
Abstract
Background and Objective
To investigate the oncologic outcomes of patients with esophageal squamous cell carcinoma (ESCC) who have achieved a pathologic complete response (pCR) of the primary tumor (ypT0) after neoadjuvant chemoradiotherapy (NCRT).
Methods
Patients with thoracic ESCC who underwent scheduled NCRT followed by surgery at our hospital between January 2010 and December 2022 were retrospectively analyzed. Only patients with ypT0 disease were enrolled in this study.
Results
A total of 118 patients were ultimately enrolled in this study. Ninety-two patients achieved pCR in the primary tumor and lymph nodes (ypT0N0), while 26 patients had residual metastatic disease in 52 lymph nodes (ypT0N+). Forty-five of the 52 lymph nodes with residual tumors were abdominal lymph nodes. Positive lymph nodes were more often observed in patients with tumors located in the lower third of the esophagus. The 1-, 3-, and 5-year overall survival (OS) rates for the entire study group were 96.5%, 79.5%, and 77.1%, and the 1-, 3-, and 5-year disease-free survival (DFS) rates were 90.5%, 76.8%, and 69.0%, respectively. According to multivariate analyses, pN classification was an independent predictor of both OS and DFS (P < 0.05), while sex and cT classification were also found to be independent prognostic factors for DFS (P < 0.05).
Conclusions
Residual nodal metastatic disease in patients with ypT0 ESCC after NCRT was more often found in the abdominal lymph nodes. pN classification was an independent predictor of both OS and DFS for ypT0 ESCC patients after NCRT.
Keywords
Introduction
For locally advanced esophageal squamous cell carcinoma (ESCC), neoadjuvant chemoradiotherapy (NCRT) plus surgery is now accepted as the standard therapy based on the CROSS study and the NEOCRTEC 5010 study.1,2 Compared with surgery alone, NCRT plus surgery can significantly improve long-term survival with acceptable toxicity for these patients.1,2
According to previous studies, 13.2% to 55.5% of patients with locally advanced ESCC achieve a pathologic complete response (pCR) in the primary tumor and lymph nodes (LNs) (ypT0N0) after NCRT.1-12 Moreover, 2.9% to 13.9% of patients achieve a pCR in the primary tumor with residual metastasis in LNs (ypT0N+) after NCRT.5-12 It is well established that patients who achieve a pCR after NCRT have significantly better survival than those who do not achieve a pCR.13,14 However, nearly 20% of patients who achieve a pCR develop recurrent disease after surgery.13-16 The oncologic outcomes of patients with ypT0 ESCC after NCRT have not been well characterized in the literature, and the impact of residual nodal disease on these patients is still controversial.9,17
In the present study, we reviewed data of 118 patients with ypT0 ESCC after NCRT in order to investigate their clinicopathologic features and oncologic outcomes.
Patients and Methods
Patients
A total of 3571 patients with esophageal carcinoma underwent esophagectomy at the Cancer Hospital of Shantou University Medical College between January 2010 and December 2022. Only the patients with thoracic ESCC who underwent scheduled NCRT followed by surgery were enrolled in this study. At last, 239 patients met the inclusion criteria and were enrolled in this study. We excluded two patients who died perioperatively and one patient with no follow-up data, leaving a total of 236 patients for analysis. Of these patients, 118 (50.0%) had a pCR of the primary tumor and were enrolled in this study. This study was approved by the Institutional Review Board of the Cancer Hospital of Shantou University Medical College on January 13, 2023 (No. 2023025). The reporting of this study conforms to STROBE guidelines. 18
Pretreatment Assessment
Pretreatment staging included barium meal imaging, cervical ultrasonography, endoscopic ultrasonography (EUS), and contrast-enhanced computed tomography (CT) of the chest and abdomen. Positron emission tomography (PET) was not routinely performed. Lymph nodes that had a maximal transverse diameter ≥1 cm on CT scan were considered to be positive. On EUS, except for the size of the lymph nodes, other characteristics such as echogenicity, border, and shape were also assessed to identify positive lymph nodes. The pretreatment clinical stages and postoperative pathologic stages were classified using the eighth edition TNM classification.
Neoadjuvant Chemoradiotherapy
Neoadjuvant radiotherapy was administered using 6 or 8 MV photons delivered by a linear accelerator. The gross tumor volume (GTV) included the primary esophageal tumor and any positive LNs, the clinical target volume (CTV) included a 3 cm margin above and below the esophageal tumor, and a radial margin of 0.5 to 1.0 cm around the gross tumor volume. The planned target volume (PTV) included the CTV plus 1 cm. The total dose was 40 to 50 Gy (median = 44 Gy) with 2.0 Gy per fraction.
The first cycle of neoadjuvant chemotherapy was administered on the first day of neoadjuvant radiotherapy, and most of the patients received 2 cycles with an interval of 3 weeks. The chemotherapy regimens included 5-fluorouracil plus cisplatin or nedaplatin (PF), docetaxel plus cisplatin or nedaplatin (TP), and vinorelbine plus cisplatin (NP). For chemotherapy, the PF regimens were given with 5-fluorouracil 750 mg/m2 intravenous (IV) for 24 h daily in Day 1 to Day 4 and cisplatin 75 mg/m2 or nedaplatin 80-100 mg/m2 IV in Day 1. The TP regimens were given with docetaxel 75 mg/m2 IV in Day 1 and cisplatin 75 mg/m2 or nedaplatin 100 mg/m2 IV in Day 1. The NP regimens were given with vinorelbine 25 mg/m2 IV in Day 1 and Day 8 and cisplatin 75 mg/m2 IV in Day 1.
Surgery
Surgery was performed at a median of 48 days (28-78 days) after the completion of NCRT. All patients underwent McKeown or minimally invasive esophagectomy with two-field lymphadenectomy. The detailed surgical procedure has been described in our previous studies. 19
Statistical Analyses
Statistical analyses were performed using SPSS 26.0 software (IBM, Armonk, New York, USA). Continuous variables between groups were compared using Student’s t test, and categorical variables between groups were compared using Pearson’s χ2 test or Fisher’s exact test. Overall survival (OS) and disease-free survival (DFS) were analyzed by the Kaplan–Meier method, and the log-rank test was used to test the differences in survival. Variables with significant differences in univariate analysis were included in multivariate Cox regression analysis to investigate independent predictors. P < 0.05 was considered to indicate statistical significance.
Results
Patient Characteristics
One hundred eighteen patients were ultimately enrolled in this study. The mean age of these patients was 57.8 ± 7.2 years, and the median age was 59 years (range, 31 to 75). The primary tumor length before treatment ranged from 2-13 cm (mean 6.1 ± 2.1 cm). The clinical T classification before treatment was cT2-3 in 73 patients (61.9%) and cT4 in 45 patients (38.1%). Sixty-five patients (55.1%) had positive lymph nodes (cN+) in the pretreatment assessment, while the other 53 patients (44.9%) had negative lymph nodes (cN0). The preoperative radiotherapy dose was 40 to 50 Gy (median = 44 Gy). Sixty-one patients (51.7%) received a total dose of 44 Gy or less, and 57 patients (48.3%) received more than 44 Gy.
In total, 2665 LNs were dissected, and 52 LNs (2.0%) had residual metastatic disease. The mean number of LNs resected was 22.6 ± 7.1, and the median number was 21 (range, 9-45). LN metastases were found in 26 patients with 1-5 positive LNs. Four patients had residual metastatic disease only in their mediastinal LNs, 18 patients had residual metastatic disease only in their abdominal LNs, and the other 4 patients had residual metastatic disease in both abdominal and mediastinal LNs. Of the 52 LNs with residual metastatic disease, 25 nodes were found along the left gastric artery, 16 nodes were found in the para-cardiac lymph nodes, 4 nodes were found in the para-esophageal lymph nodes, 4 nodes were found along the common hepatic artery, 2 nodes were found along the right recurrent laryngeal nerve, and 1 node was found along the left recurrent laryngeal nerve. Within this group, 92 patients (78.0%) had ypT0N0 disease, 21 patients (17.8%) had ypT0N1 disease, and 5 patients (4.2%) had ypT0N2 disease.
Patient Demographics.

BMI, body mass index; PF, 5-fluorouracil plus cisplatin or nedaplatin; NP, vinorelbine plus cisplatin; SD, standard error; TP, docetaxel plus cisplatin or nedaplatin.
Postoperative complications included pneumonia in 11 patients, anastomotic leakage in 6 patients, and other complications in 7 patients.
Patterns of Failure
Patterns of Failure in Patients With pT0 Esophageal Squamous Cell Carcinoma After Neoadjuvant Chemoradiotherapy.

Survival and Prognostic Factors
The last follow-up time was June 2023, and the mean follow-up duration was 54.3 months (range, 2-135 months). Thirty patients died during follow-up. The 1-, 3- and 5-year OS rates for the entire study group were 96.5%, 79.5% and 77.1%, and the 1-, 3- and 5-year DFS rates were 90.5%, 76.8% and 69.0%, respectively.
Univariate Analysis in Regard to Overall Survival and Disease-free Survival According to Clinicopathological Factors for Patients With pT0 Esophageal Squamous Cell Carcinoma After Neoadjuvant Chemoradiotherapy.

BMI, body mass index; DFS, disease-free survival; OS, overall survival; PF, 5-fluorouracil plus cisplatin or nedaplatin; NP, vinorelbine plus cisplatin; TP, docetaxel plus cisplatin or nedaplatin.

(A): Kaplan-Meier curves for overall survival of the patients with ypT0N0 and ypT0N + esophageal squamous cell carcinoma after neoadjuvant chemoradiotherapy. The 1-, 3- and 5-year overall survival rates for the ypT0N0 patients were 97.7%, 84.0% and 80.8%, compared with those of 92.3%, 63.7% and 63.7% for the ypT0N + patients. The survival difference was significant (P = 0.024). (B): Kaplan-Meier curves for disease-free survival of the patients with ypT0N0 and ypT0N + esophageal squamous cell carcinoma after neoadjuvant chemoradiotherapy. The 1-, 3- and 5-year disease-free survival rates for the ypT0N0 patients were 93.3%, 79.6% and 74.6%, compared with those of 79.9%, 66.1% and 49.7% for the ypT0N + patients. The survival difference was significant (P = 0.027).

Forest plot of clinicopathological factors on overall survival (A) and disease-free survival (B). pN classification was an independent predictor for overall survival, while gender, cT classification, and pN classification were independent predictors for disease-free survival.
Multivariate Analysis in Regard to Overall Survival and Cancer-specific Survival for Patients With pT0 Esophageal Squamous Cell Carcinoma After Neoadjuvant Chemoradiotherapy.
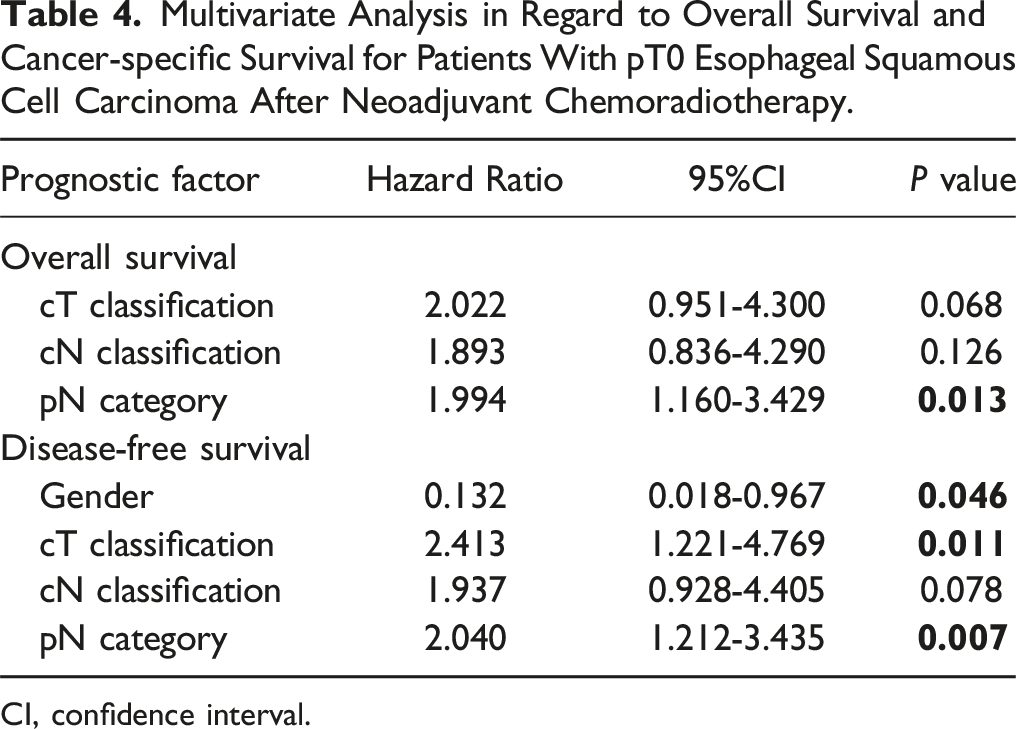
CI, confidence interval.
Discussion
The CROSS study and NEOCRTEC 5010 study established NCRT followed by surgery as the standard therapy for ESCC.1,2 According to previous studies, 13.2% to 64.4% of ESCC patients achieved a pCR in the primary tumor after NCRT.1-12 However, 2.9% to 13.9% of patients might have residual metastasis in LNs (ypT0N+) when they achieved a pCR in the primary tumor.5-12 The clinicopathological features and oncologic outcomes of these patients are still controversial. In this study, 50.0% of the patients (118/236) with ESCC who received NCRT achieved a pCR in the primary tumor, including 39.0% of patients (92/236) with ypT0N0 disease and 11.0% of patients (26/236) with ypT0N + disease. These results are similar to those of previous studies.1-12
Nine of the 26 patients (34.6%) with ypT0N + disease, of whom 8 had residual tumors in abdominal LNs, were defined as having cN0 disease in the pretreatment assessment. This indicated that the current staging methods used in this study might not have sufficiently detected positive LNs, especially abdominal LNs. Previous studies also revealed that the accuracy of EUS and CT in predicting lymph node metastasis depends on the location of the nodes.20,21 The accuracy was good for nodes located high in the thorax but poor for those located in the abdomen. 20 In this study, 45 of the 52 LNs with residual tumors were abdominal LNs, and 41 nodes were left gastric-arterial LNs and para-cardiac LNs. Most of the previous studies also showed that abdominal LNs, such as left gastric-arterial LNs and para-cardiac LNs, were the most common sites of metastasis for esophageal cancer after NCRT.9,10,22 This fact indicated that a careful abdominal LN dissection was still needed for these patients.
Tumor location was the only clinicopathological feature that was significantly different between ypT0N0 and ypT0N1 patients in this study. Nearly one-half of the ypT0 patients with tumors located in the lower third of the esophagus had residual tumors in the LNs, whereas less than 20% of the ypT0 patients with tumors located in the upper or middle third of the esophagus had residual tumors in the LNs. These results indicated that we should engage in more careful consideration when diagnosing a clinical CR for patients with tumors located in the lower third of the esophagus after NCRT. The pretreatment cN classification did not differ between ypT0N0 and ypT0N1 patients in this study. There may be several reasons for these findings. First, as mentioned above, the current staging methods may not sufficiently detect positive LNs in pretreatment examinations. Second, the patient number may not have been large enough to evaluate the difference between some clinicopathological factors, such as the cN classification.
It is well recognized that a pCR of the primary tumor is associated with better survival for esophageal cancer patients who receive NCRT.13,14,23,24 However, the impact of residual nodal disease in these patients has not been well characterized. Most previous studies reported that residual nodal disease was associated with poor prognosis in esophageal cancer patients with ypT0 disease after NCRT.7,8,22,25,26 However, another study by Cho et al. 9 revealed that residual nodal disease did not significantly influence the prognosis of ESCC patients with ypT0 disease after NCRT. Most of these previous studies were retrospective studies with both esophageal adenocarcinoma and ESCC patients, and the number of patients with ypT0N1 disease was very small (no more than 22 patients). To the best of our knowledge, we are herein reporting the largest ever single-center patient cohort of 26 patients with ypT0N1 ESCC after NCRT. In this study, residual nodal disease was found to be an independent predictor of both OS and DFS. Patients with ypT0N1 disease had significantly worse survival than patients with ypT0N0 disease. These results were similar to those of Kong et al. 8 and Wang et al. 22 Although pretreatment cN classification was found to be correlated with OS and DFS in univariate analysis, it was not an independent predictor in multivariate analysis.
Although more ypT0N + patients developed recurrent disease than ypT0N0 patients did (46.2% vs 22.8%, P = 0.019), no difference in failure patterns was observed between these two groups in this study. Both ypT0N + patients and ypT0N0 patients were more likely to have distant metastasis (76.2% of the ypT0N + patients and 66.7% of the ypT0N0 patients had distant organs as their first failure sites). This result was similar to that of Kong et al. 8 However, Blackham et al. 26 reported that ypT0N + patients were more likely to have locoregional relapse than ypT0N0 patients were.
Our study also has several limitations. First, this was a retrospective investigation, which may undermine its power. Larger prospective studies are needed to validate our findings. Second, the patient numbers in some subgroups were small, which limits the statistical power of the results. Third, the therapeutic plan for NCRT was not consistent in this study. The radiation doses ranged from 40 to 50 Gy, and the chemotherapy regimens included PF, TP, and NP. Further studies should be performed to validate our results.
Conclusions
In conclusion, residual nodal metastatic disease in patients who achieved pCR of the primary tumor after NCRT was more often found in the abdominal lymph nodes. The presence of residual nodal metastatic disease was an independent predictor of both OS and DFS for ESCC patients who achieved pCR of the primary tumor after NCRT. Larger prospective studies should be conducted to further investigate the oncologic outcome of patients with ypT0 ESCC after NCRT.
Footnotes
Author contributions
Shao-bin Chen designed the research, analyzed the data and wrote part of the paper. Xin Wang analyzed the data and wrote part of the paper. Yu-ping Chen wrote part of the paper. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Wu Jieping Medical Foundation.