
Abstract
Objective
This study ascertained current status and influencing factors of readiness for hospital discharge (RHD) of lung cancer (LC) patients with enhanced recovery after surgery (ERAS) concept-guided postoperative management.
Methods
This study prospectively and consecutively included 217 LC patients who underwent whole-course ERAS concept-guided postoperative management at the Department of Thoracic Surgery of Guangzhou Institute of Cancer Research, the Affiliated Cancer Hospital, Guangzhou Medical University from November 2023 to April 2024. RHD, quality of discharge teaching (QDT), and social support (SS) were evaluated using RHDS, QDTS, and SSRS, followed by correlation analyses of RHD with the other 2 factors. The clinical baseline and pathological data were compared between the high and low RHD groups, and the characteristics showing statistical significance were assigned as independent variables for regression analysis with RHD as the dependent variable.
Results
RHD, QDT, and SS were above average among LC patients with ERAS concept-guided postoperative management, and RHD was positively correlated with both QDT and SS. Age, education level, self-care ability, number of admissions, and presence of drainage tubes were independent influence factors for RHD of LC patients with ERAS concept-guided postoperative management.
Conclusion
In LC patients with ERAS concept-guided postoperative management, RHD may be improved by increasing QDT and SS and intervened by factors such as age, education level, self-care ability, number of admissions, and presence of drainage tubes.
Keywords
Introduction
As reported by GLOBOCAN 2020, lung cancer (LC) is still the leading reason for cancer mortality, with an estimated mortality rate of 18%. 1 Clinical care has an auxiliary role in the recovery of LC patients that is dominated by pain relief and comfort enhancement, but continuous care is still needed after hospital discharge, with varying levels of post-discharge care. 2 Therefore, LC patients should be provided with high-quality, efficient, and continuous care to assure and increase their quality of life after hospital discharge. The concept of enhanced recovery after surgery (ERAS) is formulated based on evidence-based protocols for optimizing care, where caregivers provide targeted, scientific, and comprehensive care as per the demands of individuals. 3 In recent years, the application of ERAS in the field of thoracic surgery (particularly lung surgery) has achieved certain clinical efficacy, effectively shortening the hospitalization time of patients and accelerating their recovery. 4 Therefore, the ERAS concept deserves further investigation in the domain of LC.
Readiness for hospital discharge (RHD) is a standard assessment criterion for the patient physical, psychological, and social health (including the perception of feeling prepared to leave the hospital, ability to reintegrate into society, and degree of rehabilitation), which contributes to the reasonable provision of effective care for patients after leaving the medical institution. 5 RHD assessment is beneficial for rationally scheduling the discharge of patients, thereby preventing the discharge of patients without physical recovery, reducing the incidence of post-discharge complications and readmission, and saving medical costs and resources. 6 Patients with higher RHD have a stronger responsive ability against their disease and a relatively lower risk of readmission.7,8 A prior study assessed RHD in patients with colorectal cancer (CRC) who underwent ERAS-guided management to remind medical staff improving the quality of discharge guidance. 9 However, few studies paid attention to RHD in LC patients receiving ERAS-guided postoperative management. Accordingly, this study ascertained the current status of RHD of LC patients who underwent whole-course postoperative management guided by the ERAS concept and analyzed the influencing factors of RHD in such patients, thereby offering new ideas for clinical postoperative care of LC patients based on the ERAS concept and a new entry point for the improvement of their RHD.
Materials and Methods
Study Subjects
This study prospectively and consecutively included 257 LC patients admitted to the Department of Thoracic Surgery of Guangzhou Institute of Cancer Research, the Affiliated Cancer Hospital, Guangzhou Medical University from November 2023 to April 2024 for whole-course management guided by the ERAS concept. Moreover, 28 patients who did not fulfill the inclusion criteria and conformed to exclusion criteria and 12 patients who were reluctant to participate in the study and withdrew halfway were excluded. Eventually, this study included 217 LC patients undergoing whole-course ERAS-guided management. The flowchart is shown in Figure 1. Baseline clinical and pathological data of all patients were collected and summarized, such as gender, age, education level, marital status, self-care ability, place of residence, employment status, number of hospital admissions, monthly per-capita family income, primary caregiver, presence of health insurance, comorbidities, length of stay (LOS), surgical method, and presence of drainage tubes. The reporting of this study conforms to STROBE guidelines.
10
The study complied with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Guangzhou Institute of Cancer Research, the Affiliated Cancer Hospital, Guangzhou Medical University (approval number: GYZL-2023-SW10; approval date: November 22, 2023). Patients and their families signed an informed consent form, and patients voluntarily participated in the study. All patient details were de-identified. Flow chart.
Inclusion and Exclusion Criteria
The following inclusion criteria were used: (1) patients over 18 years of age; (2) patients diagnosed with LC by histopathological examinations and other examinations 6 ; (3) patients undergoing elective surgery and receiving whole-course ERAS-guided management in the perioperative period; and (4) patients who gave informed consent to this study and participated voluntarily. Patients matching the following criteria were excluded: (1) patients complicated with severe organic diseases or other malignant tumors; (2) patients with language communication barriers or inability to fill out the questionnaire; (3) patients with incomplete data.
ERAS-Guided Nursing
A team of ERAS concept-guided nursing interventions was built with an experienced senior head nurse as the team leader. Nursing staff in the department received regular training for postoperative nursing of LC and ERAS-related knowledge, and they were assessed according to the learning progress. The temperature of patients was supervised intraoperatively, and the temperature of the operating room was controlled at around 23°C. Patients with hypothermia were provided with insulation blankets and infused fluids to maintain the temperature at 37.5°C and ensure a constant temperature. Patients were anesthetized with thoracic paravertebral block combined with general anesthesia, during which the dosages of vecuronium bromide (0.1 mg/kg), etomidate (0.2 mg/kg), midazolam (0.1 mg/kg), and sufentanil (0.5 μg/kg) were strictly controlled 11 to avoid the prolongation of the postoperative extubation time. The thoracic pressure of patients was adjusted through closed drainage of thoracic cavity, and the amount, color, and shape of the drainage fluids were closely monitored. As prescribed, patients were routinely intravenously infused with flurbiprofen Axetil Injection (100 mg, twice daily) for analgesia. 11 Medical staff and family members encouraged patients to move out of bed as early as possible and receive relevant rehabilitation training. 12 When the patients were able to take a deep breath, hold their breath, and had a drainage volume of less than 150 mL/24 h, good pulmonary dilation by chest X-ray and no leakage, bleeding, and chylothora, the drainage tube was removed13,14; on the contrary, the drainage tube could not be removed.
RHD Assessment
The RHD of patients was assessed with the Readiness for Hospital Discharge Scale (RHDS), which was originally developed in Chinese by Weiss et al. 15 and translated and modified by Wang et al. 16 The Cronbach’s α coefficient of this scale was .756. The scale mainly covered 3 dimensions, including anticipatory support, coping ability, and personal status, with a total of 12 items (each item was scored 0-10 points) and a total score ranging from 0 (low readiness) to 120 (high readiness). A score of below 50 points represented low RHD, a score of 50-70 points denoted medium readiness, and a score of above 70 points corresponded to high readiness. The obtained score was positively related to RHD.
QDT Assessment
QDT was assessed with the Quality of Discharged Teaching Scale (QDTS). The Cronbach’s α coefficient of this scale was .856. The scale involved 3 dimensions (teaching skills and effectiveness, teaching content actually obtained, content needed before discharge), with a total of 24 items (each item was scored 0-10 points). A score of <180 points was considered low QDT, a score of 180-210 points marked medium quality, and a score of >210 points indicated high quality. The score was positively related to QDT.
SS Assessment
The Social Support Rating Scale (SSRS) was utilized to assess SS, with a Cronbach’s α coefficient of .628. This scale covered 3 dimensions, namely subjective support (4 items), objective support (3 items), and utilization of support (3 items). A score of <50 points represented low SS, a score of 50-70 points suggested medium SS, and a score of >70 points denoted high SS. The score was positively proportional to the degree of SS.
Statistical Analysis
The sample size was estimated by a statistical efficiency-based method using G * Power 3.1.9.7 (University of Dusseldorf, Germany), and the included sample size met the requirements for independent sample t test, Chi-square test, Pearson’s correlation analysis, one-way ANOVA, and logistic regression (Supplementary figure 1A-E). SPSS 20.0 software (IBM, Armonk, NY, USA) was employed for data processing. Count data were summarized as frequencies and percentages and analyzed with the chi-square test. All data were normally distributed following the Shapiro-Wilk test. Measurement data were displayed as mean ± standard deviation and analyzed with the independent samples t test or one-way ANOVA. Pearson correlation analyses were carried out to assess the correlations of RHD with QDT and SS. Influencing factors for RHD of LC patients undergoing whole-course ERAS-guided postoperative management were determined with multivariate logistic regression. The test level was α = .05, with P < .05 denoting statistically significant differences.
Results
Relationship Between Baseline Clinicopathological Data and RHDS Scores
Demographic Characteristics and RHD Scores.
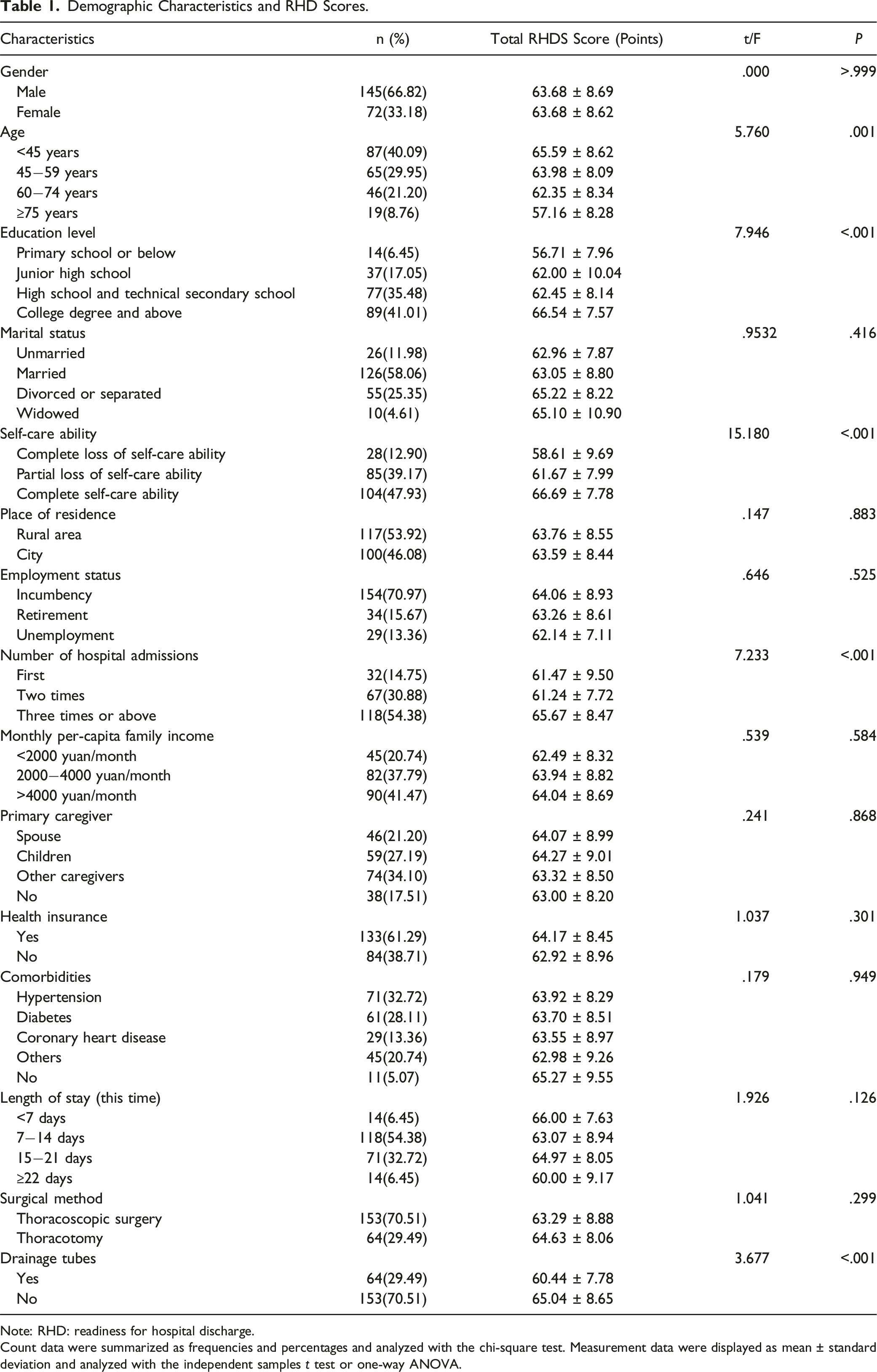
Note: RHD: readiness for hospital discharge.
Count data were summarized as frequencies and percentages and analyzed with the chi-square test. Measurement data were displayed as mean ± standard deviation and analyzed with the independent samples t test or one-way ANOVA.
Current Status of RHD, QDT, and SS in LC Patients Receiving Whole-Course ERAS-Guided Postoperative Management
The patients had a mean total RHDS score of (63.68 ± 8.65) points, and the mean dimension RHDS score was (5.17 ± .79) points (Figure 2(A) and (B)). The patients had a mean total QDTS score of (202.23 ± 9.64) points, and the mean dimension QDTS score was (8.18 ± .44) points (Figure 2(C) and (D)). The patients showed a mean total SSRS score of (63.88 ± 8.86) points and a mean dimension SSRS score of (6.37 ± .94) points (Figure 2(E) and (F)). Overall, RHDS, QDTS, and SSRS scores were above average for patients receiving whole-course postoperative management guided by the ERAS concept. Distribution of total RHDS, QDTS and SSRS scores and mean scores at each dimension in LC patients receiving whole-course ERAS-guided postoperative management. Note: (A) Total RHDS score distribution; (B) mean RHDS score distribution at all dimensions; (C) total QDTS score distribution; (D) mean QDTS score distribution at all dimensions; (E) total SSRS score distribution; (F) mean SSRS score distribution at all dimensions. LC: lung cancer; ERAS: enhanced recovery after surgery; RHDS: readiness for hospital discharge scale; QDTS: quality of discharged teaching scale; SSRS: social support rating scale; High: scores are in the high level range; medium: scores are in the medium level range; low: scores are in the low level range.
Relevance of RHD to QDT and SS in LC Patients Receiving Whole-Course ERAS-Guided Postoperative Management
As observed in Figure 3, the total RHDS score was positively correlated with the total QDTS score (r = .429, P < .001) and the total SSRS score (r = .452, P < .001). Correlations of RHD with QDT and SS. Note: (A) Pearson’s correlation analysis between the total RHDS and QDTS scores; (B) Pearson’s correlation analysis between the total RHDS and SSRS scores. ERAS: enhanced recovery after surgery; RHD: readiness for hospital discharge; RHDS: readiness for hospital discharge scale; QDTS: quality of discharged teaching scale; SSRS: social support rating scale; r: signifies the correlation coefficient, and P < .05 indicates a significant difference.
Analysis of Baseline Clinical and Pathological Data of LC Patients Receiving Whole-Course ERAS-Guided Postoperative Management With Different Levels of RHD
Analysis of Baseline Clinicopathological Data of LC Patients Receiving Whole-Course Guided Management Under the ERAS Concept With Different Levels of RHD.
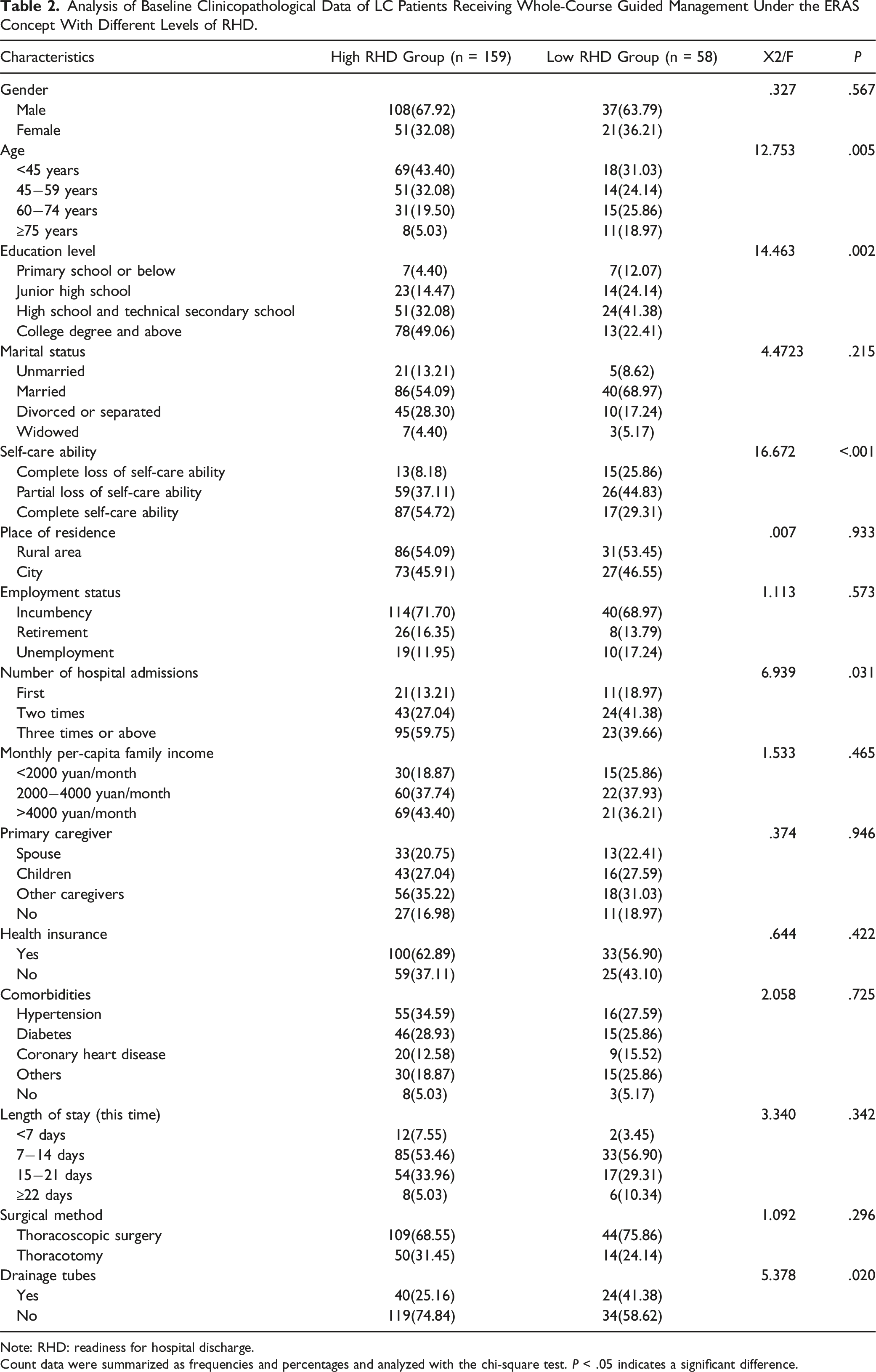
Note: RHD: readiness for hospital discharge.
Count data were summarized as frequencies and percentages and analyzed with the chi-square test. P < .05 indicates a significant difference.
Influencing Factors for RHD in LC Patients Receiving Whole-Course ERAS-Guided Postoperative Management
Assignment Table.

Note: RHD: readiness for hospital discharge.

Forest plot of influencing factors for RHD in LC patients receiving whole-course ERAS-guided postoperative management. Note: The multivariate logistic regression analysis was used to analyze influencing factors for RHD in LC patients receiving whole-course ERAS-guided postoperative management. LC: lung cancer; ERAS: enhanced recovery after surgery; RHD: readiness for hospital discharge; HR: hazard ratio; 95% CI: 95% confidence interval. P < .05 indicates a significant difference.
Discussion
At present, surgery, radiotherapy, and chemotherapy remain the predominant therapeutic options for LC patients. 17 Nevertheless, surgical treatment for LC patients is accompanied by a relatively high complication rate. 18 Accumulating studies have unveiled that the ERAS protocol may diminish the risk of mortality, complication and readmission rates, and postoperative pain level, shorten adjuvant chemotherapy time and LOS, and decrease anesthesia medication amount and hospitalization cost. 19 The postoperative RHD intervention for LC patients based on ERAS is still in its infancy. Herein, this research evaluated the current status of RHD in LC patients receiving whole-course postoperative management guided by the ERAS concept and determined the variables that impact RHD in such patients. Our finding unraveled that increasing the QDT and SS could improve RHD in LC patients receiving ERAS concept-guided management and age, education level, self-care ability, number of hospital admissions, and presence of drainage tubes are influencing factors for RHD.
As a multidisciplinary perioperative care program, the ERAS concept consists of strategies like preoperative education, shortening of fasting time, optimization of anesthesia protocols, and early mobilization, which may foster recovery and increase quality of life.20,21 The ERAS concept primarily focuses on minimizing perioperative stress responses and catabolism, eventually accelerating postoperative recovery, shortening LOS, and lowering morbidity rates. Different from the fast-track concept that only intends to shorten LOS, the ERAS concept integrates various care elements in diverse phases (preoperative, intraoperative, and postoperative) to boost the recovery. 22 Accordingly, ERAS may be a complement to the fast-track concept. As reported, the ERAS concept decreases the postoperative experience of vomiting, pain, nausea, and longer fasting time in contrast to traditional care. 23 Importantly, a recent study showed that the use of of an ERAS pathway improved postoperative outcomes of LC patients receiving surgery, as evidenced by shorter LOS and lower in-hospital costs and complication rates, thus facilitating postoperative recovery of such patients. 24 However, older patients experienced more underlying diseases and patients with lower education levels had slower reception of disease nursing cognition, resulting in poorer RHD. Hence, our study focused on RHD in LC patients receiving ERAS concept-guided management.
RHD can be used to assess the ability of patients to shoulder responsibility for and comply with treatment recommendations at home. 25 RHD shares an association with the health outcomes of patients after they return home. 26 A recent study determined a medium level of RHD in patients with bilateral ureteral stoma after radical cystectomy; it also revealed a positive correlation between the total scores of RHDS and QDTS, 27 which was also demonstrated in our research. Our results displayed that RHD was above average among LC patients undergoing ERAS concept-guided postoperative management. Another study explored RHD in LC patients undergoing chemotherapy and elucidated that gender, marital status, duration of treatment, QDT, and fear of disease progression could affect the RHD. 28 In addition, Yang et al. observed that the total and item scores of RHDS were at a moderate level in CRC patients who underwent the ERAS-based management. They also found correlations of RHD with QDT and discharge to a rehabilitative institution. 9 A prior study has proposed that SS is critical for the QDT and the improvement of RHD in fundus disease patients. 29 However, no studies have evaluated the relation between RHD and SS in LC patients undergoing ERAS concept-guided management. On this basis, our study assessed the relations between RHD and QDT as well as RHD and SS. Accordingly, the RHDS score exhibited a positive correlation with QDTS score as well as SSRS score. Wu et al. noted that the total RHDS score of elderly patients with chronic obstructive pulmonary disease was at a suboptimal level, and that multiple factors such as marital status, admission mode, LOS, and QDT were independent influencing factors for RHD in such patients. 8 Also, an existing study reported that age and education level had an impact on RHD of patients discharged with tubes from the department of hepatobiliary surgery. 30 Similarly, our study screened age, education level, self-care ability, number of hospital admissions, and presence of drainage tubes as the independent variables influencing the RHD of LC patients after whole-course ERAS-guided postoperative management.
Overall, the influencing factors can be studied one by one to further develop a more scientific and personalized nursing plan in the clinic. These findings provide a new entry point for the improvement of RHD of LC patients under the postoperative ERAS management model. Nevertheless, this study presented with several limitations. First, the samples of this study were only from 1 center, and the results may not be generalized to the whole country. Second, the sample size was relatively small, which may affect the reliability of the results. Accordingly, multi-center large-sample research is warranted before generalized conclusion, and a public database will be used as the validation queue to further validate the research results of this paper. Third, this study did not show differences in RHDS scores for different LOS, and sample size selection and self-care ability might impact RHD, which remain to be ascertained in following studies.
Conclusion
This study unveiled that RHD of LC patients undergoing ERAS concept-guided postoperative management was at a level of above average and positively correlated with the QDT and SS. Besides, age, education level, self-care ability, number of hospital admissions, and presence of drainage tubes were identified as the independent influencing variables for RHD of such patients.
Supplemental Material
Supplemental Material - Current Status and Influencing Factors of Readiness for Hospital Discharge of Lung Cancer Patients Receiving ERAS-Guided Postoperative Management
Supplemental Material for Current Status and Influencing Factors of Readiness for Hospital Discharge of Lung Cancer Patients Receiving ERAS-Guided Postoperative Management by Feiyan Zeng, Meihui Sun, Yongdong Li, Tiantian Fan, Xuan Wu, Liyan Wang and Yumei Li in Journal of Cancer Control.
Supplemental Material
Supplemental Material - Current Status and Influencing Factors of Readiness for Hospital Discharge of Lung Cancer Patients Receiving ERAS-Guided Postoperative Management
Supplemental Material for Current Status and Influencing Factors of Readiness for Hospital Discharge of Lung Cancer Patients Receiving ERAS-Guided Postoperative Management by Feiyan Zeng, Meihui Sun, Yongdong Li, Tiantian Fan, Xuan Wu, Liyan Wang and Yumei Li in Journal of Cancer Control.
Footnotes
Author Contributions
FYZ is the guarantors of integrity of the entire study; FYZ, MHS contributed to the study concepts study design, statistical analysis,; YDL, XW contributed to the definition of intellectual content, literature research, manuscript preparation; TTF, YML contributed to the clinical studies, data analysis, manuscript editing; LYW contributed to the data acquisition, manuscript review; All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Guangzhou Health Science and Technology Project, Project number: 20241A010073.
Ethical Statement
Data Availability Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.