
Abstract
Objectives
Breast cancer is leading the cancer incidence and mortality ranks worldwide. Currently, breast cancer represents 30.1% of all cancers occurring in women in Congo. In sub-Saharan Africa, breast cancer is diagnosed delayed in 70% of cases. The purpose of this work is to study the epidemiological aspects of patients with late diagnosis of breast cancer at the Brazzaville University Hospital, Congo.
Methods
We carried out a cross-sectional analytic study in the medical oncology service of the University Hospital of Brazzaville. We used systematic, exhaustive sampling. Logistic regression was used for data analysis, and P values ≤5% were considered significant.
Results
Data for 182 patients were collected. Delay in diagnosis represented 91.21% of cases. Delay in diagnosis was significantly associated with lack of finance (P = 0.011) and with breast cancer stages greater than 2 (P < 0.001), but the proximity to the center was suggestive. Multivariate analysis revealed an association between diagnostic delay and proximity to the center (P = 0.025) as well as with breast cancer stages greater than 2 (P < 0.001).
Conclusion
The delay in breast cancer diagnosis widely discussed in the literature remains relevant in Congo. Routine screening, the construction of a cancer center and its optimal equipment, and the subsidy of care are all critical factors for battling delayed breast cancer diagnosis in Congo.
Introduction
Worldwide, breast cancer accounts for 16% of all female cancers and is the leading cause of cancer incidence and mortality. 1 World Health Organization (WHO) estimates that approximately 2.1 million new cases and 627,000 deaths occurred in 2018 worldwide. Although incidence is increasing in most parts of the world, there are huge inequalities between developed and developing countries. The higher incidence rates in the West contrast with high mortality, more than two-thirds of which occurs in poor countries due to lack of early detection and access to treatment. 1
In Africa, the burden of breast cancer is estimated at 24.5 cases per 100,000 inhabitants with a mortality rate of 12 per 100,000 inhabitants, compared with 93 per 100,000 and 15 per 100,000 respectively in the United States.2,3 The Congo is not to be outdone, as this scourge also ranks first among women’s cancers before cervical cancer. 4 Breast cancer represented 30.1% of all female cancers with 110 cases diagnosed in 2017. 4 Currently, medical progress allows for early or even sub-clinical diagnosis and a better prognosis in the more equipped and organized countries. 1 Congo has a single cancer care department within the University Hospital, which is attached to the Faculty of Health Sciences for the training of cancer specialists from a variety of backgrounds. Taking into account the various aspects of cancer care (awareness-raising, treatment, etc.) should reduce the incidence of cancer in the Congo. Despite these achievements, 70% of breast cancers in sub-Saharan Africa are still diagnosed late, causing a real problem of adequate management.3,5 This results in enormous direct, indirect and opportunity costs that are difficult to bear by the population. It is now urgent to develop effective and accessible approaches for early detection, diagnosis and treatment of breast cancer in developing countries in order to better fight against this gangrene. The objective of the study is to study the epidemiological characteristics of patients with delayed diagnosis of breast cancer at the University Hospital of Brazzaville.
Methods
Design and Population Study
This is a cross-sectional analytical study, carried out in the medical oncology department of the University Hospital of Brazzaville, which is the only one of its kind in Congo. It took place from 1 October to 31 December 2020.
The target population was breast cancer patients in the city of Brazzaville during the study period. The source population was all patients with breast cancer who consulted the medical oncology department of the Brazzaville University Hospital during the study period. Exhaustive sampling was used.
All patients with histologically confirmed breast cancer with a usable record were included. Histology was performed either on biopsy specimens or on surgical specimens for cancers surgically removed. Not including all cases of histologically confirmed breast malignancy with missing variables.
As main variable we have the delayed diagnosis which includes locally advanced breast tumors (greater than 5 cm in size with or without lymph node extension; and/or stage T3-T4); and/or metastasized at the time of diagnosis. Early stage includes American Joint Committee on Cancer (AJCC) stages I and II. Advanced stage includes AJCC stages III and IV. The predictors were the socio-demographic and clinical characteristics of the patients. The reporting of this study conforms to the STROBE guidelines. 6
Data Collection Tools
The tool used is a pre-established and pre-tested questionnaire. The questionnaire contains patients ‘socio-demographic and economic characteristics, clinical and Para clinical data, the main reasons for the delay in diagnosis cited by patients, and patients’ behaviour at the first signs of the disease. The questionnaire was validated by the Scientific Committee of the Inter-State Centre for Higher Education in Public Health in Central Africa (CIESPAC).The questionnaire was field-tested with 100 patients with cervical cancer at the same Centre. All the patients had the same socio-demographic characteristics. The data was collected by direct interview of the patients and also by using a document review.
Data Analysis
For the qualitative variables we used numbers and frequencies. Means with standard deviation were calculated for the quantitative variables. A simple logistic regression was used to establish the relationship between diagnostic delay and clinical characteristics. The odds ratios with their 95% confidence intervals for P < 0.05 were obtained. Using multiple logistic regression, the relationship between diagnostic delay and selected patient characteristics was established. For this purpose, Wald Chi 2 and odds ratios with their 95% confidence intervals for P < 0.05 were used. In order to adjust for the main confounders multiple logistic regression was used, which went through a stepwise elimination for P < 0.20 to predict this relationship.
Ethical Considerations
The study received the approval of the ethics committee and an authorization from the Direction of CIESPAC. Ethical clearance to conduct the study was sought from the Ethical Review Committee of the CIESPAC with reference number
Results
Patient Characteristics
Characteristics of Patients.

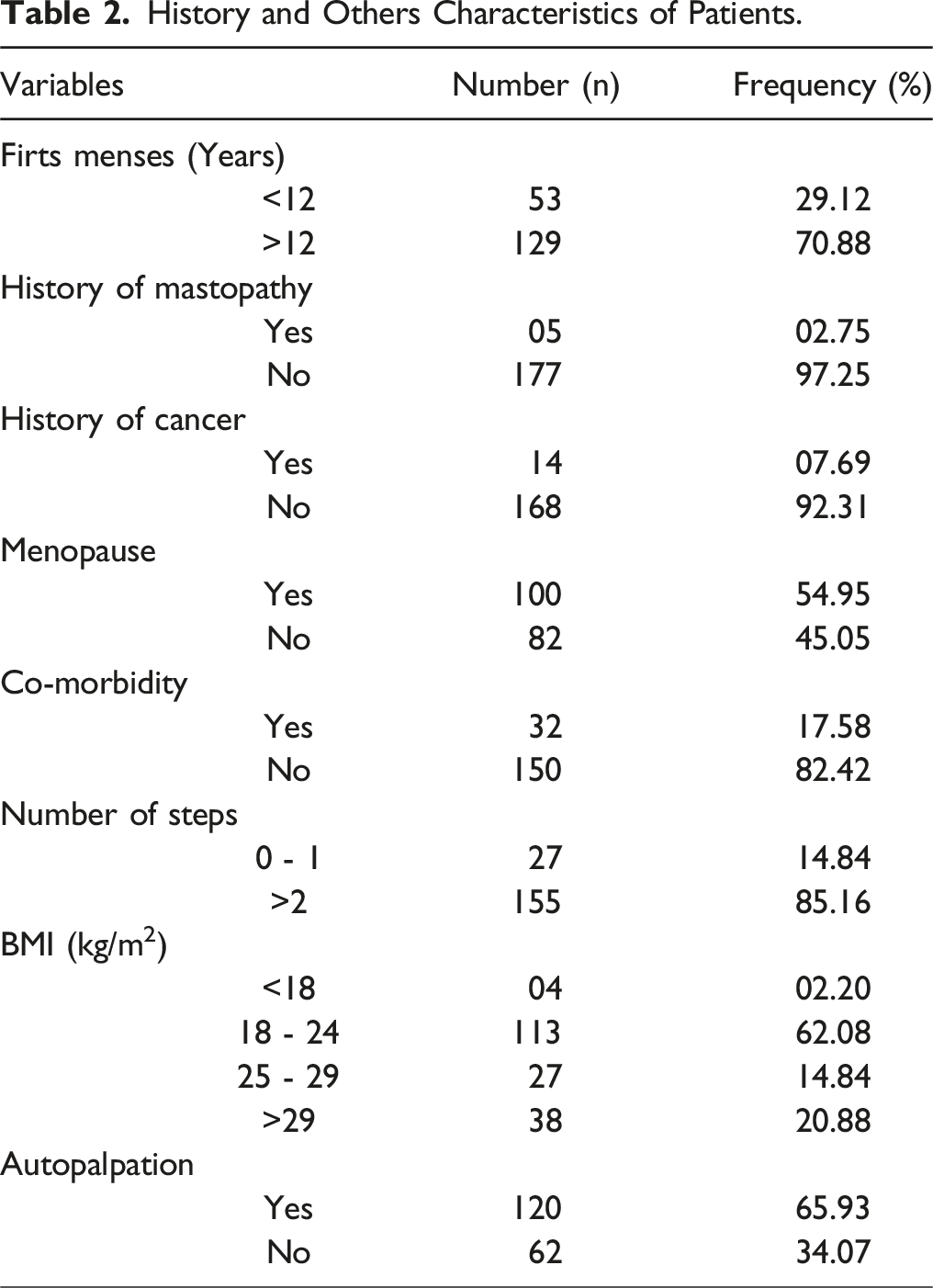
History and Others Characteristics of Patients.
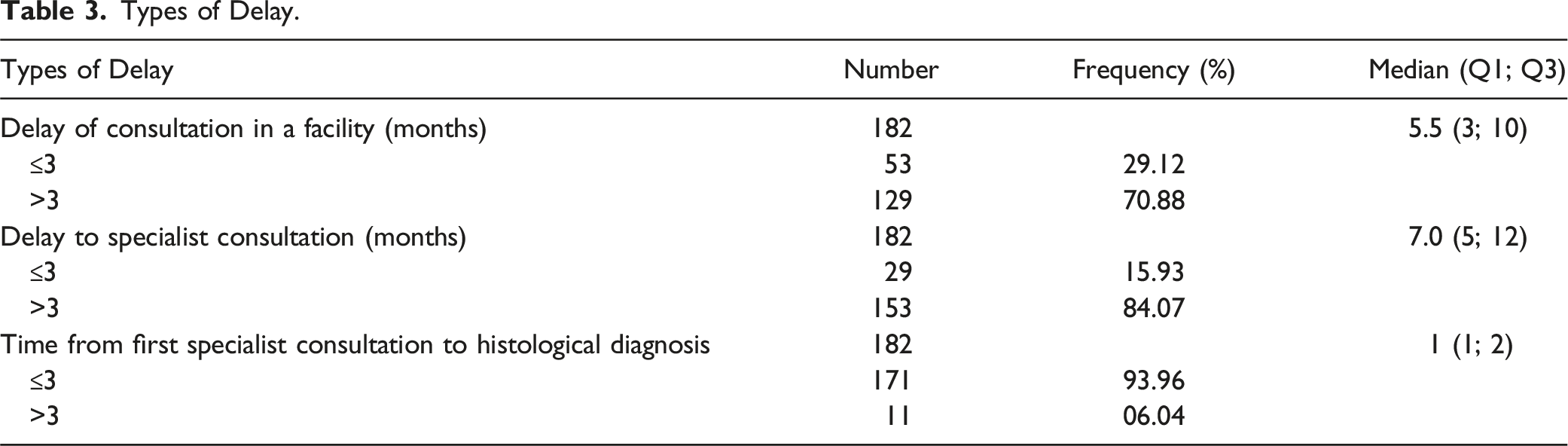
Types of Delay.
Patient-Reported Reasons for Delayed Diagnosis
Of those cancer cases, 166 (91.21%) were seen late by an oncologist. The delay was patient-related in 75.3% (125/166) of cases, health system-related in 21.08% (35/166) of cases and both in 3.61% (6/166) of cases. Figure 1 shows the main reasons given by patients for the delay in diagnosis. Patients’ reported reasons for diagnostic delay.
Factors Associated with Delayed Diagnosis
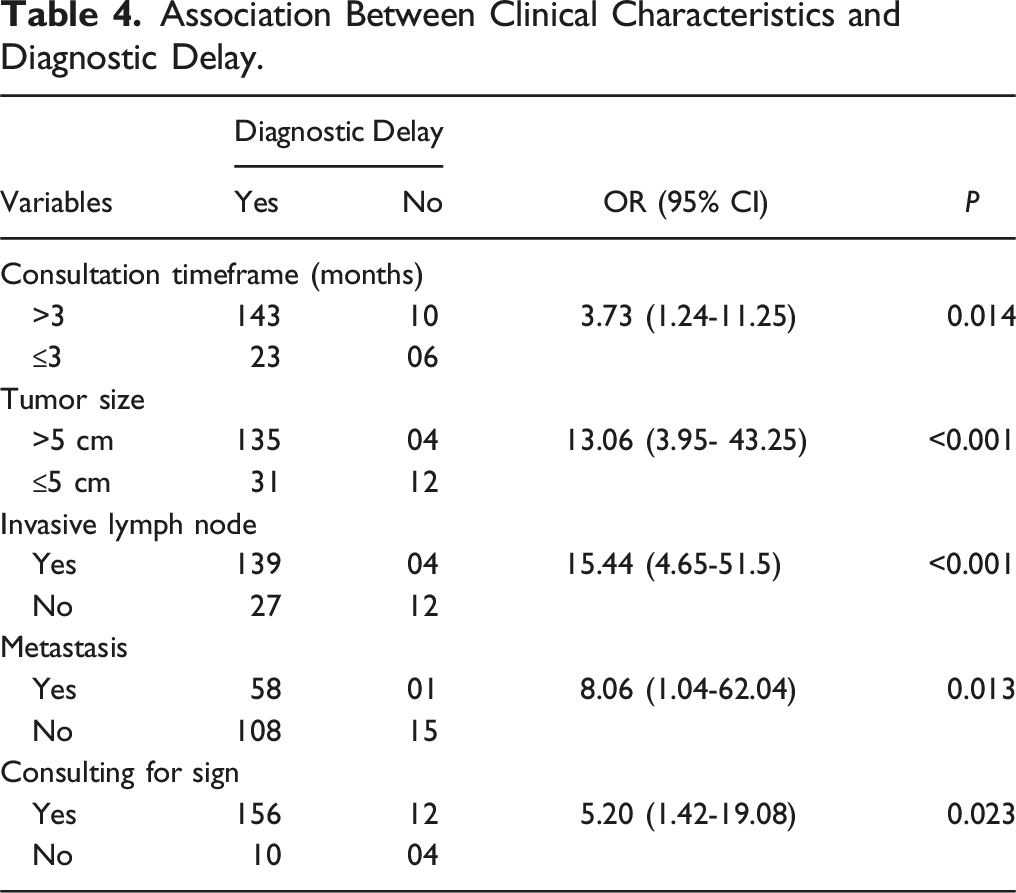
Association Between Clinical Characteristics and Diagnostic Delay.
Factors Associated With Diagnostic Delay.

aOdds ratio adjusted for comorbidity, income and marital status.
Discussion
Study Limitations and Strengths
The present study took place in the only university hospital in the country. Although it is the largest centre for cancer management, it remains accessible to only a minority. The cross-sectional nature of the study and the lack of histological evidence in some cases may have influenced the quality of our results, thus posing a potential problem of selection and information bias. Ignorance, lack of funding, socio-cultural factors and inaccessibility to qualified health services and staff are all factors blamed for the delay in diagnosing breast cancer. Taking all these factors into account could reduce the heavy burden of breast cancer in the Congolese population.
Baseline Characteristics
We collected 182 patients with a mean age of 50 years. Our results corroborate those reported by some authors (B1-3) but are higher than those found by others4-8 who showed that the age ranged between 45 and 48.3 years. However, the average age is still lower than that reported by ARNDT 7 in Germany, which was 57.3 years. Although relatively high, this average age can be explained by an improvement in health care provision, environment and lifestyle with a trend towards Western lifestyles. All this has led to an increase in life expectancy. However, Da et al. 8 reported in the literature review that breast cancer occurs 10 years earlier in sub-Saharan Africa than the average age in Western countries.
Urban patients represented 81.86% of our study population. This proportion of urban patients varies between 65% and 71% reported in some studies.9-11 Breast cancer is more likely to be diagnosed at early stages in urban patients than in rural ones and, therefore, more treatable. Indeed, the disease is thought to be more prevalent in urban than in rural communities due to the adoption of more westernized lifestyles (particularly reproductive patterns characterized by later age at first full-term pregnancy, lower parity, duration of breastfeeding less than 6 months, and increased post-menopausal weight) by urban dwellers although some researchers have explained that this difference may be due to misreporting of residence by women. 12
More than half of our population was unemployed (57.79%). This unemployment rate is higher than those found by some authors,10,13,14 which were 44.5%, 26.9% and 26.8% respectively. This can be explained by a lack of job creation and self-employment initiatives, or by a lack of skills or qualifications adapted to the current need. Thus, a sedentary lifestyle is considered to be a factor favoring the occurrence of breast cancer, hence the interest in encouraging the regular practice of sport and personal initiatives for job creation.
Nearly 30% of women have less than a secondary education. Some authors in Ethiopia and India 10,11 have made the same finding, but this is lower than the data reported by others.9,15,16 This suggests a relatively high literacy rate due to the geographical and financial accessibility of educational facilities in Congo, but is not synonymous with employability skills, as many of this population have not completed secondary school.
Delayed referral was found to be associated with patient, health system and provider mediated factors. Patient-mediated factors mainly included low education, ignorance of warning signs and lack of awareness of breast cancer, use of alternative care, financial problems, fear (of the disease and/or its effects, partner abandonment), shyness, fatalism and denial. Those mediated by the health care system and provider were distance to the nearest health care centre, type of first health care provider visited, number of providers visited before diagnosis, type of navigation followed before reaching the diagnostic centre, misdiagnosis, bad advice or fake insurance. This tendency can be traced back to low health awareness among patients, poor information campaigns and lack of mammography or other screening programmes for early detection of breast cancer, or inability of patients to pay for health care services due to lack of universal health insurance. 13 A high number of referrals lengthen the patient’s journey through the health system, resulting in a more advanced tumor stage at diagnosis.
The diagnosis delay was 92.21% in our population. This finding corroborates well the data of some authors5,11,13,17–21 on the high proportion of advanced breast cancer cases at diagnosis with values ranging from 60.9% to 96.3%, while other authors 22 reported lower data, 17.14%. This is explained by the lack of routine population-based screening programmes, poor awareness of symptoms, high cost and limited access to diagnostic services. Our results showed a significant association between diagnosis at an advanced stage and delay in consultation, tumor size, lymph node involvement and occurrence of metastasis. Some authors 13 have also reported that delay in diagnosis was associated with larger tumor size, positive lymph nodes, a high incidence of late clinical stages and metastatic disease. The same is true for other authors from Morocco, 12 Egypt 18 and Germany 7 for advanced stage at diagnosis and delayed consultation. In our context, this can be explained by the pathophysiology of the cancer itself. Once established, no spontaneous remission is possible without adequate specific treatment.
Many factors contributing to the delay in diagnosis were mentioned by the patients, but most of them did not show a significant association. Lack of financial means was significantly associated with the occurrence of delay. This result is in line with most African studies5,9,13,17,23 but contrary to the Pakistani finding 24 which reported that a significant increase in delay was associated with higher family income. In contrast, MOUSA 18 found no association between a delay in presentation of more than 3 months in Egypt and a woman’s socioeconomic characteristics or symptom type before or after adjustment for potential confounders. Education is a key factor in socioeconomic status, influencing lifestyles, behavioral patterns, reproductive factors such as parity and even stage of presentation. Socioeconomic status is correlated with late diagnosis of breast cancer.12,25 Low education and low socioeconomic status lead to poor compliance with screening by the population, especially mammography, the cost of which remains high for many of our populations. 17
After adjustment for comorbidity, income and marital status on bivariate analysis, the number of steps greater than two and the distance to the health centre are associated with delayed diagnosis with respectively P < 0.001 and P = 0.025. This finding confirms the data from Morocco 19 and the systemic review 11 concerning Rwanda and Cameroon on the implication of the number of steps (>2) on late diagnosis. This can be explained by the fact that patients with delayed diagnosis who resided close to the screening centres tended to go to alternative medicine or non-accredited practices for their care. This led to misdiagnosis and/or inadequate care, increasing their diagnostic delay and the stage of the disease. This behavior was motivated by negative information and the fatal outcome of some patients followed at the Brazzaville university hospital or the military hospital, which came to their understanding. Others preferred to go to a neighboring country where there is no centre and no approved personnel for the treatment of cancer, where they were treated indiscriminately. This indicates a continuous ignorance and fear of breast cancer among the Brazzavillian population, hence the notion of “breast cancer haunting”. Patients have linked their cancer to supernatural forces, hence their adherence to alternative treatments, and have presented themselves to hospitals only when their symptoms worsened. This finding is consistent with data reported by some authors.9,10,17,19,24 The association of breast cancer with supernatural and ancestral causes produces guilt and lack of control over the disease for most patients in sub-Saharan Africa. 8 Patients believe that cancer is a punishment from their ancestors in response to a wrong they have inflicted on them and that no living person can fight the dead. The ancestors are said to have the power to protect, heal and kill, and a good relationship with the ancestors is said to be the key to good health.
Conclusion
Delay in diagnosis is characterized by a long delay in consultation, a large tumor size, and a distant location, which is responsible for a more complex, expensive treatment and a poor prognosis. Ignorance, lack of funding, socio-cultural factors as well as inaccessibility to a service and qualified health personnel are all factors incriminated in the diagnostic delay of breast cancers. Mammography screening is often advocated as the best intervention to improve the early diagnosis of breast cancer, but despite its low accessibility, it remains insufficient in our context. It will only reduce specific mortality if women with suspicious lesions at screening have access to diagnosis and appropriate treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.