
Abstract
Background:
Whether the presence of postoperative complications was associated with poor prognosis of gastric carcinoma (GC) patients remain controversial. This meta-analysis was designed and reported to compare the survival difference between patients with complications and non-complications.
Methods:
Cochrane Library, PubMed and Embase databases were comprehensively searched for published literatures to review current evidence on this topic. The survival data were extracted, and a random-effect or fixed-effect model was used to analyze the correlation between postoperative complications and oncologic outcome of GC patients.
Results:
Of all studies identified, 32 were eligible for this pooled analysis, with a total of 32,067 GC patients. The incidence of postoperative complications was approximately 12.5% to 51.0%. Among them, infectious complications varied from 3.0% to 28.6%, anastomotic leakage varied from 1.1% to 8.7% and postoperative pneumonia varied from 1.6% to 12.8%. The presence of postoperative complications resulted in a significant poorer overall survival (OS) of gastric carcinoma patients (hazard ratio [HR]:1.49, 95% confidence interval [CI]: 1.33-1.67, P < 0.001). Additionally, the pooled results showed a significant correlation between infectious complications and decreased OS (HR: 1.61, 95%CI: 1.38-1.88, P < 0.001). Concerning specific postoperative complications, we found that both anastomotic leakage (HR: 2.36, 95%CI: 1.62-3.42, P < 0.001) and postoperative pneumonia (HR: 1.74, 95%CI: 1.22-2.49, P = 0.002) impaired the OS of gastric carcinoma patients.
Conclusion:
Postoperative complications were significantly correlated to recurrence and poor survival in gastric carcinoma patients. To gain a better surgical outcome and long-term oncological outcome, postoperative complications should be minimized as much as possible.
Keywords
Introduction
According to the 2018 Global Cancer Statistics, gastric carcinoma remains the common type of lethal malignancies around the world, although its prognostic outcome has been remarkably improved. 1 Surgical resection with adequate lymphadenectomy is the most effective treatment of choice for resectable gastric carcinoma. However, D2 lymphadenectomy is a complex and challenging task for the surgeons, resulting in a high incidence of postoperative complications. 2,3
Major and severe postoperative complications increase treatment costs, prolong the hospitalization time and have a negative effect on the quality of life. It has been reported that postoperative complications, 4,5 especially for infection complications, 6,7 anastomotic leakage, 8,9 and postoperative pneumonia, 10,11 are significantly related to a higher risk of local recurrence and worse long-term survival in gastric carcinoma patients. According to the analytic data of Wu et al, 12 the 3-year overall survival (OS) rate and 3-year relapse-free survival (RFS) rate of gastric carcinoma patients with postoperative complications were 56.8% and 43.5%, respectively. In contrast, the 3-year OS rate was 66.0% and 3-year RFS rate was 58.1% in those without postoperative complications. The survival curves revealed a significant survival difference. 12 However, other studies have shown that independent prognostic significance of postoperative complications is not significant in the adjusted multivariate regression analysis, although the prognosis of gastric carcinoma patients who had postoperative complications is inferior to that of those without postoperative complications. 13 Understanding the prognostic significance of postoperative complications for gastric carcinoma patients is crucial to perioperative management and clinical treatment decision-making. In the current analysis, we systematically reviewed the current evidence and reported a meta-analysis to explore whether the presence of postoperative complications was associated with poor prognosis of gastric carcinoma patients who were treated with surgical resection.
Methods
Literature Search Strategy
Two investigators performed a systematic search for relevant literatures using the Cochrane Library, EMBASE (Ovid) and MEDLINE (Pubmed) databases. The search strategy inlcuded the following keywords and medical subject heading (MeSH) terms: “postoperative complication”, “anastomotic leakage”, “pneumonia” or “pulmonary infection”, “Clavien-Dindo”, “gastric cancer”, “gastric carcinoma” or “gastric adenocarcinoma”, “gastrectomy” and “prognosis”, “survival” or “prognostic”. The primary collection of studies was identified according to these combined keywords. What’s more, we scrutinized the reference lists of previously published literatures to ensure that all relevant studies were not missed. There is no language and publication date limitation for full-text index.
Eligibility Criteria
Eligible studies should report a comparison of survival outcome between gastric carcinoma patients who had and did not have postoperative complications. The original data from included studies, including OS, cancer-specific survival (CSS), disease-free survival (DFS) or RFS, were available. Hazard ratio (HR) and its 95% confidence intervals (CIs) were used as the summary statistics for survival data, and all data was extracted from the multivariate Cox regression analysis in order to control the effect of confounding variables on the pooled outcomes. The presence of postoperative complication was defined as an unusual course that occurred during within 30 days after surgery or the whole hospitalization. The studies assessed the severity of postoperative complications using the Clavien-Dindo classification, which was a treatment-oriented, objective criterion. 14 Those studies that did not use the Clavien-Dindo classification to define the presence of postoperative complications or did not report at least 1 of long-term oncological outcomes should be excluded. In case of studies with overlapping data from the same populations, the most recent or the most informative study was included. Conference abstracts, letters to the editor, comments, review articles and case series were excluded.
Data Extraction and Assessment of Methodological Quality
The authors systematically reviewed the titles and abstracts of relevant literatures identified by the electronic search, and studies deemed potentially relevant were further selected for full-text screening. Relevant data and information extraction were independently conducted by 2 investigators using a standardized electronic form. In case of discordance, a collective discussion was made to reach a consensus. For non-randomized, observational reports, risk of bias for included study was evaluated by the Newcastle-Ottawa quality assessment scale (NOS), 15 which scored each study based on the methodological items. Studies with a NOS score of 7 or more were thought of methodological high-quality. This systematic review and meta-analysis was conducted and reported according to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement.
Statistical Analysis
The primary oncological outcomes of this pooled analysis included OS, CSS and RFS. Overall survival (OS) was defined as the time interval from the first surgery to the date of death from any cause or the last follow-up. Cancer-specific survival (CSS) was defined as the time interval from the date of surgery to the date of death related to gastric carcinoma or the last follow-up. Recurrence-free survival (RFS) was defined as the time interval from the date of surgery to the date of the first recurrence. In this meta-analysis, we used the HR estimates with 95% CIs as a summary statistical measure to calculate and weigh the correlation between postoperative complications and survival outcomes of gastric carcinoma patients. As time-to-event outcomes, a pooled HR more than 1 represented a worse prognosis in the experimental group (complication group) than in the contrast group (non-complication group). The Cochran Q test and the inconsistency (I2) statistic were used to quantitatively evaluate the degree of heterogeneity among included studies, and I2 statistic of greater than 50% and/or P value of less than 0.01 for Q test represented a considerable heterogeneity. In view of high clinical heterogeneity for the presence of postoperative complications, in this study, we selected a random-effect model to estimate the pooled HR of all outcomes.
Subgroup analyzes stratified by the study populations (Western versus Eastern), pathological stage (stage I-III versus stage I-IV), study size (≥450 versus <450), the frequency of postoperative complications (≥25% versus <25%, based on the median of postoperative complication rates), Clavien-Dindo classification (≥grade II vs ≥grade III) and assessment score of methodological quality (≥7 versus <7 points) were performed to explore the clinical and methodological sources of heterogeneity. In addition, the publication bias for this meta-analysis was visually detected by the funnel plots via their symmetry. In this study, we used the Stata 13.0 software (Stata Corporation, College Station, TX, USA) to perform all data processing and statistical analyzes. The threshold of a 2-tailed P value for statistical significance was set at 0.05 for all analyzes.
Results
Search Results and Main Characteristics of Eligible Studies
Figure 1 showed the selection process of eligible studies. We initially identified 948 potentially relevant literatures from electronic databases through the predefined search strategy. 891 studies were considered to be irrelevant to this topic after scanning the titles and abstracts. Subsequently, the full texts of the remaining 57 articles were further screened to determine which studies met the eligibility criteria. Of these studies, 6 studies did not use Clavien-Dindo grade to describe the severity of postoperative complications, 8 studies did not present the prespecified outcomes, 4 were duplications, and 7 were review articles. Ultimately, a total of 32 published literatures were entered into qualitative or quantitative analysis. 4 -13,16 -38

The flow diagram of study selection.
Table 1 summarized the baseline characteristics of the included literatures. This meta-analysis involved 32,067 study participants who underwent gastrectomy for gastric carcinoma, which included 5,141 patients with postoperative complications and 26,926 patients without postoperative complications, with study sizes ranging from 101 to 5,327. The included studies were published between 2009 and 2020, of which all had a retrospective design. Among these studies, 17 were conducted in Japan, 7 were conducted in China, 4 were carried out in Europe, 2 were carried out in Korea and 2 were conducted in the USA. A total of 22 studies reported the data on comparing survival difference between overall postoperative complication and non-complication groups, and 7 studies and 3 studies specifically focused on the influence of anastomotic leakage and postoperative pneumonia on survival outcomes in gastric carcinoma patients, respectively. The median follow-up period ranged from 3.6 to 149.9 months. According to included studies, the incidence of overall postoperative complications varied from 12.5% to 51.0% across gastric carcinoma patients who underwent surgical resection. The frequency of overall postoperative complications ranged from 14.8% to 39.5% in Japan, ranged from 12.5% to 40.6% in China and ranged from 34.0% to 51.0% in Western countries, respectively. In terms of the postoperative complication category, the incidence of infectious complications, anastomotic leakage and postoperative pneumonia varied from 3.0% to 28.6%, 1.1% to 8.7% and 1.6% to 12.8%, respectively.
Clinicopathological Characteristics of Included Studies.

Abbreviations: C, complication group; NC, no complication group; PC(%), overall incidence of overall postoperative complication; IC(%), the incidence of postoperative infectious complication; AL(%), the incidence of anastomotic leakage; PP(%), the incidence of postoperative pneumonia; C-D, Clavien-Dindo classification; OS, overall survival; CSS, cancer-special survival; DFS, disease-free survival; RFS, recurrence-free survival; HR, hazard ratio.
Overall Postoperative Complications
In total, 18 reports compared the OS between postoperative complication and non-complication groups, and 12 of these studies showed a significant survival difference. Meta-analysis of the pooled data demonstrated a pooled HR of 1.49 for OS (95% CI: [1.33, 1.67], P < 0.001), and heterogeneity I2 was significant at 52.3% (P = 0.005) (Figure 2A). Next, we performed the sensitivity analysis and the result showed that the study of Li et al (2013) 16 might be a potential sources of heterogeneity for OS. The pooled result remained significant and heterogeneity was markedly decreased when this study was removed (HR: 1.43, 95% CIs: [1.29, 1.59], P < 0.001; I2 = 38.6%) (Figure S1).
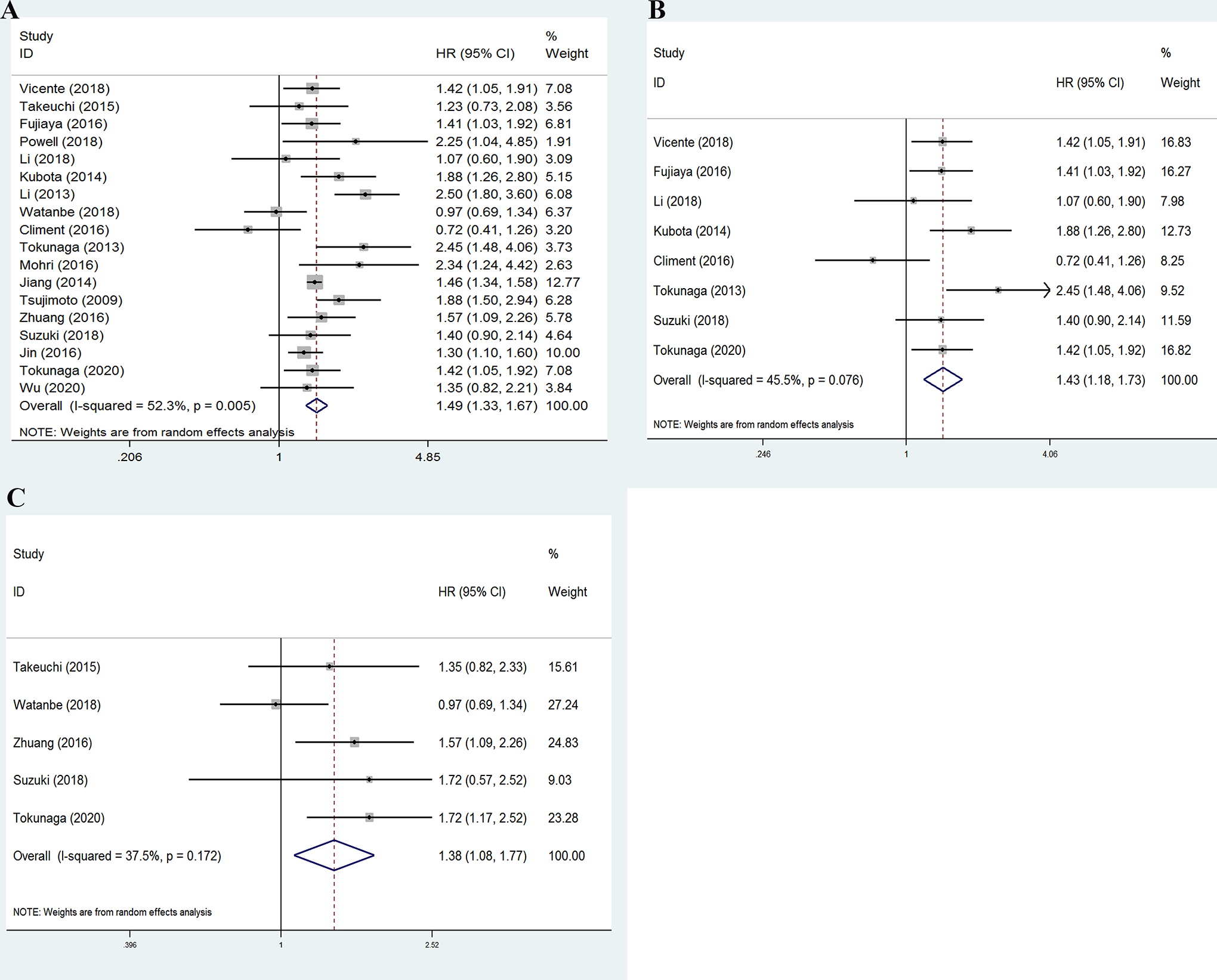
(A) Forest plots evaluating the impact of postoperative complications on the OS of gastric carcinoma patients. (B and C) Forest plots evaluating the impact of the severity of postoperative complications on the OS of gastric carcinoma patients. (B) For Clavien-Dindo grade ≥II; (C) for Clavien-Dindo grade ≥III.
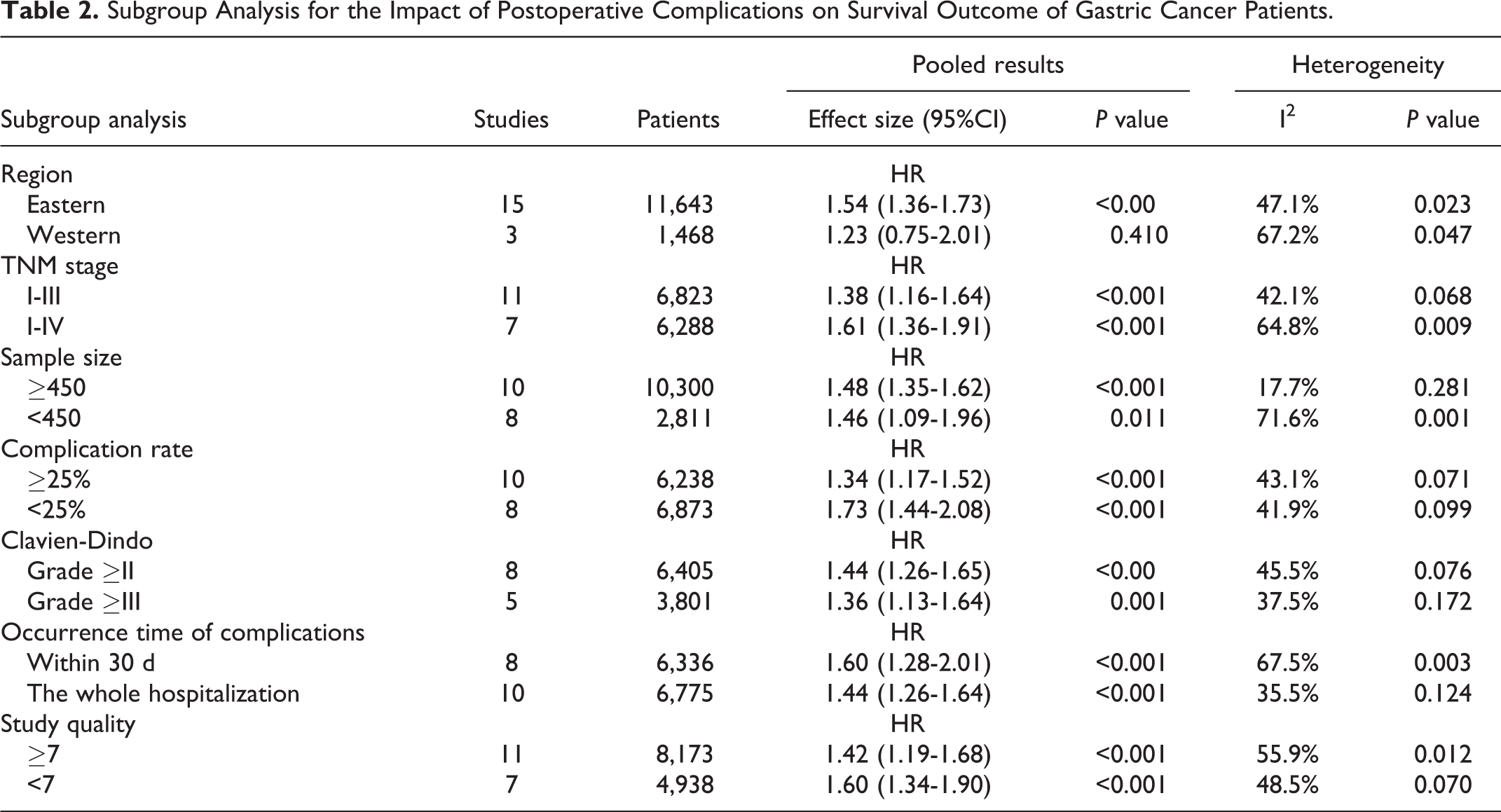
Table 2 shows the results of the subgroup analysis for prognostic effect of postoperative complications. The results demonstrated that the sample size, tumor stage, Clavien-Dindo grade, the frequency of postoperative complications, occurrence time of postoperative complications, and study quality could not affect the pooled results except for geographic area. In addition, we also conducted a meta-regression analysis based on the stratified variables (eg: sample size, the frequency of postoperative complications, TNM stage and study quality), but the results did not show any significant sources of heterogeneity (Supplemental material).
Subgroup Analysis for the Impact of Postoperative Complications on Survival Outcome of Gastric Cancer Patients.
The available data on RFS and CSS measures were extracted from 11 studies and 7 studies, respectively. Meta-analysis of recurrence and cancer-specific survival also indicated that the presence of postoperative complications resulted in a worse long-term oncological outcomes of gastric carcinoma patients (HR for RFS: 1.36, 95% CIs: [1.17, 1.58], P < 0.001; I2 = 38.3%; HR for CSS: 1.63, 95% CIs: [1.24, 2.13], P < 0.001; I2 = 66.0%) (Figure S2).
Clavien-Dindo Grader
In the analysis of the severity of postoperative complications, we found that Clavien-Dindo grade II or higher had a negative impact on both OS (HR: 1.43, 95% CIs: [1.18, 1.73, P < 0.001; I2 = 45.5%) (Figure 2B) and RFS (HR: 1.28, 95% CIs: [1.10-1.49], P = 0.002; I2 = 35.0%) (Figure S3A). Similarly, postoperative complications with Clavien-Dindo grade ≥III significantly reduced the OS of gastric carcinoma patients (HR: 1.38, 95% CIs: [1.08, 1.77], P = 0.009; I2 = 37.5%) (Figure 2C).
Infection Complications
In included studies, infection complications were defined as being present in patients who received antibiotic therapy for an infection or suspected infection and had at least 1 of the following: body temperature ≥38.0°C, white blood cell count > 10,000/µL and positive blood or fluid culture. 6,24 In general, infectious complications included wound infection, intra-abdominal abscess, pancreatic fistula, anastomotic leakage, pneumonia, cholecystitis, catheter-related sepsis, urinary tract infection and so on. The results of this meta-analysis also revealed a negative relevance between infection complications and OS in gastric carcinoma patients (HR for OS: 1.62, 95% CI: [1.34, 1.95], P < 0.001; I2 = 28.3%), as illustrated in Figure 3A. Similarly, the presence of infection complications was significantly associated with worse RFS (HR for RFS: 1.59, 95% CI: [1.34, 1.89], P < 0.001; I2 = 1.5%) (Figure S3B).

Forest plots evaluating the impact of different types of postoperative complications on the OS of gastric carcinoma patients. (A) For infectious complications; (B) for intra-abdominal infectious complications; (C) for anastomotic leakage; (D) for postoperative pneumonia.
Intra-abdominal infection complications included pancreatic fistula, anastomotic leakage, and intra-abdominal abscess without leakage. Our results suggested that there was a significant decrease in OS (HR: 1.48, 95% CIs: [1.14, 1.93], P = 0.004; I2 = 42.5%) (Figure 3B) and RFS following intra-abdominal infection complications (HR: 1.44, 95% CIs: [1.11, 1.87], P = 0.006; I2 = 38.5%) (Figure S3C).
Anastomotic Leakage and Postoperative Pneumonia
Concerning the specific postoperative complications, we found that both anastomotic leakage (HR: 2.36, 95% CIs: [1.62, 3.42], P < 0.001; I2 = 73.6%) and postoperative pneumonia (HR: 1.74, 95% CI: [1.22, 2.49], P = 0.002; I2 = 64.5%) had a correlation to poor OS of gastric carcinoma patients (Figure 3C and D). Moreover, the presence of anastomotic leakage was significantly associated with worse CSS of these patients (HR: 2.46, 95% CI: [1.41, 4.31], P < 0.001; I2 = 69.1%) (Figure S3D).
Publication Bias
The funnel plots of pooled analysis for the impact of postoperative complications on the prognosis of gastric carcinoma patients revealed no significant asymmetry, suggesting a low possibility of publication bias (Figure 4).
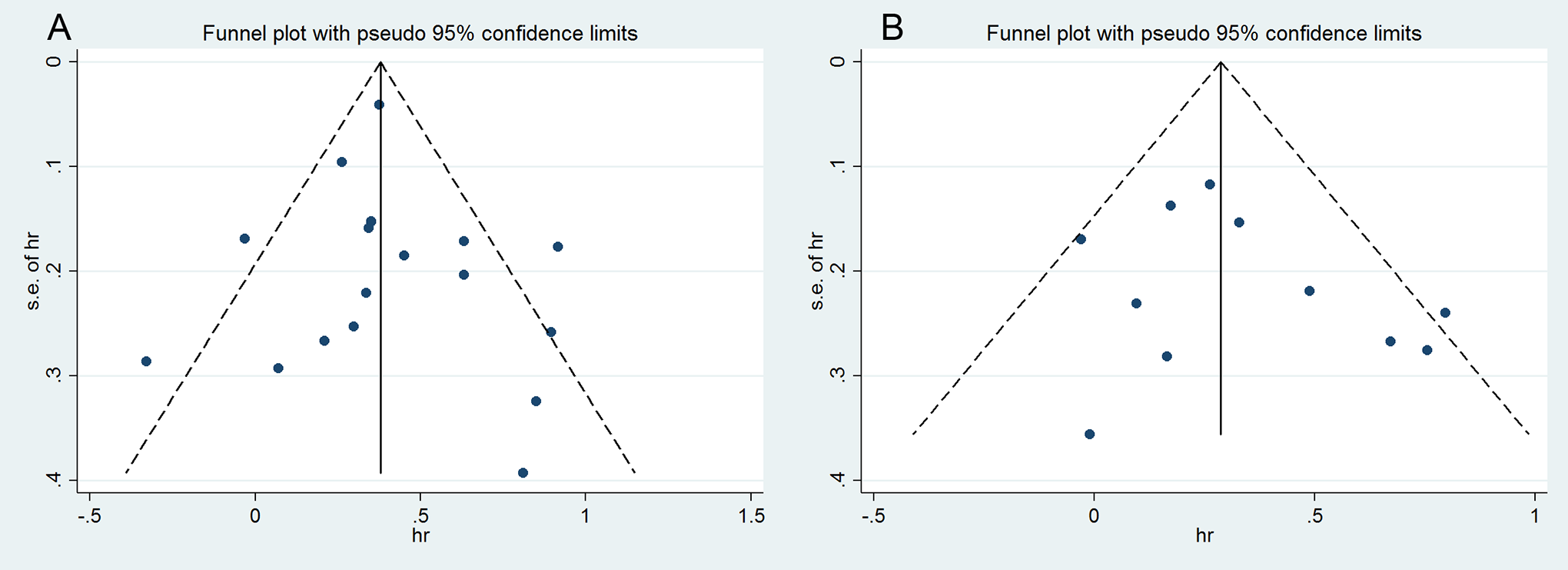
Funnel plot for the association between postoperative complications and the prognosis of gastric carcinoma patients. (A) For overall survival (OS); (B) for recurrence-free survival (RFS).
Discussion
Infectious complications, including duodenal stump leakage, pancreatic fistula, anastomotic leakage, intra-abdominal infection/abscess, wound infection and pneumonia, are the most common postoperative complications after gastrectomy with curative intent. The adverse impacts of postoperative complications, especially for infectious complications, on recurrence and long-term survival have been reported previously. 6 -8,10 By comparing the survival outcomes of gastric carcinoma patients, Hayashi et al showed that the 5-year RFS rates were 58% and 83% in those with and without infectious complications, respectively. 6 Similarly, Kubota et al assessed the prognostic significance of postoperative complications for gastric carcinoma patients using the propensity-score matching analysis, and the results revealed a significant and independent correlation between infectious complications and poor survival outcomes (HR for OS: 1.88, 95% CIs: [1.26, 2.80], P < 0.001; HR for CSS: 1.90, 95% CIs: [1.19, 3.02], P < 0.001). 4 These findings suggested that the presence of postoperative complications, especially infectious complications, was significantly correlated to disease recurrence and poor survival. However, a few studies reported a conflicting finding with regard to the prognostic effect of postoperative complications. 13,19,26 In the current study, we systematically searched relevant literatures and evaluated the correlation between postoperative complications and oncological outcomes of gastric carcinoma patients. The results of meta-analysis indicated that the presence of postoperative complications, including infectious complications, intra-abdominal infectious complications, anastomotic leakage and postoperative pneumonia were predictors of recurrence and poor long-term survival.
The following several possible reasons may explain why there was a negative correlation between postoperative complications and prognostic outcomes. First, inflammatory responses to severe postoperative complications may result in immune suppression. The cell-mediated immune response, particularly involving cytotoxic T lymphocytes and natural killer cells, is compromised by systemic inflammation and surgical stress, promoting the immune escape of micrometastatic carcinoma cells. 39,40 Second, a large amount of activated leukocytes and cytotoxic mediators such as interleukin-1(IL-1), IL-6 and TNF-α released from the inflammatory response could accelerate the proliferation and invasion ability of residual cancer cells, which promotes the development of tumor recurrence and metastasis. 13,41 Consequently, reducing surgical stress and postoperative inflammatory responses may be helpful to improve short-term and long-term outcomes. Recent evidence have demonstrated that laparoscopic surgery for gastric carcinoma has more advantages over open gastrectomy in the field of surgical trauma, intraoperative blood loss and postoperative recovery. 42,43 With the advancement in laparoscopic technique and accumulation of surgical experience, laparoscopic gastrectomy has increasingly become an alternative surgical procedure for gastric carcinoma patients, and surgical trauma and the incidence of postoperative complications would be further reduced in the future.
Another possible explanation for the adverse impact of postoperative complications on survival outcome is the delayed initiation of adjuvant chemotherapy or the omission of adjuvant chemotherapy caused by severe postoperative complications. In general, adjuvant chemotherapy should be initiated as soon as possible after full recovery from surgery. It has been demonstrated that advanced, resectable gastric carcinoma patients could benefit from perioperative chemotherapy. 44 However, Kubota et al revealed that the initiation time of adjuvant chemotherapy for gastric carcinoma patients who had postoperative complications was later by at least a median of 1 week than that for those who had no postoperative complications. 4 A previous report demonstrated that at least half of gastric carcinoma patients who had postoperative complications were unlikely to be treated by adjuvant chemotherapy. 29 The data revealed that the combination of postoperative complications and no adjuvant chemotherapy increased the risk of death by more than 200% in comparison to patients who did not experience postoperative complications and received adjuvant chemotherapy. However, the overall survival of gastric carcinoma patients with postoperative complications could be improved by adjuvant chemotherapy. 29 In other words, delayed initiation or the failure to receive adjuvant chemotherapy may play an intermediate role in decreased survival of patients with postoperative complications.
Anastomotic leakage is a major and serious surgical-related complication, and its incidence varies from 1.1% to 8.7% in gastric carcinoma patients who underwent surgical resection. 7,8,23,31 Despite the low incidence, anastomotic leakage prolongs the length of hospital stay and increases the risk of hospital mortality. The results of the current study indicated that anastomotic leakage had a detrimental impact on the long-term survival outcome of gastric carcinoma patients. Based on these findings, meticulous surgical techniques and intensive perioperative care should be encouraged to minimize the morbidity rate and improve long-term oncological outcomes. Postoperative pneumonia was another common complication after surgical resection for gastric carcinoma, and its frequency has been reported to be 1.6% to 12.8%. 5,23,35 Our study also investigated the influence of postoperative pneumonia on oncological outcomes, indicating that it is responsible for worse overall survival of gastric carcinoma patients who underwent curative-intent resection. Concerning the occurrence of postoperative pneumonia, it has been shown that elder age (≥65 years), poor nutritional status, advanced tumor stage (≥stage II), comorbid disease, total gastrectomy and extended lymphadenectomy are its independent risk factors. 10,35 To prevent the occurrence of postoperative pneumonia, active preoperative interventions such as respiratory function training and sufficient nutritional support should be considered.
In the current study, we confirmed the negative correlation between postoperative complications and poor survival in gastric carcinoma patients who underwent gastrectomy. Based on current evidence, however, it is difficult to determine whether the systemic inflammatory response or postoperative complications themselves have a direct effect on the survival outcomes of these patients. Saito et al reported that the 5-year RFS of patients who had postoperative complications was significantly worse than that of those who did not experience postoperative complications, but adjusted multivariate analysis indicated that the level of serum C-reactive protein (CRP) rather than postoperative complication could independently affect the prognostic outcome of gastric carcinoma patients. 13 The researchers believed that systemic inflammatory response induced by surgical trauma and tissue damage resulted in poor prognostic outcome even if postoperative complications did not occur. In addition, it is also hard to determine that the negative correlation should be ascribed to patient-specific conditions or postoperative complications. It has been reported that combined multiorgan resection, extended lymphadenectomy, a high body mass index(BMI) (≥25 kg/m2) and prolonged operation time are independent predictors for the presence of postoperative complications. 16,17,45 In addition to surgery-related factors, postoperative complications can occur as a result of other factors such as advanced age, poor performance status and severe comorbidities, 23 which also can significantly affect the oncological evaluation of gastric carcinoma patients, especially in the case of death unrelated to gastric carcinoma.
Several limitations may still existed in this study and need be further underlined. First, the level of current evidence from this meta-analysis is relatively limited. All data and conclusions were based on retrospective design, which inevitably introduce a potential source of bias. Moreover, the studies that did not provide data on HR and its 95% CIs had to be excluded from this meta-analysis, which might also result in a potential bias. Second, although all studies used the Clavien-Dindo grade to assess the severity of postoperative complications, its definition was inconsistent across studies. Not all studies classified patients with grade II or more severe postoperative complications into the research group. Moreover, the occurrence time of postoperative complications were not clearly defined by a few studies. These differences may become a potential source of high heterogeneity and limit the comparison between postoperative complication and non-complication groups. However, we further performed a subgroup analysis for the severity and the occurrence time of postoperative complications to determine their impacts on the prognosis of gastric carcinoma patients, and the results still showed a significant finding. Third, although we used adjusted HR and 95% CIs to perform the pooled analysis, there may be several covariates or unknown factors (e.g., physical status, comorbidities and surgical quality) that were not included in multivariate Cox regression analysis. On the other hand, the baseline characteristics, such as surgical procedures, the extent of lymphadenectomy and the administration of adjuvant chemotherapy, were not comparable among the included studies. However, it is unlikely to design and carry out a RCT for evaluating the prognostic significance of postoperative complications for gastric carcinoma patients since their occurrence could not be controlled or adjusted. This systematic review and meta-analysis was helpful for understanding the prognostic significance of postoperative complications in gastric carcinoma patients and guiding subsequent treatment strategies.
Conclusions
Postoperative complications including infectious complications, intra-abdominal infectious complications, anastomotic leakage and postoperative pneumonia were significantly associated with poor survival outcomes and tumor recurrence in gastric carcinoma patients. Although the exact mechanism underlying this negative correlation was unclear, the establishment of perioperative management aimed at minimizing complications was necessary for the improvement of short-term and long-term outcomes of resectable gastric carcinoma patients.
Supplemental Material
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211011955 - Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-1-ccx-10.1177_10732748211011955 for Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis by Guofeng Chen, Jun Wang, Kaibo Chen, Muxing Kang, Hang Zhang, Xiaoli Jin, Lele Lin and Jian Chen in Cancer Control
Supplemental Material
Supplemental Material, sj-pdf-2-ccx-10.1177_10732748211011955 - Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis
Supplemental Material, sj-pdf-2-ccx-10.1177_10732748211011955 for Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis by Guofeng Chen, Jun Wang, Kaibo Chen, Muxing Kang, Hang Zhang, Xiaoli Jin, Lele Lin and Jian Chen in Cancer Control
Supplemental Material
Supplemental Material, sj-tif-1-ccx-10.1177_10732748211011955 - Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis
Supplemental Material, sj-tif-1-ccx-10.1177_10732748211011955 for Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis by Guofeng Chen, Jun Wang, Kaibo Chen, Muxing Kang, Hang Zhang, Xiaoli Jin, Lele Lin and Jian Chen in Cancer Control
Supplemental Material
Supplemental Material, sj-tif-2-ccx-10.1177_10732748211011955 - Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis
Supplemental Material, sj-tif-2-ccx-10.1177_10732748211011955 for Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis by Guofeng Chen, Jun Wang, Kaibo Chen, Muxing Kang, Hang Zhang, Xiaoli Jin, Lele Lin and Jian Chen in Cancer Control
Supplemental Material
Supplemental Material, sj-tif-3-ccx-10.1177_10732748211011955 - Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis
Supplemental Material, sj-tif-3-ccx-10.1177_10732748211011955 for Relationship Between Postoperative Complications and the Prognosis of Gastric Carcinoma Patients Who Underwent Surgical Resection: A Systematic Review and Meta-Analysis by Guofeng Chen, Jun Wang, Kaibo Chen, Muxing Kang, Hang Zhang, Xiaoli Jin, Lele Lin and Jian Chen in Cancer Control
Footnotes
Authors’ Note
Guofeng Chen, MD, and Jun Wang, MD, are equal contributors to this work. All data and materials related to this manuscript can be accessed via e-mail to the corresponding author. No ethical approval and informed consent were required for this systematic review and meta-analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Zhejiang Provincial Key Project of Research and Development (2019C03043).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.