
Abstract
Background
The quality of cancer care affects patient outcomes. It is therefore important to understand what factors and/or barriers shape a cancer patient’s decision about where to seek care. We sought to understand factors influencing decision-making for historically marginalized communities in a large metropolitan area with multiple options for cancer care, including a National Cancer Institute (NCI)-designated comprehensive cancer center.
Methods
We conducted semi-structured interviews with cancer patients from economically marginalized neighborhoods in Washington D.C., and with healthcare professionals who work with patients from these areas. Participants were recruited through flyers, social media posts, and word of mouth. Two researchers analyzed the data using a combination of inductive and deductive approaches supported by the ATLAS. ti software.
Results
A total of 15 interviews were conducted. Analysis revealed 3 major factors influencing where patients decide to seek care: health insurance, transportation, and prioritization of needs. Participants repeatedly identified navigating the bureaucracy of insurance enrollment and high medical costs as prohibitive to seeking care. Transportation was often mentioned in terms of convenience of use and proximity to the care center. Prioritization of needs refers to circumstances such as unstable housing, poverty, and mental illness, that some patients prioritize over seeking quality cancer care. Across these themes 2 findings arose: a discrepancy between stated and actual factors in choosing an oncologist, and the extent to which a cancer patient is able to choose their oncologist.
Conclusion
This study helps explain some of the factors that influence how cancer patients in urban settings choose an oncology center, and the barriers which prohibit access.
Aims of the Study
This study aimed to understand how cancer patients decide where to seek treatment.
Introduction
Quality of care is known to be a predictor of cancer outcomes, yet many Americans are obstructed from high-quality cancer care due to geographic, financial, cultural, and other barriers. Socioeconomic status and geographic access to care are key factors that affect the quality of cancer care a person receives. 1 1 study found greater than a ten percentage point difference in 5 year cancer survival rates between patients who live in affluent areas and patients living in lower-income areas. 2 While geographic disparities in cancer care exist between rural and urban populations, 3 significant inequities in health outcomes also exist across urban neighborhoods, despite the closer proximity to health care facilities and wider range of transportation options. 4 Cities are often highly racially and socioeconomically segregated, which contributes to racial and ethnic minority groups in the United States having higher cancer incidence and mortality rates compared with their white counterparts. 5 This difference in cancer rates can be attributed to multiple variables including greater exposure to environmental risks such as unhealthy levels of air pollutants, high rates of late diagnosis, and poorer access to healthcare.6,7
Cancer patients treated in high-quality facilities such as academic medical centers or National Cancer Institute-Designated Cancer Centers (NCI cancer centers) experience better outcomes than patients treated in community hospitals.8,9 Despite the established benefits of NCI cancer centers, approximately 85% of cancer patients are diagnosed and receive care from their community hospitals.8,10 Additionally, research suggests that certain minority groups underuse NCI cancer centers compared with their white counterparts. 11 This connection between quality of care and outcomes underscores the importance of cancer patients choosing the right location to receive treatment. Existing literature has identified geographic distance as a factor that can influence a cancer patient’s choice of where to seek treatment. Studies have found that some patients prefer to receive treatment at a lower quality, but closer treatment center even when informed about the benefits of receiving treatment at high quality treatment centers. 12 Additional research non-specific to cancer about factors that affect how 1 chooses a hospital include insurance, hospital reputation, doctor recommendations, and word of mouth affect a patient’s choice. Geographic distance is a factor that influences patient choice of care. 13
Washington D.C. (D.C) is an exemplar American city. It has a high concentration of quality cancer treatment centers, including 1 NCI cancer center and several academic hospitals. 14 D.C. also has 1 of the largest wealth gaps in the country with the top 5% of households earning 18 times the combined incomes of the bottom 20%. 15 These socioeconomic divisions occur along racial lines between the wealthier areas which are predominantly white and the underserved areas which are predominantly Black. 16 Despite the concentration of high quality cancer care in D.C., disparities exist in cancer outcomes between wealthier and poorer neighborhoods within the city. 17
D.C. is divided into 8 neighborhoods, or wards, each with approximately 75 000 residents. 18 Wards 7 and 8 are located east of the Anacostia River, physically separated from the rest of D.C., and are majority Black. 16 The median household income in wards 7 and 8 is less than half the median household income for D.C. as a whole.19,20 A recent health equity report of the city found that residents of wards 7 and 8 have the lowest life expectancy in D.C., with an almost 16 year difference from the neighborhood with the highest life expectancy. 21 According to a study measuring cancer rates in the District from 2014-2018, wards 7 and 8 had both the highest cancer incidence and cancer mortality rates. 21 Mortality rates for certain cancer types including breast cancer, colorectal cancer and prostate cancer are highest among the Black population in D.C. 22 There are no cancer centers in wards 7 or 8. 22
While research about barriers to cancer care is plentiful, to date, relatively, little has been published about the factors that contribute to a cancer patient’s decision about where to seek care and how that decision is ultimately made, particularly among socioeconomically marginalized populations. The aim of this qualitative study was to understand how cancer patients living in urban setting with a high concentration of high quality cancer centers decided where to seek treatment. This study focused on the perspectives of cancer patients and health care professionals living in Washington, D.C. about this decision-making process and the various factors contributing to the choice of oncologist. The study also sought to identify barriers that might hinder access to quality cancer care. Results of this study will help cancer advocacy and healthcare organizations in their efforts to empower patients to make informed decisions about where to seek cancer care.
Methods
This study employed a qualitative approach to investigate the experiences and perspectives of 2 distinct groups: cancer patients who reside in wards 7 and 8 of Washington D.C., and healthcare professionals engaged in treating cancer patients from these neighborhoods. Although not all participants were actively receiving treatment at the time of this study, for simplicity we use the term ‘cancer patient’ or ‘patient’ to refer to all participants who have had or currently have cancer.
A combination of purposive and snowball sampling techniques was chosen to select participants who met all inclusion criteria. The inclusion criteria were adults aged 18+, history of cancer or experience as a healthcare professional providing cancer treatment and living in wards 7 and 8 of Washington D.C., and seeking care or providing care for cancer patients from wards 7 and 8.
Recruitment efforts included the distribution of informative flyers within the regions of interest, engagement on X (formerly Twitter) and Facebook, and in-person interactions with individuals who meet the inclusion criteria.
Nineteen individuals were identified and invited to participate in the study. However, 4 participants did not meet the inclusion criteria and were thus excluded. Of the 15 study participants, 5 were cancer patients and 10 were healthcare professionals (6 clinical social workers, 2 directors at healthcare facilities, 1 patient navigator, 1 physician’s assistant). Due to resource constraints and difficulty recruiting participants that met the study inclusion criteria, recruitment was stopped when participants began giving similar answers, although it was not evident that sample saturation was fully reached.
Semi-structured interviews were conducted from July to August 2022 (Appendix A. Interview Guides). Interviews were conducted via Zoom or telephone, according to the participant’s preference. Consent forms were emailed to participants at least 24 hours before the interview, and verbal consent was sought immediately preceding the initiation of audio recording to confirm voluntary involvement. Prior to the beginning of the interview the researcher introduced herself and explained her background and the goals of the study. Interviews averaged 30-45 minutes in length. Upon completion, participants received a $50 Amazon gift card as appreciation for their contribution. Following the interviews, recordings were transcribed using transcription software, Otter. ai and edited for correction by the researcher. The researcher followed up with participants to clarify any questions about responses.
The research team consisted of 3 doctoral-level researchers trained in qualitative methods andnwith experience working in the geographic setting of the study. The researcher conducting the interviews was a white, female, undergraduate student who had experience and training in collecting and analyzingqualitative data.
The study used a combination of deductive and inductive approaches to analyze the interview data. The research team developed a preliminary codebook based on barriers to quality cancer care identified in the literature review. Using Atlas. ti, 2 researchers separately carried out 3 rounds of coding, ensuring a comprehensive and thorough examination of the data. The researchers identified emergent themes and refined the codebook incrementally with each iteration. After each coding round, the research teams engaged in collaborative discussions to discuss the codes and reconcile any discrepancies. As the analysis progressed, discernible thematic patterns emerged within the coded data. These codes were thoroughly and systematically grouped into overarching themes and subthemes, accompanied by precise definitions for each category. The final codebook consisted of 19 primary codes and 28 subcodes, providing a nuanced and comprehensive framework for interpreting the data. This rigorous analytical approach adheres to the established principles of qualitative research methodology, to ensure the study’s findings are firmly rooted in the experiences and perspectives of the participants.
The reporting of this study conforms to COREQ guidelines. 23 This study was approved by the Brigham Young University Institutional Review Board in Provo Utah (IRB# IRB2022-157) on April 15, 2022.
Results
Four main themes emerged as factors that influence a patient’s decision of where to seek care: (1) Insurance, (2) Transportation, (3) Referrals and Recommendations and (4) Social Needs (See Figure 1). Summary of results.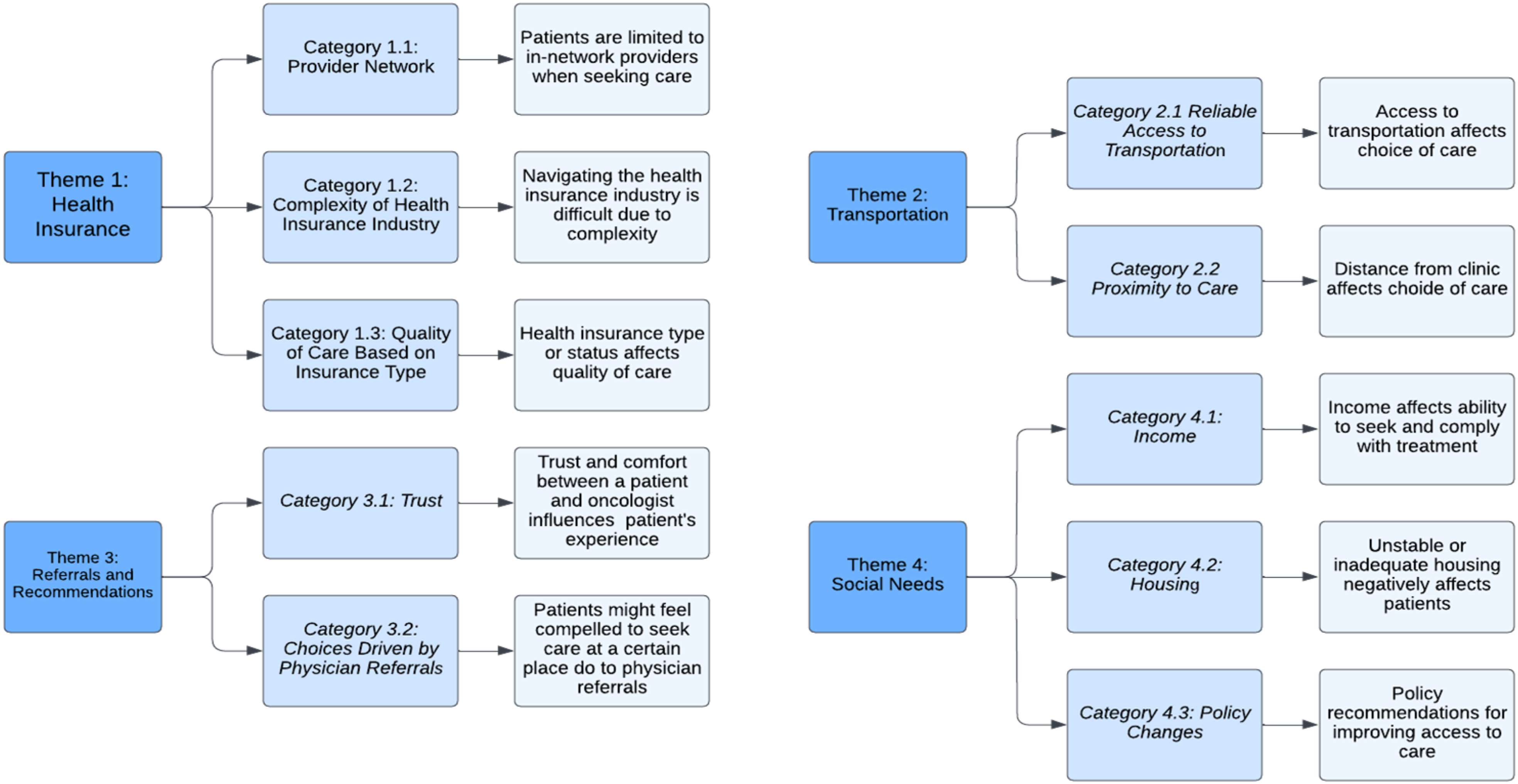
Theme 1: Health Insurance
Health insurance plays a large role in how cancer patients decide where to seek care. Most providers and patients listed it as 1 of the main factors in the decision. This theme included 4 categories: provider selection, complexity of the health insurance industry, and quality of care based on insurance type.
Category 1.1: Provider Network
Providers said that insurance is 1 of the first things that is taken into consideration when helping a patient in their decision process. If a prospective patient comes to them, but they are out-of-network, then the providers cannot work with them. According to some providers, socioeconomic status affects the extent to which insurance might control treatment provider choice, implying that provider selection presents a larger barrier to people of low socioeconomic status than to more well-off people. “Is my insurance accepted there? In my experience, that’s really what it comes down to. When you’re working with somebody that’s maybe more affluent, or, and more educated, then it really gets into more of like, where am I going to get the best care?” (Participant 11).
Patients were restricted in their choice of treatment facility by their coverage. Some patients expressed feeling unable to go where they wanted to seek care as a result of this restriction. “My decision to where to go for care was based upon who participated in my health insurance plan. I didn’t have free roam” (Participant 1). Other patients felt satisfied with the coverage options available to them.
Category 1.2: Complexity of Health Insurance Industry
Both patients and providers expressed frustration and exasperation at having to deal with the complexity of the health insurance system. Providers commented on how the complicated nature of the health insurance industry can be an additional barrier and burden to cancer patients. “You’re dealing with people who are sick, they’re fatigued, they don’t have energy to deal with making themselves dinner, let alone going through their bills and their mail and not being on the phone with insurance for hours” (Participant 4).
Providers described insurance recertification as chaotic and potentially detrimental to patients’ treatment schedules. Certain insurance plans require yearly reenrollment. Providers said that insurance enrollment can interrupt a patient’s continuity of care, which can lead to someone going without necessary treatment. “I think for patients with Medicaid, they have to recertify every year. And if they don't recertify that means their insurance gets dropped, that means we can't accept them as patients. So, I had a lot of patients who didn't recertify and so we had to stop their treatment” (Participant 8).
Patients did not comment on the ins and outs of the health insurance industry to the same extent that providers did. They talked about how insurance affected their ability to receive care. In some cases, despite being in-network, primary providers still had to press insurance companies to cover certain procedures. “Even though I was covered by him. He told me that he had to fight my insurance company” (Participant 1). Providers also mentioned having to pause treatment when physicians and insurance companies don’t agree on coverage or costs “I’ve had patients that have had to push back their visits because they don’t have insurance, or they haven’t had the clearance yet, or they had to change the drug because the insurance didn’t agree with what the doctors recommended” (Participant 11).
Category 1.3: Quality of Care Based on Insurance Type
Several providers mentioned insurance type as an indicator of treatment and care quality. They said that some people on Medicaid feel that they are treated worse in clinical settings than patients with private insurance. “I’ve had conversations with people who have Medicaid who have expressed that because they have Medicaid, they don’t feel they’re getting the best care. They feel like it’s second-rate care” (Participant 15).
This issue did not come up with patients who participated in this study. Patients did not have a uniform insurance provider; some had private insurance, some were on Medicaid or Medicare, and some had a combination of the two.
Theme 2: Transportation
Transportation to and from medical centers is important to consider when making the choice of where to seek medical care. Just providers brought transportation up as a major barrier to care while patients spoke of proximity and convenience as factors in how they decided where to seek care. This theme included 2 categories: reliable access to transportation and proximity to care.
Category 2.1 Reliable Access to Transportation
Reliable transportation to and from appointments was brought up by providers as a factor in where a person decides to seek care. Because there are no cancer treatment facilities in Ward 7 or Ward 8, residents of those wards must travel to other parts of the city to receive cancer treatment. Washington D.C. has a more comprehensive public transportation system than most cities in the United States but public transit is often not a viable option for someone in active cancer treatment. “For people who are at an active treatment, public transport is going to be tough just because it’s, they’re fatigued, and they’re sick, and they’re not feeling great” (Participant 4).
According to providers, if a patient does not have access to a car or a dependable ride or can’t afford transportation to their appointments, they might choose not to receive treatment. “Yeah I still think that [transportation] is a barrier and deciding factor because if I can't afford or it's going to stress me out to get there, I just choose not to. The headache might be if I'm speaking in patient terms, a headache of not knowing what to do and I'm trying, then I got all this stuff on my shoulders (Participant 12).
In order to ensure that patients have access to reliable transportation providers, who work as social workers, said they spend a lot of time coordinating and scheduling rides for their clients so that they can receive the care they need. “I would say at least 25% of my time was actually booking rides for patients” (Participant 8). According to providers, some medical facilities in the area are able to offer transportation assistance such as Uber vouchers to patients who are otherwise unable to get to their appointments. City services such as Metro Access were also mentioned as an alternative to public transportation.
Patients did not bring up reliable access to transportation as a big deciding factor in how they personally decided where to seek care. They said that they were able to drive themselves to and from their appointments or get rides from members of their support system. “Because I'm strong in the Lord, I was able to drive myself to my chemo and radiation. Chemo was once a week; my radiation was every day for like 30 days. I drove myself because I didn't want to share my experience and burden anybody else” (Participant 1).
Category 2.2 Proximity to Care
Patients and providers said that proximity to a cancer center can play a role in deciding to receive care there. Patients mentioned that they chose where to receive treatment at a specific hospital because of its proximity. “The main reason I settled for George Washington was just because it was closer to me and that even like scheduling the surgery, and also the aftercare that came with it would be possible, especially because I didn’t have like, so many people who could keep driving me to and from” (Participant 3).
Both patients and providers said that the lack of cancer centers in Ward 7 and Ward 8 was a burden to patients and a barrier to care. “When you think about going to chemotherapy and having to travel like 20 minutes away from your home, and then traveling back 20 minutes after treatment, and you're dealing with nausea, you know, you're dealing with just being uncomfortable. I don't think that they should have to travel outside of their neighborhood that much to receive cancer treatments'' (Participant 8). Because of the distance of some neighborhoods to cancer treatment centers, patients might forgo or delay seeking timely treatment. “People aren't going for treatment because it's not close by or easily accessible. And I think they will go sooner if it was more convenient or readily accessible, or maybe not as costly” (Participant 1).
Some participants felt that the lack of a cancer center in the neighborhood removed any real choice about where to seek care, since cancer patients must go to other parts of the city to receive care. “Yeah, I mean, I would say, to be honest with you, it's like, no decision because really, there's when you're talking specifically about wards 7 and 8, because there's not there's not any cancer centers there, I don't really feel that patients have that much of a choice” (Participant 8).
Theme 3: Referrals and Recommendations
Recommendations were often brought up as a factor in the decision-making process of where to seek care. Recommendations can be word-of-mouth suggestions from family or friends, online searches, name recognition, or official referrals from primary providers and specialists. This theme included 2 categories: trust and physician driven choice.
Category 3.1: Trust
According to patients and providers, trust between a patient and their oncologist is important in helping a patient feel comfortable and listened to. Multiple people spoke of patients choosing to go to seek care from a facility where someone they knew had a positive experience. “You know, my neighbor went to Washington Hospital Center, my niece went to Howard, whatever the case may be, and having some familiarity within their own community of a place that they know, someone they know has gone for care” (Participant 4).
Patients said they prioritized finding oncologists with whom they felt comfortable and heard. Multiple participants mentioned that comfort they felt at a certain clinic or with a certain oncologist was a factor in choosing to receive treatment at a specific place. “Yeah, and also like the team, I just wanted to feel comfortable with the oncologist I was choosing” (Participant 3).
Category 3.2: Choices Driven by Physician Referrals
Multiple participants talked about the role primary providers and specialists play in where a patient ultimately receives treatment. Referrals can be necessary to receive treatment. Because of this, a physician can directly influence where someone is treated even if the patient is the 1 who makes the choice to get care there. “They usually go where they’re told to go. So the whole concept of choice in and of itself is not always a thing. It’s like you go where you’re recommended to go. And that’s not just unique for ward 7 and 8. Sometimes people have never really entered the healthcare world until they get cancer. And then you’re just going where you’re told to go”’ (Participant 11).
Patients and providers cited referrals as a primary way people find themselves receiving treatment at a given facility. A referral system can help patients meet with specialists and receive treatment, but multiple participants mentioned that it can also take autonomy away from the patient. “Oncologists are chosen, they're not chosen by the patient. I'll put it like that. I don't think so. I think if you asked twenty other people in your survey, how it was their oncologist, it isn’t like they went through, they all looked at the record and so forth, or something. Somebody told him “look go see so and so”’ (Participant 7).
After being referred to a specialist or oncologist, patients may not feel in a position to request a different doctor. Both patients and providers mentioned the fear surrounding a cancer diagnosis and the imbalance of power between a doctor and her patient. These factors can contribute to a patient receiving care from someone they did not choose and would rather not have. “But do they kind of acquiesce to what they have? Most likely, yes. Because the diagnosis, it's scary. I think that a lot of general healthcare doesn't approach it in a way to tell you that it's your choice. So generally, they will just follow, they will just follow suit, unless it's egregious. And sometimes by the time it gets to a space that's egregious, it's hard to advocate for yourself, if folks were advocating for yourselves, the healthcare system would have to hold itself accountable. But we are in decades of discrimination, decades of oppression...” (Participant 14).
Theme 4: Social Needs
Social needs were often brought up throughout interviews as additional barriers to care, and although they do not directly address the question of how cancer patients decide where to seek care, they are important in understanding access to care. Both patients and providers talked about external factors that might affect a person’s access to care or willingness to seek out treatment. This theme included 3 categories: financial resources, housing, and policy changes.
Category 4.1: Income
Financial resources were brought up often by providers when discussing barriers to care. According to providers, sometimes patients are in economic situations that make it very difficult to prioritize personal health. This might delay someone’s choice to seek care or their ability to receive continuous care. “I can’t have this treatment. I need to go to work because my kids got to eat. I need to pay this light bill, I need to have a roof over my head. I have no other money coming in if I don’t work. So a lot of patients go through that. Like, well, maybe I just, I just have to roll the dice” (Participant 12).
Category 4.2: Housing
Patients are not always able to work while they are receiving treatment, which can make paying rent and other bills challenging. Participants said that the lack of affordable housing options in the area can make it really difficult for patients with cancer to find safe and reliable housing. “I mean, it’s just the cost of living as you know in this area is just so expensive. And a lot of our patients are not able to work because of their medical issues. And they can’t, you know, afford to pay normal rent. So they look to us to help refer them to more affordable housing, and the options are so limited there’s just not enough more affordable housing options” (Participant 13).
According to participants, the lack of affordable housing options in the area coupled with the possibility of losing steady housing might deter or delay cancer patients from seeking treatment. “If I don't have a great housing situation, and I get diagnosed with some sort of chronic illness, I might only address it once it's right in front of me. Maybe I've had something growing and now it's really a problem and I have to address it. I think that if you have a lot more going on in your life that causes stressors, and that are barriers to focusing on your personal wellbeing, it's not going to be top priority” (Participant 11).
Category 4.3: Policy Changes
Patients and providers were asked about what issues they would bring to the attention of policymakers if they had the choice. Both groups talked about providing more services to people, specifically residents of wards 7 and 8. “It starts with focus groups, it starts with providing the basic human and health needs for folks in wards 7 and 8, you know, like, we deserve, we deserve grocery stores. We deserve more than just fast-food restaurants at every single corner. You know, we deserve more than cutting a ribbon of a new Starbucks, when I don’t have a healthcare center. I don’t have a hospital” (Participant 14).
Discussion
This study contributes knowledge to a small body of research surrounding the decision-making process of a cancer patient about where to seek treatment, and it supports existing research about factors that contribute to that choice. Our results identified 3 factors influencing a cancer patient’s decision about where to seek care: insurance type and status, access to reliable transportation, and recommendations or referrals from doctors or community members. In addition to these factors, stable housing and access to financial resources were identified as barriers to care.
Our findings highlighted a discrepancy between how patients said they actually chose their oncologist and what patients said was most important to them in finding an oncologist. While patients reported selecting their oncologist based primarily on insurance, recommendations, and proximity, they said the factors that were most important to them in finding an oncologist were the education and experience of the oncologist, their comfort with the medical center and oncologist, and how they were treated by doctors and medical staff. This finding aligns with those from other studies that have found high levels of patient-provider trust among cancer patients to reduce patient fear and encourage more communication. 18
This insight that patients are making decisions about where to seek care based on practical considerations rather than what they say they value the most indicates that patient choice is quite limited when deciding where to seek care. In other words, a patient might prefer certain characteristics in an oncologist, but are compelled to prioritize external factors such as provider network or proximity.
Interestingly, the results of this study did not yield as much information about the specific cancer centers in the city as the authors expected. Instead, the results pointed to a larger question of the extent to which a patient has a choice when deciding where to seek care. Both providers and patients talked about referrals from physicians as one of the most important driving factors in where people seek care. Due to the complexity of the healthcare system in the U.S. and the referral system, some patients did not feel the choice about where to receive cancer treatment was theirs to make because it had effectively been made for them by their referring physician.
There are important health equity implications when considering treatment options for marginalized patients, such as those in this study, who may have less facilitating in navigating the complexities of the US healthcare system in the face of a major diagnosis. To help ensure all patients have access to quality care, shared decision-making is essential so that cancer patients know all options available to them when seeking care.
Insurance type and status were mentioned not only as influencing factors in where to seek care, but also as indicators of quality of care. According to providers, patients on public insurance, such as Medicaid, might feel that they receive lower quality of care because of their insurance type. 24 Research suggests that uninsured patients and publicly insured patients are more likely to experience unfair treatment in a healthcare setting than patients who are privately insured. 25 Insurance type or status should not dictate quality of care. Patients should reliably receive the same treatment regardless of insurance.
This study also surfaced themes related to racial inequities in healthcare since it focused on 2 neighborhoods in D.C. that are predominantly Black and are geographically isolated from the rest of the city by the Anacostia River. 11 Due to decades of racism and racist redlining policies, wards 7 and 8 have long been underserved and lack many of the resources that are available to residents in other parts of the city such as working grocery stores, hospitals, or safe sidewalks.26-30 This further illustrates the point that health disparities due to lack of geographic access exist in urban along rural settings.
While this study focused on a specific geographic region, it has important implications for cancer care in other regions as well. To our knowledge, there is a scarcity of existing literature about a cancer patient’s decision-making process when seeking treatment. Our findings provide relevant insights into the experience of cancer patients trying to determine next steps in their treatment process.
Limitations
While this study is not generalizable to areas outside of the targeted neighborhoods in Washington, D.C., issues around racial segregation and health disparities are likely to exist in other urban areas in the United States, and this study can offer insights into how cancer patients from economically marginalized neighborhoods in those cities decide where to seek care. This paper achieved its aim by helping better understand how cancer patients choose where to seek care, but the small sample size is a limitation that makes its findings less conclusive and non-generalizable. Additionally, participant feedback was not sought after the data was finalized. Due to the qualitative approach and low number of study participants, a larger study using different methods would be necessary to confirm our findings. Selection bias is another limitation since the recruitment method employed resulted in many healthcare providers holding similar positions in healthcare facilities across the city. It is valuable to understand their perspectives, but a wider range of professional experiences and opinions from healthcare workers would meaningfully contribute to the findings of this study.
Conclusion
The findings in this study indicate that insurance, transportation, and recommendations affect how a cancer patient decides where to seek care. Based on our results, several recommendations can be made to improve a cancer patient’s experience when seeking and receiving treatment. Building and improving systems to increase health literacy has been found to positively affect a patient’s level of self-efficacy. Investing in these systems will enable cancer patients to feel more confident about what next steps are available to them. Additionally, cultural competence has been linked to higher rates of patient satisfaction and a reduction in health disparities among diverse populations. An increased focus on cultural competency could improve a patient’s treatment experience and health outcomes.
On a structural level, recommendations from this study include higher investment into health and access to healthcare in wards 7 and 8 in Washington D.C. This may include building a cancer center or out-patient cancer treatment facility so that residents of wards 7 and 8 are not compelled to travel as far to access care. Additionally, policymakers should understand and consider cancer patients’ preferences for treatment when considering making changes that affect the city’s healthcare system.
Results from this study will be distributed back to the individuals and organizations who contributed to its completion. In this way, the authors hope to give back and to disseminate the information found in this study to as many people as possible.
Footnotes
Acknowledgments
The authors would like to thank the following individuals for their valuable contribution to this paper: Dr Alejandra De Mendoza, Altonia Garret, Dr Angela Johnson, Dr Carla Williams, Carole O'Toole, Cheryl Shaw, Dr Chiranjeev Dash, Christina Marea, Dale Mooney, Elizabeth Franklin, Reverend George Gilbert Jr, Hannah Arem, Irwin Royster, Jennifer Bires, Jennifer Meldau, Kimberly Parekh, Kelly Hendershot, Kiersten Gallagher, Lauren Broschak, Dr Mandi Pratt-Chapman, Dr Maranda C. Ward, Phyllis Givens, Dr Randi Williams, Dr Regina Hampton, Stephanie Stern, Tesha Coleman, Thelma D. Jones, Founder, Thelma D. Jones Breast Cancer Fund, Tommy Zarembka, Dr Wayne Lawrence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Brigham Young University Simmons Center for Cancer Research.
Ethical Statement
Institutional Review Board
This study was approved by the Brigham Young University Institutional Review Board in Provo Utah (IRB# IRB2022-157) on April 15, 2022. Participants provided written consent prior to the interview.