
Abstract
Background
Splenic flexure adenocarcinoma poses unique challenges in surgical management due to its location and lymphatic drainage. This study compared the efficacy and oncological safety of extended right hemicolectomy (ERC) and left colectomy (LC) for treating this condition.
Methods
This study followed the PRISMA and AMSTAR 2 guidelines. Key outcomes included postoperative mortality, morbidity, severe complications, operative results, pathological findings (R0 resection, lymph nodes), and oncological results (overall survival and disease-free survival at 3 and 5 years).
Results
Twelve non-randomised studies were included involving 1710 patients (713 ERC group, 997 LC group). The analysis showed that ERC was associated with more lymph nodes and a lower conversion rate. However, there were no significant differences between ERC and LC in terms of mortality, morbidity, severe complications, anastomotic leak, wound infection, ileus, reoperation, R0 resection, hospital stay, and overall and disease-free survival rates.
Conclusions
ERC and LC are comparable in terms of postoperative and long-term oncological outcomes for splenic flexure adenocarcinoma, with ERC potentially producing a higher lymph node harvest rate and a lower conversion rate. ERC could be suggested for a better stage of the disease and when the surgical team considers the laparoscopic approach.
Keywords
Introduction
Colorectal cancer (CRC) is the most prevalent malignancy of the gastrointestinal tract, with splenic flexure adenocarcinoma being a specific entity. 1 This tumour is typically located between the distal third of the transverse colon and the proximal segment of the descending colon. 2 Splenic flexure adenocarcinoma is a distinct surgical entity that represents approximately 3% of all resected colorectal cancers, although its definition in the literature is not explicit. 3 This type of cancer exhibits unique pathological characteristics, particularly lymphatic drainage, that extend to the right and left regions of the colon. However, the optimal surgical intervention remains a topic of debate. Due to its positioning at the junction of the superior and inferior mesenteric vasculature, there is ongoing discussion in the surgical community about its classification as either a tumour of the right or left-sided tumor. Clinically, two variants of colectomy are widely considered: extended right hemicolectomy (ERC) and left colectomy (LC). Despite this, there is no consensus on the appropriate extent of surgical resection for splenic flexure adenocarcinoma. The current literature does not demonstrate significant differences between these two techniques in terms of short- and long-term outcomes.1,2 Taking into account the varying extents of bowel resection and their potential physiological impact on patients, a comparative analysis of these techniques is essential. This study aimed to compare two surgical approaches, ERC and LC, to identify the most effective management strategy for splenic flexure adenocarcinoma, with a focus on postoperative outcomes, pathological findings, and oncological outcomes.
Methods
This study was conducted according to the PRISMA guidelines 2020 (Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines 3 and AMSTAR 2 guidelines (assessing the methodological quality of systematic reviews). 4 The study protocol was registered with PROSPERO under the number CRD42024516288.
Electronics Searches
The last electronic search of the relevant literature was conducted on May 1, 2023, with no language restrictions. Trials were sought in the following databases: “Cochrane Library,” “United States National Library of Medicine,” “PubMed/MEDLINE”, “Excerpta Medica Database», «Embase,» and “Google Scholar.” Keywords used were: “colon cancer”; “splenic flexure”; “surgery”; “extended right hemicolectomy”; “left colon resection”; “left hemicolectomy”; “subtotal colectomy”; “outcome,” “morbidity,” “mortality,” “overall survival,” and ‘disease-free survival’. We use the Boolean markers “and” and “or.” The reference lists of the articles obtained were checked for eligible clinical trials. Data from descriptive studies, reviews, editorial letters, case series, abstracts, and comments were excluded.
Study Selection
Clinical trials comparing ERC and LC. We included only articles published in peer-reviewed journals.
Participants/Population
Adults (aged >18 years) of either sex who underwent surgery for splenic flexure adenocarcinoma. We studied two different approaches for splenic flexure cancer using an open or laparoscopic approach.
Intervention Group
Patients with splenic flexure adenocarcinoma undergoing extended right colectomy (ERC group).
Control Group
Patients with splenic flexure adenocarcinoma undergoing left colectomy (LC group).
Outcomes
The different outcomes assessed in our study were the postoperative outcomes (mortality, morbidity, severe complications, operative time, anastomotic leak, wound infection, paralytic ileus, reoperation, and hospital stay), pathological findings (R0 resection and number of harvested lymph nodes), and oncological outcomes (3-years overall survival (OS), 5-years OS, 3-years disease-free survival (DFS), and 5-years DFS). Mortality and morbidity were considered if they occurred within 30 days after colon resection. Postoperative results were assessed during the 30-day postoperative period. Most studies used the Clavien-Dindo classification to report postoperative complications. 5 Major complications were classified as grade ≥ III.
Study Selection
Two authors reviewed all abstracts that met the inclusion criteria. Disagreements were resolved after consulting a third author.
Evaluation of Study Quality and Risk of Bias
Two authors assessed studies that met the selection criteria. We used the MINORS (Methodological Index for Nonrandomised Studies scale (MINORS) for CCTs for the quality assessment. 6 Studies with a score <13/24 were excluded. We use the Newcastle-Ottawa Scale (NOS) 5 for bias assessment to assess the quality and risk of bias in randomised and non-randomized clinical trials. The scoring system covers eight items related to three major domains (selection of exposed and non-exposed cohorts, comparability, and outcome assessment).
Data Extraction
Two authors extracted data. Disparities were resolved by the senior author. The following data were extracted: first author’s name, country, year of publication, type of study, period of study, indication for surgery, number of included patients, number of patients in each group, sex, age, body mass index, postoperative results (mortality, morbidity, severe complications, operative time, anastomotic leak, wound infection, paralytic ileus, reoperation, and hospital stay), pathological findings (R0 resection and number of lymph nodes), and oncological results (3-year OS, 5-year OS, 3-year DFS, and 5-year DFS).
Missing Data
In instances of unclear bias domains or missing primary outcome information, the authors were contacted by email. If the data were not numerically reported, information was extracted from the figures.
Certainly Assessment of Evidence
To rate the evidence quality, two authors used the GRADE guidelines. 7 We used GRADEpro GDT software to prepare the “Summary of findings tables.” We explained the downgrading or upgrading of the included studies in the footnotes and comments.
Assessment of Heterogeneity
Three strategies were used to assess heterogeneity between studies.
Effect Size Evaluation
Review Manager 5.3.5: Statistical package from the Cochrane Collaboration was used for meta-analysis. 10 Standardized mean difference (SMD) was selected as an effective measure of continuous data and odds ratios (OR) with 95% confidence intervals (95% CI) for dichotomous variables. We used random-effects model. The significance was set at P less than 0.05. We tested the interaction between the relevant factors and the effects size estimates.
Results
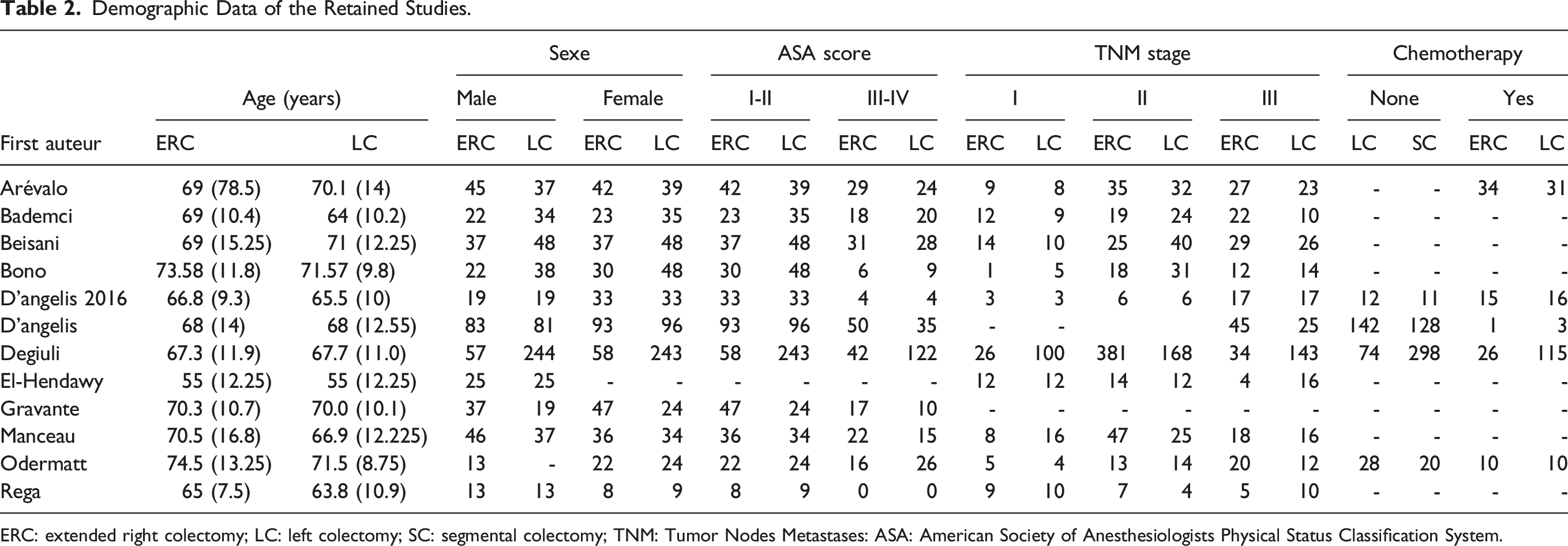
The literature search identified 12 eligible nonrandomized studies that matched the selection criteria11-22 (Figure 1). Five articles were excluded for the following reasons: two studies were systematic reviews and meta-analyses, two were descriptive studies, and one was a letter to the editors. A list of the retained studies is summarised in Table 1. These articles were published between 2013 and 2022. All of these studies were CCTs. Retained studies assessed the outcomes of elective surgery in seven studies and elective and emergent surgeries in five studies. They included 1710 patients: 713 in the ERH group and 997 in the LC group. The follow-up period ranged from 36 to 84 months. The demographic data of the included patients are presented in Table 2. The sex ratio of the included patients was 1.48 with a male predominance. The mean age in the ERC and LC groups ranged from 67.3 to 74.5 Â years and 64.5 years to 71.57 years. The mean BMI ranged from 24.7 kg/m2 to 26 kg/m2 in the ERC group and from 21.9 kg/m2 to 29.3 kg/m2 in the LC group. Patients who had ASA scores (I-II) in the ERC group were 62.81% and in the LC group 65.46%. Patients presenting ASA score (III-IV) in the ERC group were 34.40% and in the LC group were 30.29%. PRISMA 2020 flow-diagram. List of the Retained Studies. ERC: extended right colectomy; LC: left colectomy; SC: segmental colectomy. Demographic Data of the Retained Studies. ERC: extended right colectomy; LC: left colectomy; SC: segmental colectomy; TNM: Tumor Nodes Metastases: ASA: American Society of Anesthesiologists Physical Status Classification System.

Mortality
Eleven studies reported the mortality rate.12-22 It was found in 25 of 619 patients in the ERC group and 15 of 923 patients in the LC group with no difference between the two groups (OR = 1.66; IC95% [0.82, 3.33]; P = 0.16) (supplemental file 1, Figure 2).
Morbidity
It was reported in seven eligible studies.11,14,16-20 It was reported in 134 of 482 patients in the ERC group and 145 of 771 patients in the LC group with no significant difference between the two groups (OR = 0.93; IC95% [0.63, 1.38]; P = 0.72). There was little heterogeneity among the studies (tau 2 = 0.09(I2 = 32%)) (supplemental file 1, Figure 3).
Severe Complications
Severe complications were reported in nine studies.11,13-17,20-22 It was reported in 76 of 566 patients in the ERC group and 105 of 875 patients in the LC group with no significant difference between the two groups (OR = 0.88; IC95% [0.59, 1.33]; P = 0.55)) (supplemental file 1, Figure 4).
Anastomotic Leak
Anastomotic leakage was reported in ten studies.11-17,19-21 It was reported in 44 of 628 patients in the ERC group and 41 of 922 patients in the LC group. There was no difference between the two groups (OR = 1.29; IC95% [0.81, 2.05]; P = 0.28) (supplemental file 1, Figure 5).
Wound Infection
It was reported in five eligible studies.12,14,15,19,20 15 of the 177 patients in the ERC group and 10 of 230 patients in the LC group presented a wound infection with no significant difference between the two groups (OR = 1.56; IC95% [0.67, 3.64]; P = 0.30)) (supplemental file 1, Figure 6).
Ileus
It was reported in five studies.12,14-16,19 42 of 278 patients in the ERC group and 17 of 262 patients in the LC group presented ileus with no significant difference between the two groups (OR = 2.04; IC95% [0.71, 5.83]; P = 0.18). There was little heterogeneity among the studies (tau 2 = 0.45(I2 = 31%)) (supplemental file 1, Figure 7).
Conversion
Conversion was reported in five studies.12,13,15,16,19 It was estimated in 612 patients, occurring in 18 of 310 patients in the ERC group and 38 of 302 patients in the LC group. There was a lower conversion rate in the ERC group (OR = 0.50; IC95% [0.27, 0.90]; P = 0.02)) (supplemental file 1, Figure 8).
Reoperation
Reoperation was reported in five studies.11,16,17,20,21 It was reported in 38 of the 380 patients in the ERC group and 33 of 670 patients in the LC group with no significant difference between the two groups (OR = 1.71; IC95% [0.83, 3.52]; P = 0.15). There was little heterogeneity among studies (Tau2 = 0.26(I2 = 40%)) (supplemental file 1, Figure 9).
R0 Resection
Resection of R0 was reported in four studies.15,17,18,21 199 of 205 patients in the ERC group and 470 of 510 patients in the LC group presented R0 resection with no significant difference between the two groups (OR = 2.16; IC95% [0.89, 5.29]; P = 0.09)) (supplemental file 1, Figure 10).
Harvested lymph Nodes
Harvested lymph nodes were reported in eight studies.11-14,16,18,21,22 It was estimated that there were 881 patients: 426 in the ERC group and 455 in the LC group. There was a greater number of harvested lymph nodes harvested in the ERC group (MD = 0.83; IC95% [0.35, 1.31]; P = 0.0007). There was low heterogeneity between the studies (Tau2 = 0.42(I2 = 91%)) (supplemental file 1, Figure 11).
Hospital Stay
It was reported in eight studies.12-14,16-18,21,22 It was estimated in 1260 patients: 455 in the ERC group and 805 in the LC group with no significant difference between the two groups (MD = 0.02; IC95% [-0.10, 0.14]; P = 0.75)) (supplemental file 1, Figure 12).
Operative Time
It was reported in nine studies.11,12,14-19,22 Operative time was estimated in 1334 patients: 511 in the ERC group and 823 in the LC group with no significant difference between the two groups (MD = 0.18; IC95% [-0.15, 0.51]; P = 0.29). There was low heterogeneity among the studies (Tau2 = 0.21(I2 = 86%)) (supplemental file 1, Figure 13).
Three-Year OS
Overall survival was assessed in 11 studies.11-16,18-22 It was reported in 549 out of 757 patients in the ERC group and 504 out of 753 patients in the LC group. We did not find a difference in overall survival between the two groups (OR = 1.12, 95% CI [0.70, 1.79]; P = 0.64). There was low heterogeneity among the studies (Tau2 = 0.31(I2 = 61%)) (supplemental file 1, Figure 14).
Five-Year OS
Overall survival was assessed in 10 studies.11-16,19-22 It was reported in 356 of the 725 patients in the ERC group and 380 of the 719 patients in the LC group. We did not find a difference in 5-year overall survival between the two groups (OR = 0.88, 95% CI [0.68, 1.13]; P = 0.31)) (supplemental file 1, Figure 15).
Three-Year DFS
Three-year DFS was evaluated in eight studies.11,14-16,18,20-22 It was reported in 366 of 598 patients in the ERC group and 400 of 594 patients in the LC group. We did not find a difference in 3-year DFS between the two groups (OR = 1.03, 95% CI [0.54, 1.98]; P = 0.92). There was low heterogeneity between the studies (Tau2 = 0.48(I2 = 75%)) (supplemental file 1, Figure 16).
Five-Year DFS
The 5-year DFS was evaluated in nine studies.12-17,20-22 It was reported in 250 of 696 patients in the ERC group and 542 of 1035 patients in the LC group. We did not find a difference in 5-year overall survival between the two groups (OR = 0.79, 95% CI [0.62, 1.00]; P = 0.05)) (supplemental file 1, Figure 17).
Included Studies Quality Assessment and the Effects of Surgical Procedure Choice Reporting
The results of our study are summarised in Table 3 and supplementary file 1. Quality assessment and risk of bias are presented in Table 4. A summary of the evidence is presented in Table 5. This review shows that ERC was performed for splenic flexure adenocarcinoma compared to LC. ⁃ It likely increases the number of lymph nodes. Comparison Between Extended Right Colectomy Group and Left Colectomy Group. OR: odds ration; MD: mean difference; CI: confidential interval; OS: overall survival; DFS: disease free survival.

Studies Quality and Risk of Bias Assessment.

CONSORT: Consolidated Standards of Reporting Trials; MINORS: methodological index of non-randomized studies; retro: retrospective; comp: comparative.
Summary of the Findings Table.

*The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: confidence interval; OR: odds ratio; SMD: standardised mean difference; LC: left colectomy; ERC: extended right colectomy GRADE Working Group grades of evidence.
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
aSmall sample size.
bI2 greater than 50%.
Discussion
This systematic review and meta-analysis concluded that the ERC group was associated with a higher number of harvested lymph nodes and a lower conversion rate to laparotomy. We do not know if there is any difference in terms of mortality, morbidity, anastomotic leak, wound infection, ileus, conversion, reoperation, R0 resection, severe complications, hospital stay, 3-year OS, 5-year OS, 3-year DFS, and 5-year DFS because the evidence is very uncertain.
The literature on splenic flexure adenocarcinoma and its optimal surgical intervention is limited and is based on a handful of case series, single-centre retrospective studies, and matched case-control studies. 23 At present, there are no recommendations on the extent of surgery to be performed for splenic flexure tumours. Therefore, there is no optimal surgery, and the choice of surgery depends on several factors. An anonymous survey by members of the Coloproctology Association of Great Britain and Ireland (ACPGBI) showed that ERC was the preferred option by 63% of respondents, followed by LC (23%) and segmental colectomy of the splenic flexure (14%). 24 When we assessed the comparison between ERC and LC, there is little evidence in the literature. ERC and LC are the most commonly used. 19 ERC is more frequently used in the emergency setting because it is technically easier, 24 and there is often a serious concern about the viability of the right colon. Moreover, lymphatic drainage at this site is poorly defined and is assumed to be heterogeneous. 22 In the literature, postoperative complications and mortality after surgery for splenic flexure adenocarcinoma have often been reported to be higher than those of other colon locations. Aldridge et al. 25 concluded that splenic flexure adenocarcinoma is associated with the highest mortality and morbidity rates. Among recent publications, a meta-analysis by Hajibandeh et al. 1 and two additional studies have specifically compared postoperative complications of ERC and LC, while Kim et al. 26 concluded higher morbidity with ERC, whereas Gravante et al. 19 did not find significant differences. Our study did not find any differences between the two groups in terms of mortality and morbidity. Beisani et al. 13 reported that the incidence of postoperative ileus was significantly higher in the ERC group. The larger dissection in the ERC group could explain the slower recovery of bowel movements. In a recent study, no differences were observed between the two groups.
Conventional wisdom suggests that colocolic anastomoses have a higher risk of failure than ileocolic anastomoses due to differences in local vascularization of the stump. Therefore, differences in anastomotic leak rates between the two techniques are expected. 19 However, not all studies have clearly shown that colonic anastomoses are more susceptible to leakage than ileocolic anastomoses. In our study, there were no significant differences in leakage rates between ERC and LC. Gravante et al., 19 Beisani et al., 13 and Hajibandeh et al. 1 found no differences between the two groups. However, Binda et al. 11 reported that anastomotic leak was diagnosed in 35 patients (10.8%), associated with peritonitis in 20, and deep surgical site infection in 15. The risk was higher in the ERC group (10.8%) than in the LC group (8.4%). Furthermore, Hajibendah et al., 1 Binda et al. 27 and Arévalo et al. 11 analysed short-term postoperative complications and found no significant differences between the ERC and LC groups regarding the need for reoperation. Similar results were reported in 38 of the 380 patients in the ERC group and 33 of 670 patients in the LC group. Bademci et al. 12 reported that the conversion rates from laparoscopy to open surgery were 19% in the ERC group and 28% in the LC group. There was no significant difference between the groups in terms of operating time. Interestingly, laparoscopic procedures were safely performed, as indicated by a similar rate of conversion to laparotomy. These results are consistent with the findings of a recent systematic review and meta-analysis by Martnez-Pérez et al. 2 and support the clear trend of the increasing application of laparoscopy to perform both surgical procedures for segmental colectomies. Conversely, in our study, LC resulted in greater conversion than ERC did. When comparing conversion rates between ERC and LC in the context of laparoscopic surgery, the decision to favour ERC over LC is advocated and could influence clinical practice. Reducing the need for conversion to open surgery also optimizes operating room time and resources, which can be particularly beneficial in high-volume centers. It is associated with several benefits, including reduced operating time, shorter recovery periods, decreased pain, and shorter hospital stays, which can reduce overall healthcare costs. If ERC consistently demonstrates lower conversion rates compared to LC, this might indicate that ERC is more straightforward to perform laparoscopically under certain circumstances, potentially leading to better overall outcomes. ERC often involves a simpler dissection along well-defined vascular planes, and ileocolic anastomosis is generally easier to perform laparoscopically. Left colectomies, particularly when involving the splenic flexure, can be more technically challenging due to the less favorable anatomy. The presence of dense adhesions from diverticulitis or other inflammatory conditions can increase the difficulty of laparoscopic dissection and anastomosis. This complexity can result in a higher likelihood of conversion.
Wide resection to obtain a good quality operative specimen is mandatory for greater oncological outcomes.28,29 De Angelis et al.
16
and Hajibandeh et al.
1
found no differences between the two groups in terms of R0 resection. In our study, there were no differences between the two groups in terms of R0 resection. This highlights that the time of resection did not directly affect the resection margin, but mostly affected the number of harvested lymph nodes. This was confirmed after evaluating oncological safety. Beisani et al.
13
found no significant differences between the two strategies. More lymph nodes were harvested in the ERC group, which was consistent with the larger extension of the resected colon. However, the number of invaded nodes remained the same in both groups
De Angelis et al. 16 and Binda et al. 27 findings suggest that progressive extension of surgical resection has a significant impact on postoperative outcomes. Differences were observed when comparing ERC and LC, with longer operative time, more general postoperative complications and postoperative ileus, longer flatus time and longer hospital stay for patients with ERC. This may be explained by the extent of surgical resection, considering that the larger dissection related to the ERC technique likely requires a longer operative time and slower recovery. In the present study, no differences were found between the two groups in terms of length of hospital stay. For these different outcomes, we should mention that we compared elective and emergent surgeries using the open or laparoscopic approaches, which could explain, to some degree, the existence of heterogeneity among the studies.
Regarding long-term outcomes, there was no difference in terms of recurrence and long-term survival between the groups. In our study, there were no differences between the two groups in terms of 3-year OS, 5-year OS, 3-year DFS, and 5-year DFS. In the study by Odermatt et al., 21 the trend toward a worse survival for patients undergoing extended right colectomy in the univariate analysis was likely to be because this procedure was predominately chosen for high-risk emergencies and in patients with higher ASA scores; indeed, when adjusted in the Cox regression model, this trend converged to the opposite trend, showing a trend toward better survival in the RC group. This trend may also be explained by a more radical approach to the middle colic vessels, as this is the most distinct difference between the two procedures.
Our study had several limitations. Due to the reduced number of RCTs, there was a lack of some outcomes, such as functional outcomes, and a lack of suitable follow-up for oncological data. Additionally, we included both elective and emergent resections using open or laparoscopic approaches, as the number of papers is limited. We included additional CCTs with a risk of selection bias and low to moderate heterogeneity between the studies, highlighting the need for additional RCTs on this topic. The quality of the evidence was limited. We assessed the risk of bias using different tools to alleviate this issue. Therefore, our findings should be interpreted with caution. Making firm conclusions about the treatment of splenic flexure carcinoma is challenging given the small number of studies conducted to date and the variety of techniques used, according to the surgeon’s choice. Additional long-term data in the context of standardized surveillance protocols may provide better answers. Furthermore, the use of laparoscopy or open surgery and the difference in the tumour stage of the included patients should be considered. More prospective and randomized clinical trials are required.
Conclusions
These findings suggest that while ERC may offer some advantages over LC, the choice of surgical technique should be tailored to the individual patient, considering the lack of significant differences in postoperative outcomes and long-term survival. The limited evidence base, characterised by non-randomized studies and potential biases, underscores the need for further high-quality randomised controlled trials to definitively determine the optimal surgical strategy for splenic flexure adenocarcinoma.
Supplemental Material
Supplemental Material - Comparative Efficacy and Long-Term Oncological Safety of Extended Right Hemicolectomy Versus Left Colectomy for Splenic Flexure Adenocarcinoma: A Systematic Review and Meta-Analysis
Supplemental Material for Comparative Efficacy and Long-Term Oncological Safety of Extended Right Hemicolectomy Versus Left Colectomy for Splenic Flexure Adenocarcinoma: A Systematic Review and Meta-Analysis by Mohamed Ali Chaouch, Bassem Krimi, Amine Gouader, Hanen Bhiri, Elise Barel, and Faiza Khemissa Akouz in Cancer Control.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
All data generated or analysed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.