ultimately carry limited impact on a patient’s recovery. While studies frequently omit rates of any complication, the value presented in our investigation falls within the upper range reported by a systematic review assessing all pelvic exenteration procedures for rectal cancer. 16 As previously reported in other pelvic malignancies, this is to be expected as morbidity tends to increase with more extensive resections. 17 Further, just over one third of patients (37.0%) in our series experienced at least one major complication, with the most common being a deep or organ site abscess. This mirrors contemporary studies assessing TPE across all pelvic malignancies 9 and rectal cancer specifically. 8 Notably, no difference in complication rate was observed between primary and recurrent CRC patients. Lastly, despite the high morbidity, our study did not have any deaths within the 90-day window, corroborating recent reports of minimal perioperative mortality.4,5,9
Importantly, the present study also assessed the timing of each major complication. In comparison to those studies assessing 30-day morbidity, we tracked complications through 90 days and stratified them according to time. We found that 40% of major complications took place beyond the classically studied 30-day window, highlighting the importance of extended close follow up. This information is particularly crucial when adjuvant treatment(s) are considered or indicated. 18 Major complications may render a patient unfit for timely therapy, which may portend worse oncologic outcomes.19,20 Therefore, physicians must appropriately educate their CRC patients on this risk when TPE is a consideration.
Separately, we investigated the potential prognostic factors of major complications, including neoadjuvant therapies, preoperative lab metrics, and prior surgical history. Elevated hemoglobin was found to predict major complications on univariate analysis, but this was not upheld by the multivariable regression model. Previous pelvic exenteration studies have also explored the prognostication of major complications. Notably, the PelvEx Collaborative found neoadjuvant therapy to be associated with heightened morbidity. 4 However, more recent case series assessing TPE specifically have suggested that neoadjuvant therapy does not affect morbidity. We reached a similar conclusion, finding no association between the use of neoadjuvant therapy, or the timing of its administration before surgery, and postoperative morbidity. The overall inconsistency of findings with respect to predicting TPE complications underscores the heterogeneity of the patient population and the unique challenge of identifying universal prognosticators.
While not the primary aim of the study, we evaluated the oncologic outcomes of patients in the case series. We found one- and 2-year RFS measures of 83.9% and 72.6%, respectively. At the same time points, OS was 91.1% and 80.0%, respectively. To date, most modern case series include either numerous pelvic malignancies or multiple exenteration types, making it difficult to understand CRC specific outcomes in TPE exclusively. Our 1-year and 2-year survival measures, however, are comparable to those contemporary investigations that have also assessed TPE in CRC.8,9
There are several limitations of the present study. It is based upon retrospective analysis, the sample size is relatively small, and the patients all were treated at a single, tertiary care institution. In particular, the retrospective nature of the study made it difficult to determine if lost and or delayed adjuvant therapy was secondary to extended complications or another cause. Furthermore, the cohort was comprised of heterogenous CRC patients, including both primary and recurrent disease, which may limit the ability to generalize the results to more uniform populations. As such, the results of our study, particularly those that have not been previously investigated, must be validated in a larger, multi-institutional patient cohort. Despite the limitations, it adds to the body of literature regarding the perioperative course of patients undergoing a high-risk pelvic operation for CRC.
In summary, the present study provides a contemporary update of the TPE complication profile for CRC patients with clinical T4b disease. As compared to many previous investigations, we tracked morbidity beyond 30 days, capturing later onset events and emphasizing the need for longer follow up. Secondarily, we assessed the feasibility of predicting major complications in an inherently heterogenous patient group while also elucidating the oncologic outcomes of TPE in CRC.
Conclusion
Total pelvic exenteration is an aggressive oncologic resection that may offer long-term survival in rectal adenocarcinoma, however, is associated with significant morbidity. In this surgical series annotating postoperative complications, perioperative morbidity occurred in the majority of patients, with approximately a third experiencing a major complication. Of these major complication events, 40% occurred beyond the 30-days from TPE, highlighting the importance of extended, close follow up. This annotated postoperative complication profile series may assist patient and clinician decision-making when considering pursuing exenteration.
Supplemental Material
Supplemental Material - Short- and Intermediate-Term Morbidity Following Total Pelvic Exenteration in Colorectal Cancer
Supplemental Material for Short- and Intermediate-Term Morbidity Following Total Pelvic Exenteration in Colorectal Cancer by Christopher Guske, Nusheen Immen, Devon Conant, Jose Laborde, Joshua Linscott, Mitchell Hayes, Seyed Behzad Jazayeri, Adnan Fazili, Erin Siegel, Sophie Dessureault, Julian Sanchez, Amalia Stefanou, Brandon Manley, and Seth Felder in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.