
Abstract
Purpose
This systematic review and meta-analysis aimed to compare outcomes between stapled ileal pouch-anal anastomosis (IPAA) and hand-sewn IPAA with mucosectomy in cases of ulcerative colitis and familial adenomatous polyposis.
Methods
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Review and Meta-analysis) guidelines 2020 and AMSTAR 2 (Assessing the methodological quality of systematic reviews) guidelines. We included randomized clinical trials (RCTs) and controlled clinical trials (CCTs). Subgroup analysis was performed according to the indication for surgery.
Results
The bibliographic research yielded 31 trials: 3 RCTs, 5 prospective clinical trials, and 24 CCTs including 8872 patients: 4871 patients in the stapled group and 4038 in the hand-sewn group. Regarding postoperative outcomes, the stapled group had a lower rate of anastomotic stricture, small bowel obstruction, and ileal pouch failure. There were no differences between the 2 groups in terms of operative time, anastomotic leak, pelvic sepsis, pouchitis, or hospital stay. For functional outcomes, the stapled group was associated with greater outcomes in terms of seepage per day and by night, pad use, night incontinence, resting pressure, and squeeze pressure. There were no differences in stool Frequency per 24h, stool frequency at night, antidiarrheal medication, sexual impotence, or length of the high-pressure zone. There was no difference between the 2 groups in terms of dysplasia and neoplasia.
Conclusions
Compared to hand-sewn anastomosis, stapled ileoanal anastomosis leads to a large reduction in anastomotic stricture, small bowel obstruction, ileal pouch failure, seepage by day and night, pad use, and night incontinence. This may ensure a higher resting pressure and squeeze pressure in manometry evaluation.
Protocol Registration
The protocol was registered at PROSPERO under CRD 42022379880.
Keywords
Introduction
Ileal-pouch anal anastomosis (IPAA) is primarily employed in the treatment of ulcerative colitis (UC) and familial adenomatous polyposis (FAP). 1 Since its initial description by Parks et al in 1978, 2 the procedure has undergone several technical modifications. Restorative proctocolectomy is also referred to as IPAA or pelvic pouch. This procedure can be performed in 1, 2, or 3 stages. 3 The rectal stump can be replaced with a “J,” “W,” or “S" or S pouch. The most recent modification involves preserving the anal transitional zone and using a stapled device for IPAA. Subsequently, 2 types of IPAA have been suggested: 1 involving mucosectomy of the rectal stump followed by a hand-sewn IPAA, and the other utilizing a stapled IPAA without mucosectomy. Since both UC and FAP are mucosal diseases, mucosectomy allows for removal of the diseased colon and rectal mucosa. 4 In the case of stapled anastomosis, it is essential to preserve the anal transitional zone, in contrast to traditional hand-sewn anastomosis. 5 This approach offers the advantage of being quicker with less manipulation of the anal canal. 6 The choice between these 2 techniques remains controversial. In the case of hand-sewn anastomosis, mucosectomy necessitates manipulation of the anal canal, increasing the risk of sphincter damage and alterations in anal sphincter pressure. 6 In the case of stapled anastomosis, mucosectomy is not performed, as it is based on the rationale that the mucosa of the anal transitional zone has rich sensory innervation, which plays a role in anal sphincter function, distinguishing between flatus and stool and contributing to the maintenance of the anorectal inhibitory reflex. However, proponents of hand-sewn anastomosis with mucosectomy emphasize the risk of residual inflamed mucosa affecting short-term outcomes and the risk of dysplasia and cancer affecting long-term outcomes and oncological safety. Many studies have compared these data,7,8 but their results have been controversial, underscoring the importance of this systematic review and meta-analysis.
The purpose of this systematic review and meta-analysis is to compare the outcomes of stapled IPAA vs hand-sewn IPAA in patients undergoing restorative proctocolectomy for UC and FAP in terms of postoperative outcomes, functional outcomes, and oncological safety.
Methods
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines 2020 1 and AMSTAR 2 (Assessing the methodological quality of systematic reviews) guidelines. 2 The protocol was registered at PROSPERO under CRD 42022379880.
Electronics Searches
We conducted bibliographic research on January 30, 2023, using the following sources: The National Library of Medicine through PubMed, Cochrane database, and Google Scholar. The Keywords used were “proctocolectomy,” “ileal pouch-anal anastomosis,” “ulcerative colitis,” “restorative proctocolectomy,” “pelvic pouch,” “functional outcomes,” “stool frequency,” “seepage,” “pad usage,” “incontinence,” “quality of life,” “dysplasia,” “inflammation,” “dysplasia,” “anastomosis,” “complications,” “morbidity,” “mortality,” “anastomotic leak,” “pelvic sepsis,” “anastomotic stricture,” “pouch related stricture,” “small bowel obstruction,” “pouchitis,” “anorectal physiology,” “impotence,” “meta-analysis,” “review,” “controlled clinical trial” and “randomized clinical trial.” We manually checked the reference lists of the relevant reviews for additional citations.
Inclusion and Exclusion Criteria
We retained randomized and controlled clinical trials, irrespective of their publication status or language, including adult patients who underwent IPAA using a stapled anastomosis or handsewn anastomosis with mucosectomy. Only articles published in peer-reviewed journals were included in this study.
Outcomes Measures
The primary outcome was postoperative findings. We assessed the postoperative complications during the follow-up period. The secondary outcomes were the functional and oncological outcomes.
Data Extraction
Two authors extracted the data independently, and senior authors settled the disparities after discussion.
Assessment of Studies Quality and Risk of Bias Assessment
Two authors independently appraised all the studies that met the selection criteria. Concerning quality assessment, CCTs and RCTs were assessed according to the methodological index of non-randomized studies (MINORS) 3 and Consolidated Standards of Reporting Trials (CONSORT) statement, 4 respectively. We excluded all studies with a MINORS or CONSORT statement inferior to 13. For the risk of bias in the RCTs, we used the Cochrane tool for bias assessment to assess the risk of bias in randomized trials (ROB2). 5 We evaluated bias in 5 distinct domains (randomization process, deviations from intended interventions, bias in the measurement of outcome, bias to missing outcome data, bias in selecting the reported results, and overall bias). Within each domain, 1 or more signaling questions led to judgments of “low risk of bias,” “some concerns,” or “high risk of bias” high risk of bias. The Newcastle-Ottawa Scale (NOS) was used to assess the risk of bias in CCTs. 6
Data analysis
The analysis of continuous data was performed using the statistical software Review Manager 5.3.5, developed by the Cochrane Collaboration, specifically for conducting meta-analyses. 7 If the mean and standard deviation (SD) values were not directly available, they were inferred from the median and interquartile range (IR) using the estimation method proposed by Hozo et al. 8 For instances in which the sample size exceeded 25, it was assumed that the median and mean values were equivalent. Furthermore, for sample sizes below 70, the SD was approximated by dividing the IR by 4, and for those above 70, by dividing the IR by 7.
Evaluating Study Heterogeneity
The examination of heterogeneity in the studies involved a three-pronged approach: Application of the Cochrane Q-test (Chi2 test), analysis of Tau2 (true effect variance), and calculation of a 95% predictive interval to gauge the extent of heterogeneity, 9 utilizing the Comprehensive Meta-analysis software for predictive interval determination. Employing funnel plots for visual heterogeneity analysis. 10 Sensitivity checks were conducted through subgroup analyses, where relevant. 11 In scenarios where significant heterogeneity was detected, particularly in studies grouped under Ulcerative Colitis (UC) and Familial Adenomatous Polyposis (FAP), a detailed subgroup analysis was undertaken, segregating studies focused solely on UC or FAP from those encompassing both conditions.
Synthesizing study findings
Two researchers independently evaluated the evidence related to primary outcomes using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) methodology. 12 This included the consideration of study limitations, consistency of effect, accuracy, relevance, and potential publication bias. The certainty of the evidence was categorized as high, moderate, low, or very low. Enhancements to evidence strength were considered under circumstances of significant effect, dose-response correlation, or plausible confounding. The assessment followed the procedures outlined in sections 8.5 and 8.7 and chapters 11 and 12 of the Cochrane Handbook for Systematic Reviews of Interventions. The GRADEpro GDT software facilitated the preparation of the Summary of Findings tables, with detailed rationales for any downgrading or upgrading decisions provided in the footnotes.
Determining the Magnitude of Effects for Meta-Analysis
The RevMan 5.4 software, provided by the Cochrane Collaboration, was utilized. 7 The mean difference (MD) was chosen as a measure of continuous data. In the case of binary outcomes, odds ratios (OR) and 95% confidence intervals (95% CI) were calculated. A random-effects model was used for these calculations, with a significance threshold of .05.
Results
Bibliographic Research
The bibliographic research yielded 36 trials (Figure 1). Five studies were excluded for the following reasons13-16: 1 study included patients undergoing stapled anastomosis and compared high with low anastomosis,
13
1 study included only patients undergoing a hand-sewn anastomosis,
14
1 study included patients with rectal cancer,
15
1 study compared the outcomes of the reversal loop ileostomy,
16
and 1 study was a narrative review.
17
We then retained 31 trials18-48: 3 RCTs,39,40,44 5 prospective clinical trials,19-23 and 24 CCTs.18,24-38,41-43,45-48 The demographic data of the studies are summarized in Table 1. These studies included 8872 patients, 4871 patients in the stapled group, and 4038 hand-sewn group, and were published between 1991 and 2022. PRISMA flow-diagram of the bibliographic research. List of the Retained Studies. Nbre: number; retro: retrospective; comp: comparative; pros: prospective; Random: randomized; N: total number of patients; SA: stapled anastomosis; HA: hand-sewn anastomosis; M: male; F: female; FAP: familial adenomatous polyposis, UC: ulcerative colitis; IC: indeterminate colitis; CD: crohn disease.

Operative Time
Operative time was reported in 6 studies. It was estimated in 472 patients (178 in the stapled group and 293 in the hand-sewn group). There was no significant difference between the 2 groups (MD = −12.59; IC95% [−49.24, 24.07]; P = .5). There was a high heterogeneity among the studies.
Anastomosis Leak
Anastomotic leaks were reported in 14 studies. It was reported in 62 of 1372 patients in the stapled group and 123 of 1522 patients in the handsewn group. There was no significant difference between the 2 groups (OR = .84; IC95% [.58, 1.21]; P = .34).
Pelvic Sepsis
Pelvic sepsis was reported in 17 studies. It was estimated in 7526 patients, occurring in 560 of 4047 patients in the stapled group and 293 of 3479 patients in the hand-sewn group. There was no significant difference between the 2 groups (OR = .85; IC95% [.60, 1.19]; P = .34). There was little heterogeneity among these studies.
Pouchitis
Pouchitis was reported in 11 studies. It was estimated in 4108 patients, occurring in 1133 of 3087 patients in the stapled group and 384 of 1021 patients in the hand-sewn group. There was no significant difference between the 2 groups (OR = .59; IC95% [.35, 1.01]; P = .05). There was little heterogeneity among these studies.
Anastomotic Stricture
The Anastomotic structure was reported in 15 studies (Figure 2). It was estimated in 4816 patients, occurring in 496 of 3489 patients in the stapled group and 242 of 1327 patients in the hand-sewn group. There was a lower rate of anastomotic strictures in the stapled group (OR = .53; IC95% [.35, .81]; P = .003). There was little heterogeneity among the studies (Tau2 = .19(I2 = 39%)). In the UC and UC + FAP subgroup analyses, we found a significantly lower rate of anastomotic stricture in the stapled group than in the hand-sewn group (OR = .26; IC95% [.09, .73]; P = .01) and (OR = .60; IC95% [.42, .87]; P = .006), respectively. For the FAP subgroup, there was no difference between the 2 groups (OR, .69; IC95% [.18, 2.54]; P = .57). Forest plot of anastomotic stricture.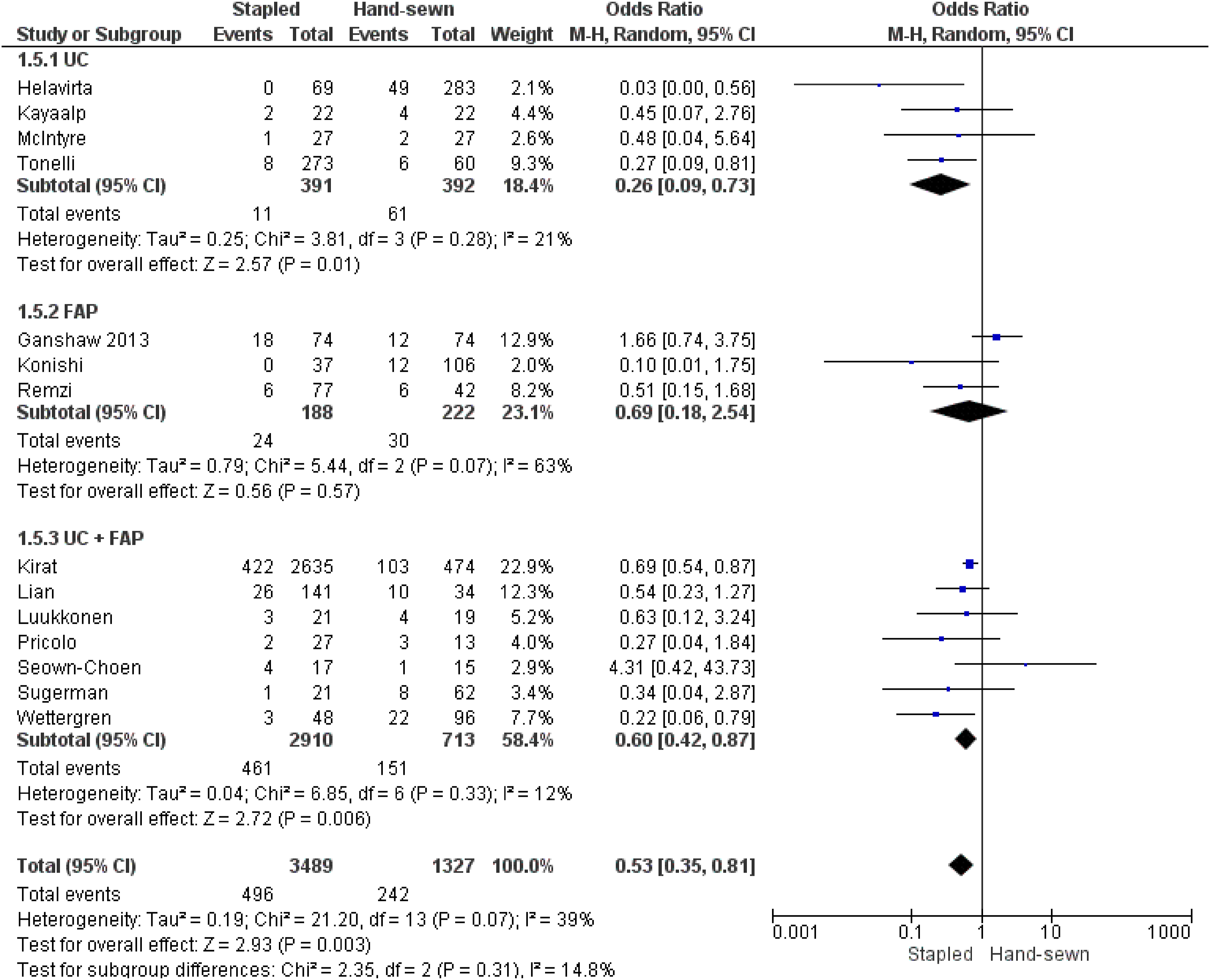
Small Bowel Obstruction
Small-bowel obstruction was reported in 12 studies. It was estimated in 4524 patients, occurring in 572 of 3367 patients in the stapled group and 203 of 1157 patients in the hand-sewn group. The stapled group had a lower rate of small bowel obstruction (OR = .79; IC95% [.65, .97]; P = .02).
Ileal Pouch Failure
Ileal pouch failure was reported in ten studies. It was estimated in 5110 patients, occurring in 135 of 3825 patients in the stapled group and 99 of 1285 patients in the hand-sewn group. A lower rate of ileal pouch failure was observed in the stapled group (OR = .32; IC95% [.23, .43]; P < .00001).
Hospital Stay
Hospital stay was reported in 4 studies. It was estimated in 3447 patients: 2875 in the stapled group and 572 in the hand-sewn group. There was no significant difference between the 2 groups (MD = .51; IC95% [−1.94, 2.97]; P = .59). There was a low heterogeneity among the studies.
Stool Frequency Per 24h
The stool frequency per 24h was reported in 14 studies. It was estimated that there were 4445 patients: 3347 in the stapled group and 1098 in the hand-sewn group. There was no significant difference between the 2 groups (MD = .14; IC95% [−.29, .56]; P = .53). There was little heterogeneity among these studies.
Stool Frequency at Night
Stool frequency at night was reported in 7 studies. It was estimated in 3808 patients: 3093 in the stapled group and 715 in the hand sewn group. There was no significant difference between the 2 groups (OR = .05; IC95% [−.41, .50]; P = .84). There was little heterogeneity among these studies. In the UC + FAP subgroup analysis, we found a significantly lower rate of stool frequency in the handsewn group than in the stapled group (OR = .3; IC95% [.15, .45]; P < .0001). For the UC and FAP subgroups, there were no differences between the 2 groups (OR = .01; IC95% [−.88, .89]; P = .99) and (OR = −.10; IC95% [−.71, .51]; P = .75), respectively.
Seepage by Day
Seepage by Day was reported in 4 studies. It was estimated in 3356 patients: occurring in 441 of 2787 patients in the stapled group and 173 of 569 patients in the hand-sewn group. There was a lower rate of seepage per day in the stapled group (OR = .41; IC95% [.25, .66]; P = .0003). There was little heterogeneity among these studies.
Seepage by night
Seepage by night was reported in 5 studies. It was estimated in 3345 patients: occurring in 765 of 2789 patients in the stapled group and 270 of 556 patients in the hand-sewn group. There was a lower rate of seepage at night in the stapled group (OR, .38; IC95% [.20, .72]; P = .003). There was little heterogeneity among these studies.
Pad Use
The Use of a pad was reported in 8 studies. It was estimated in 3504 patients, occurring in 429 of 2864 patients in the stapled group and 196 of 640 patients in the hand-sewn group. There was a lower pad use rate in the stapled group (OR = .42; IC95% [.30, .60]; P < .00001).
Pad Use Per day
The use of pads per day was reported in 4 studies. It was estimated in 3559 patients: occurring in 399 of 2807 patients in the stapled group and 204 of 752 patients in the hand-sewn group. There was a lower rate of daily pad use in the stapled group (OR = .36; IC95% [.27, .49]; P < .00001).
Pad Use Per Night
The use of pads per night was reported in 3 studies. It was estimated in 3522 patients, occurring in 486 of 2778 patients in the stapled group and 290 of 744 patients in the hand-sewn group. There was a lower rate of overnight pad use in the stapled group (OR = .29; IC95% [.24, .35]; P < .00001).
Night Incontinence
Night incontinence was reported in 12 of the studies. It was estimated in 4217 patients, occurring in 130 of 3250 patients in the stapled group and 196 of 967 patients in the hand-sewn group. There was a lower rate of night incontinence in the stapled group (OR, .37; IC95% [.27, .51]; P < .00001).
Antidiarrheal Medication
Antidiarrheal medication was reported in 6 studies. It was estimated in 581 patients, occurring in 43 patients out of 201 in the stapled group and 131 380 patients in the hand-sewn group. There was no significant difference between the 2 groups (OR = .62; IC95% [.32, 1.21]; P = .16). There was little heterogeneity among these studies.
Sexual Impotence
Sexual impotence was reported in 6 studies. It was estimated in 3432 patients, occurring in 346 of 2818 patients in the stapled group and 97 of 614 patients in the hand-sewn group. There was no significant difference between the 2 groups (OR = .70; IC95% [.30, 1.65]; P = .41). There was little heterogeneity among these studies.
Resting Pressure
Resting pressure was reported in 7 studies. It was estimated that there were 293 patients: 166 in the stapled group and 127 in the hand-sewn group. There was a greater value of resting pressure associated with the stapled group (MD = 14.74; IC95% [9.58, 19.9]; P < .00001). Moderate heterogeneity was observed among the studies.
Squeeze Pressure
The squeeze pressure was reported in 6 studies. It was estimated in 261 patients (146 in the stapled group and 115 in the hand-sewn group). There was a greater value of squeeze pressure in the stapled group (MD = 21.78; IC95% [5.67, 7.88]; P = .008). Significant heterogeneity was observed among the studies.
Length of the High-Pressure Zone
The length of the high-pressure zone has been reported in 5 studies. It was estimated that there were 229 patients: 135 in the stapled group and 94 in the hand-sewn group. There was no significant difference between the 2 groups (MD = .27; IC95% [−.06, .60]; P = .11). There was little heterogeneity among these studies.
Dysplasia
Dysplasia was reported in 3 studies. It was estimated in 300 patients, occurring in 69 of 186 patients in the stapled group and 28 of 114 patients in the hand-sewn group. There was no difference between the 2 groups (OR, 1.62; IC95% [.73, 3.58]; P = .24). There was little heterogeneity among these studies.
Neoplasia
Neoplasia was reported in 3 studies. It was estimated in 300 patients, occurring in 20 of 186 patients in the stapled group and 10 of 114 patients in the hand-sewn group. There was no difference between the 2 groups in terms of neoplasia (OR, .63; IC95% [.24, 1063]; P = .34).
Quality Assessment of the Included Studies and Reporting of the Effects of Stapled Ileoanal Anastomosis
The quality assessment and risk of bias are presented in Table 2. The results of the pooled analyses are presented in Table 3. A Summary of the evidence is presented in Table 4. This review shows that stapled ileoanal anastomosis is superior to hand-sewn anastomosis. • This leads to a large reduction in anastomotic stricture, small bowel obstruction, ileal pouch failure, seepage by day and night, pad use, and night incontinence. • It may ensure a higher resting pressure and squeeze pressure in the manometry evaluation. • We do not know if it leads to additional anastomotic leak, pelvic sepsis, pouchitis, sexual dysfunction, antidiarrheal medication, length of high-pressure zone, operative time, hospital stay, stool frequency, dysplasia, and neoplasia because the evidence is very uncertain. Quality Assessment and Risk of Bias in the Retained Studies. Nbre: number; CONSORT: Consolidated Standards of Reporting Trials; MINORS: methodological index of non-randomized studies; retro: retrospective; comp: comparative; pros: prospective; Random: randomized. Outcomes of the Pooled Analysis. Summary of Findings Table. * Explanations. aSmall sample size of the included patients. bExisting of a heterogeneity among the different studies.



Discussion
This systematic review and meta-analysis concluded that the stapled group had better outcomes than the hand-sewn group in terms of anastomotic stricture, small bowel obstruction, ileal pouch failure, seepage by day and night, pad use, night incontinence, resting pressure, and squeeze pressure in the manometry evaluation. It was also concluded that there were no differences between the 2 groups in terms of anastomotic leak, pelvic sepsis, pouchitis, sexual dysfunction, antidiarrheal medication, length of high-pressure zone, operative time, hospital stay, stool frequency, dysplasia, and neoplasia.
Operative time is a critical factor in evaluating surgical techniques. Our systematic review and meta-analysis found no significant difference in operative time between stapled and hand-sewn ileal pouch-anal anastomosis (IPAA) procedures.1-6 This aligns with the results of 4 of the 6 studies we reviewed. The heterogeneity in these studies may be attributed to the lack of standardized measurement tools and limited data on the surgeon’s experience. Additionally, most studies were retrospective and lacked clear patient allocation information. Anastomotic leaks, particularly in the lower gastrointestinal tract, are a significant concern (56). Our study revealed a lower relative incidence of anastomotic leak in the stapled group than in the hand-sewn group,7-11 which may be attributed to the tension-free anastomosis with stapling. Hand suturing resulted in a lower anastomosis placement relative to the dentate line, potentially leading to ischemia and anastomotic stricture. However, subgroup analysis showed no difference between the 2 techniques in studies involving familial adenomatous polyposis (FAP) patients,27,44,48 likely due to the limited number of studies and heterogeneity in the definition of strictures at the IPAA. The higher use of diverting stomas in the hand-sewn group may also have contributed to this heterogeneity. In addition, several factors that were not assessed in our study affected the outcomes. Many patients undergoing intestinal surgery are elderly, and vascularization tends to decrease with advancing age, often due to atherosclerosis. Unfortunately, low cardiac output was a common occurrence, particularly in ‘fragile’ patients who frequently required at least 1 day of intensive care or were managed in the wards. These patients were often classified by anesthesiologists as ASA class 3. Low cardiac output can lead to a temporary reduction in intestinal blood flow, a condition known as Non-occlusive Mesenteric Ischemia (NOMI). 49 This may contribute to anastomotic dehiscence, irrespective of whether anastomosis is performed manually or mechanically. 49
Regarding small bowel obstruction,12-23 our study, which included data from 12 studies, demonstrated a lower rate of small bowel obstruction in the stapled group. Ileal pouch failure and pouchitis can lead to complications and revision surgery. Our findings were consistent with those of Kirat et al., 43 who identified the type of anastomosis as a risk factor for pouchitis. However, the significance of these findings remains uncertain. Ileoanal anastomosis modifies anatomy and has functional consequences, including seepage per day and night incontinence.24-26 Our study indicated a lower rate of daily seepage in the stapled group. Patients in the stapled group also used fewer pads (29, 46, 47, 51). Antidiarrheal medication use did not differ significantly between the 2 techniques (29, 42, 48, 52, 53). Six studies evaluated sexual impotence (29, 40, 42, 43, 48, 52), and the results were in line with Kirat et al's findings, suggesting that sexual function may be more affected by proctectomy and pelvic nerve damage than by IPAA type. However, further research using validated questionnaires is needed to reduce the subjectivity in assessing this outcome. Functional factors, such as stool frequency, consistency, urgency, and incontinence, were considered, but these remain subjective measures. Manometry measures, including resting pressure, squeeze pressure, and the length of the high-pressure zone, were analyzed in 7 studies.1,26,38,46,47,49 Our findings favored the stapled technique, potentially due to better sphincter and perianal nervous system preservation. Residual rectal mucosa is a concern in patients with UC and FAP after IPAA due to the risk of colorectal cancer. 35 Mucosectomy for UC aims to eliminate mucosal inflammation and the risk of malignant transformation. Hand-sewn anastomosis with mucosectomy may be more challenging, but offers a definitive cure. For patients with FAP, residual rectal mucosa can lead to polyposis, dysplasia, and neoplasms (63). Our study found no significant difference in dysplasia rates between stapled and hand-sewn anastomoses.31,35,48 The risk of cancer recurrence after mucosectomy was noted, possibly because of incomplete rectal mucosa removal. A portion of patients in the hand-sewn group had remnant rectal mucosa. Mucosectomy can reduce the risk, but does not entirely eliminate it.
Our study had several limitations. Owing to the reduced number of RCTs, the lack of some outcomes, and the lack of suitable follow-up. We did not assess other outcomes, such as cuffitis, in the UC population because they were not reported in the majority of studies. We included additional CCTs with a risk of selection bias and low-to-moderate heterogeneity between the studies, highlighting the need for additional RCTs on this topic. However, the quality of evidence is limited. We assessed the risk of bias using different tools. Therefore, our findings should be cautiously interpreted. Making firm conclusions for dealing with rectal cancer or dysplasia is challenging, given the small number of studies conducted to date. In addition, for several studies, the follow-up was limited and did not provide strong recommendations in terms of oncological safety. Additional long-term data in the context of standardized surveillance protocols may provide better answers. In addition, there may be concerns about introducing bias by including UC and FAP. These 2 diseases have different clinical presentations, etiology, preoperative treatment, development of pathology, and recurrence or development of cancer. To alleviate this issue, we performed a subgroup analysis of patients with UC and FAP, when possible.
Conclusions
In conclusion, both anastomoses had advantages and disadvantages. Additional RCTs with larger sample sizes and longer follow-up periods seem to be mandatory for a greater placement of stapled IPAA in the therapeutic armature of UC and PAF to investigate which patients need stapled or handsewn IPAA.
Footnotes
Author Contributions
Mohamed Ali Chaouch, Mohammad Iqbal Hussain, Amine Gouader, Bassem Krimi and Alessandro Mazzotta wrote the main manuscript text and Adriano Carneiro Da Costa, Niccolo Putricciani and Hani Oweira checked the statistical analysis. All authors reviewed the manuscript and validate the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
All data generated or analyzed during this study are included in this published article.