
Abstract
Objective
The objective of our study is to explore Nepali women’s beliefs about access to mammography screening, and motivations to get screened or not. This work was intended to be hypothesis generating for subsequent quantitative analysis and to inform policy and decision-making to improve access.
Methods
We conducted structured qualitative interviews among nine Nepali women in the Northeast of the United States receiving care at a local community health center and among nine white women receiving mammography care at a large academic medical center in the Northeast. We analyzed the transcripts using a mixed deductive (content analysis) and inductive (grounded theory) approach. Deductive codes were generated from the Health Belief Model which states that a person’s belief in the real threat of a disease with their belief in the effectiveness of the recommended health service or behavior or action will predict the likelihood the person will adopt the behavior. We compared and contrasted qualitative results from both groups.
Results
We found that eligible Nepali women who had not received mammography screening had no knowledge of its availability and its importance. Primary care physicians emerged as a critical link in addressing this disparity: trust was found to be high among Nepali women with their established primary care provider.
Conclusion
The findings of this study suggest that the role of primary care practitioners in conversations around the importance and eligibility for mammography screening is of critical importance, especially for underserved groups with limited health knowledge of screening opportunities and potential health benefits. Follow-up research should focus on primary care practices.
Plain Language Summary
In this study, we interviewed Nepali women in a small, rural state in in the Northeast of the United States who are eligible for breast cancer screening yet do not seek it to better understand their motivations f. We also interviewed women who did get mammography screening to understand their motivations. We found that eligible Nepali women who had not received mammography screening had no knowledge of its availability and its importance. Primary care physicians emerged as a critical link in addressing this disparity: trust was found to be high among Nepali women with their established primary care provider. The findings of this study suggest that the role of primary care practitioners in conversations around the importance and eligibility for mammography screening is of critical importance.
Keywords
Introduction
Breast cancer is one of the leading causes of death among women in the United States (US). The American Cancer Society estimated that 310,720 new cases of invasive breast cancer, 56,500 new cases of ductal carcinoma in situ (DCIS) and 42,250 deaths from breast cancer occurred among women in the United States in 2023. 1 Overall survival advantages in breast cancer depend on multifactorial aspects, including primary breast cancer prevention strategies, such as physical activity, smoking cessation, healthy diet, and maintaining a normal BMI as well as secondary prevention, chiefly through screening mammography. The Center for Disease and Control (CDC) emphasizes that mammography screening is the only proven effective breast cancer screening method 2 and it’s the most sensitive and specific test that can be performed for early detection of breast cancer. 3 From a seven US population-based screening programs on about 463,372 participants, the result showed that mammography sensitivity and specificity was at 75 and 92.4%, respectively. 4
Several randomized trials as well as population-based screening evaluations have indicated that early detection of breast cancer through screening mammography improves treatment options,5-8 the likelihood of successful treatment, and improved survival. Breast cancer screening save lives: early detection of breast cancer increases the chances of survival of an afflicted individual by up to 98% 9 ; when breast cancer is not detected early, the odds of survival decreases 25%. 10 In a recent study, survival rate for all women who attended five screening mammograms was found to be 80%, while those who never participated in mammography screening had a a survival rate between 59.1% and 77.6%. 11
Screening mammography is one of the free preventive measures available under the Affordable Care Act (ACA). Unfortunately, not everyone is aware of this and not everyone is making use of this unique opportunity to get screening mammography done at not out of pocket cost to them. Early and timely detection of breast cancer reduces the burden on the healthcare systems. Immigrant and minority women are often diagnosed with advanced stage breast cancer disease than other group of women, and lower attendance in mammography screening services is a major contributory factor. 10 Unlike other countries, screening in the United States occurs is majorly opportunistic, meaning the recommendation for screening is from people who present themselves at the healthcare facilities or per patient request. 12 Therefore, if eligible immigrants and minority women have no access to healthcare facility where they can be referred, or have no knowledge about mammography screening, they may lose out on the benefit it provides. Sociodemographic gradient has been associated with mammography participation in many countries; income, level of education, access to health insurance, use of health services, ethnic minorities have negatively impacted breast cancer screening participation rates. 12 Women who are less educated, women in lower occupational classes or with no occupation are less likely to participate in mammography and produces inequalities, due to socioeconomic status (SES). 13 Universal access to mammography can potentially obliterate all racial and sociodemographic lines in breast cancer screening. 12
We conducted a study at an academic medical center in the Northeast where white women seek screening mammography more than the non-white population. We know this by comparing Census data with cancer registry data in the state and from the literature.14-17 While racial disparity gaps among mammography seekers have been reported in the literature for other parts of the United States, there has been limited research in rural states. This study is carried out with the aim of gathering first-hand information from eligible women about their access, motivation, and/or barriers to seeking mammography screening. The knowledge gathered from this study is intended to inform quantitative research focused on designing interventions that will bridge the racial divide among mammography seekers in the state of Vermont.
The objective of our study is to explore Nepali women’s beliefs about access to mammography screening, and motivations to get screened or not. This study was hypothesis generating for follow-up quantitative analysis and to inform policy and decision-making to improve access. We started with the Nepalese population in the area because they rank highest among non-white women population regularly visiting the academic medical center.
Methods
This was a prospective study using qualitative research method to explore perceptions related to access to mammography screening. Interviews were conducted in-person (in compliance with social distancing and health and safety guidelines) between April 27, 2021, and June 29, 2021, at the medical center and the Community Health Centers by well-trained researchers. Verbal informed consent was obtained from the study participant before the interview. The reporting of this study conforms to COREQ guidelines,. 18 This was a small pilot study with the intention to be hypothesis generating. Therefore, no sample size calculation was conducted as the aim was not to deduct statistically significant differences.
We interviewed women on regular visit to a local Health Center as well as women attending the academic medical center during their mammography visit, to compare motivations of women who get screened and those who do not. A convenience sample of eighteen women were recruited by email and phone calls and patient’s primary care providers. Nine Nepalese participants were recruited from the community health center and nine white women receiving mammography were recruited from the medical center. Participants were compensated for their time with a $15 grocery gift card.
For this study, we collected data through face-to-face individual, in-depth, and semi-structured interviews conducted in English. For the Nepalese population, interpretative services were provided during the interview sessions. No discrepancies between translations were identified. There were no repeat interviews. Each participant was interviewed in a session lasting approximately 20-60 min. All interviews were recorded using a voice recorder with the consent of the interviewee and transcribed via a local transcription service.
Data Analysis
Interpretative Phenomenological Analysis (IPA) was undertaken with the assistance of NVivo 12 19 for coding and data management. The six-step IPA process includes: looking for themes; looking for connections; producing a table of themes; continuing analysis with next case; creating a master list of themes; and writing up findings. Deductive and inductive codes were employed by two separate coders, comparing results. We analyzed coded interview transcripts using a mixed deductive (content analysis) and inductive (grounded theory) approach. Deductive codes were generated from the Health Belief Model.20-22 Units of meaning were first drawn from the transcripts; codes were then generated inductively and were assigned to different hierarchical categories based on their similarities to each other. This process was continued until data saturation was achieved so that no other themes could be drawn. Finally, participant demographics were analyzed quantitatively by comparing counts, percentages, and standard deviations by the two groups (Nepalese vs comparison group) using Stata 17 23 and Redcap. 24
Examples of Health Belief Model Concepts, as Applied to Mammography Screening.

Results
Demographics of Interviewed Community Members.

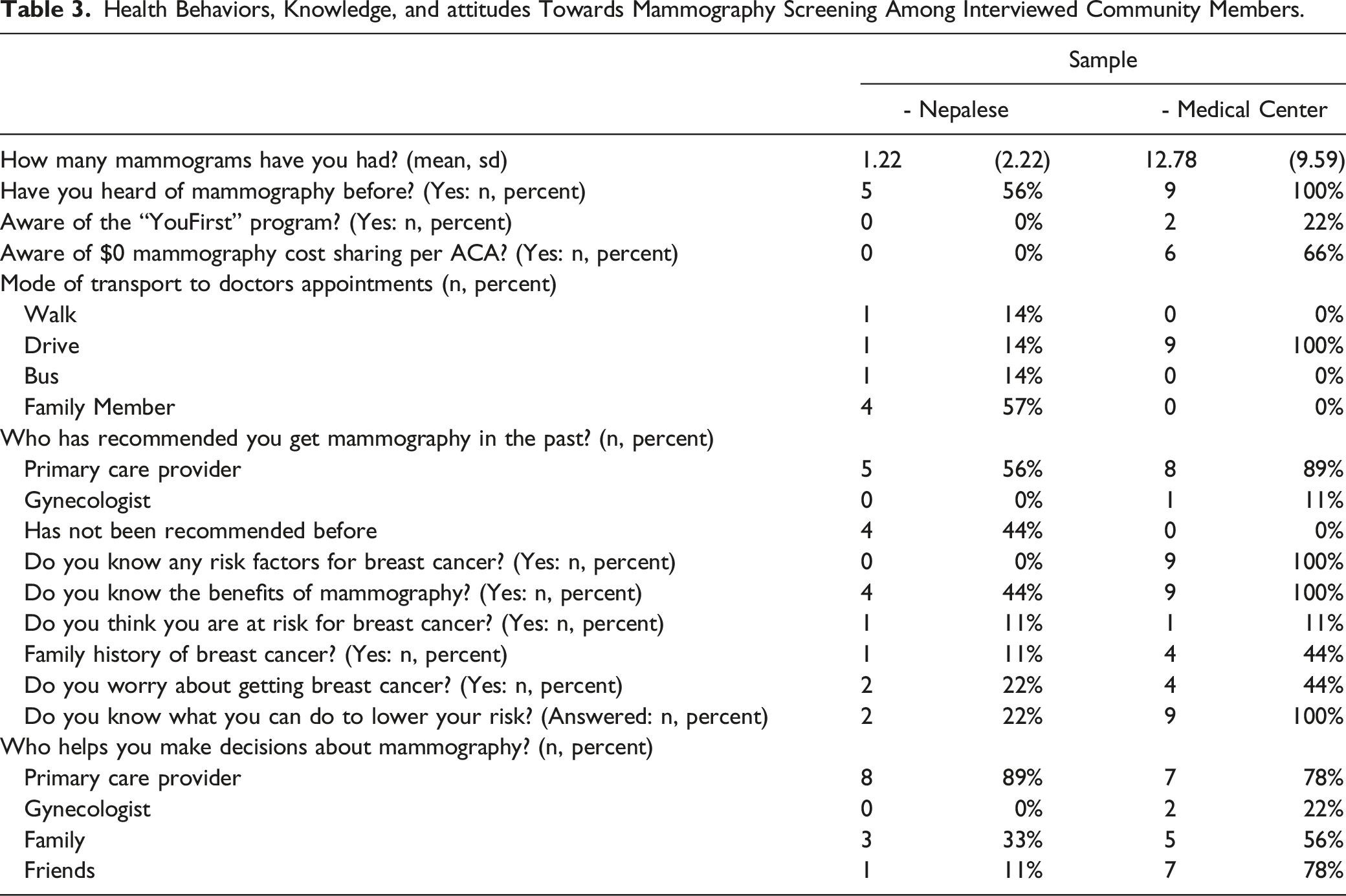
Health Behaviors, Knowledge, and attitudes Towards Mammography Screening Among Interviewed Community Members.
From our study, while all participants at the medical center (comparison group) had beyond high school education, all the Nepalese participants had less than high school education. Also, all the women at the medical center had full-time jobs, while 67% of the Nepalese population were unemployed and only 33% of them are in full time employment (Table 2). All medical center participates owned their homes however, only 33% of the Nepalese population owned houses and the remaining 67% rent their homes (Table 2). The sociodemographic characteristic may influence the perception and access to mammography screening at medical center. These findings are similar to a prior study conducted to explore women’s views and personal acceptability of a potential risk-based mammography screening paradigm where their convenience sample method revealed that all participants were white women and highly educated. 26
Perceived susceptibility refers to an individual’s belief that a health problem is personally relevant or that a diagnosis of illness is accurate. 27 In this context, if the woman perceives that she has a high risk of getting breast cancer, most probably, she will execute into the intended behavior of reducing the risk of breast cancer or to advert it. 28 The greater the perceived risk of breast cancer, the greater the likelihood of engaging in behaviors to screen for it. Conversely, when women believe that they are not at risk for the disease, they are less likely to engage in early detection practices. Almost all women uniform agreed they are not at risk of breast cancer for both of our study population. While the Nepalese population could not identify the basis for this, the patients in the comparison group based their reason for not being at risk on information of breast cancer acquired through personal interest and research.
Perceived severity refers to one’s belief about the severity of a disease based on medical information and personal beliefs they may have about the difficulties a disease will cause for their life. 27 For example, women who perceive breast cancer as a minor ailment are less likely to try to prevent its occurrence. If she perceives that the consequences of being diagnosed with breast cancer are very serious, she may probably go for screening, executing the intended behavior to prevent or reduce the severity. 28 We examined knowledge on breast cancer disease and risks, previous mammogram, access to primary care provider (PCP), previous breast cancer symptoms experience, risk of breast cancer and previous breast cancer diagnosis in the family.
Among the Nepalese population, the majority of the interviewees mentioned that they were not at risk for breast cancer. However, knowledge of breast cancer is missing among this population as well. About half (56%) of the Nepalese population had some knowledge of mammography and all the women at the medical center are knowledgeable about mammography (Table 3). Women in the comparison group were more informed and a number of them had an increased awareness of the risks of breast cancer disease. Hence, majority of the comparison group identified as being at risk for breast cancer from a prior breast cancer diagnosis among family members. Overall, the limited knowledge of breast cancer among the Nepalese women may influence their perception of the risk associated with breast cancer disease. Despite the paucity of knowledge about breast cancer disease and risks, after careful explanation of the topic, the Nepalese population were willing to be screened for breast cancer.
Perceived benefits are an individual’s opinion of the effectiveness and value of behaviors to prevent disease acquisition. 27 If the woman believes that she will gain positive returns from her outcome expectancy, she will most likely engage into the recommended behavior of getting screened. 29 Although there is extensive evidence that supports the benefits of screening, women have to believe that there is a personal benefit for adopting the behavior. The gain to be made by taking the action is a reduction in the seriousness of the disease, or an increase in awareness of the benefits of breast cancer screening. The majority of the Nepali participants don’t know the benefits of breast cancer screening. Our study show that 44% of the Nepalese interviewees are aware of the benefits of mammography screening compared to 100% of the patients interviewed at the medical center (Table 3).
None of the Nepalese women were worried about getting breast cancer. That being said, from our study these women also have no knowledge about breast cancer. Their lack of knowledge thereof may be the reason they’re not worried about getting breast cancer. The women in the comparison group who aware of the benefits of breast cancer screening mentioned early detection as beneficial to improving breast cancer mortality, and generally had greater health literacy level.
Perceived barriers are the most significant factor in determining behavioral change. This is an individual’s evaluation of the costs and obstacles in their way of establishing a new behavior.27,30,31 Transportation barriers, financial costs associated with physician visits, knowledge, and belief systems are all reasons why women may choose not to seek breast screening. Perceived barriers are obstacles that women face in taking action towards getting mammography screening. For this, we examined fear and cost of mammography screening, transportation or access to the doctor’s appointment, previous negative experience in seeking healthcare, ease of discussing breast cancer with their primary provider, and COVID-19 barrier to breast cancer screening.
Transportation was a major barrier for getting healthcare among the Nepalese women. Most of them need to rely on the family members to get to their appointments, and many found it difficult to get to their physician’s appointments. “This morning, I was told to come back at 1 p.m.. I was asked if someone else can bring you to this appointment at 1 o’clock. I told them my son leaves at 1 p.m. for work and then my daughter-in-law will leave at 2 p.m. for her work, so there is no one to bring me to the appointment”. “Transportation is a major issue for me. The last couple of days, I missed appointments. When my kids have time, they do give me a ride, but I do face a lot of problems because transportation is an issue and I miss a lot of appointments.”
On the other hand, all the women on the comparison group have easier ways of getting to their appointments by driving. All the Nepalese women that were interviewed were satisfied by the healthcare services they received at medical center, they didn’t report any negative experiences in seeking healthcare, and they were comfortable asking their doctor about breast cancer. Additionally, all our interviewees in this study have health insurance coverage. Language barrier was evident in this study. The Nepalese interviewees could not speak English, and this has led to the main barrier identified; lack of adequate or timely translation services, which makes the women depend on their family members to fill this need.
Long wait times for mammography screening appointments were mostly mentioned as a barrier to seeking mammography among the white women who received screening. Very few of the women were aware of their medical insurance coverage for the cost of mammography screening. The fear of the cost of mammography could potentially deter their interest in seeking mammography. “Yes, that does happen, and we never know how much of the bill we have to pay out of pocket, so yeah, we do want to go to doctor and then consult them about our health concerns, but we never know how much you need to pay out of pocket. That’s why it does happen”.
None of the Nepalese women were aware of zero cost sharing per ACA coverage, and only 66% of the comparison group had knowledge of the zero-cost share available to them.
Cues to action or readiness to change are people, events, and external things that motivate an individual’s adoption of a new behavior. 27 If a woman is aware of the struggle a friend or family member is having with breast cancer, she will be more likely to engage in screening behavior. We examined personal efforts in preventing breast cancer, access to health insurance coverage and awareness of breast health promotion programs.
None of the Nepalese interviewees had knowledge of breast awareness programs. Some of the breast awareness programs for example, offers personalized support that offers to pay for and connect eligible residents to breast, cervical and heart screenings, diagnostic tests and heart healthy lifestyle programs. Most knowledge about breast cancer among the Nepalese population was from their healthcare providers. Consequently, those who had not been told about the need for mammography by their PCPs had no level of awareness of the screening, nor of breast cancer signs, symptoms, or risk factors.
As reported by the Nepalese women, three interviewees made decision for mammography screening from their friends and family, however the vast majority consulted solely with their primary care physician. When asked if our interviews who haven’t been tested would like to get tested, they were willing (some, eager) to get a mammogram.
The comparison group had great knowledge of breast cancer that was mostly from social media, internet, friends, and family. They receive most motivation for mammography screening from their primary providers more than family members or friends, though friends and social networks were a large supportive factor for many of the Nepali population. The differing literacy level among the two groups may be contributory to the various sources of information on mammography screening.
Self-efficacy is the belief that a change in behavior will result in a valued outcome and It’s one’s belief in their actual ability to achieve a certain behavior with accuracy. 27 For example, if a woman understands the benefits of mammograms but is not confident that she can go through with actual action of doing so, she is less likely to try it.
Most decision makers for breast cancer screening from our study were primary care providers, internet, television Ads, friends, and family. None of the Nepalese women knew what to do about preventing breast cancer. There were mentions of making healthy eating, breast self-examination and lifestyle choices to reduce risk of breast cancer by the medical center group. Education level and personal interest were very instrumental in spurring these actions. These are potential opportunities for interventions for reducing racial and ethnic disparities in screening mammography utilization among groups of minority women. 32
Discussion
This study explored Nepali women’s beliefs about access to mammography screening, and motivations to get screened or not. This work was intended to be hypothesis generating for subsequent quantitative analysis and to inform policy and decision-making to improve access.
Knowledge of mammography screening, and subsequent utilization, was found to be low among the Nepali women interviewed, aligning with documented disparities in the state’s Mammography Registry. PCPs emerged as a critical link in addressing this disparity: trust was found to be high among Nepali women with their established PCP, and those who had not had a conversation with their physician regarding breast cancer screening had no awareness of it.
Further, language and translation supports were identified as a large barrier to effective health communication for the Nepali population, with informational packets and scheduling reminders often mailed in English, where many of the recipients may not know English or be able to read at all. White women seeking mammography care at medical center reported thorough knowledge of screening practices and risk factors, positive experiences obtaining care, and easy access to care.
We conclude that the role of primary care physicians seems to be of critical importance, especially for underserved groups with limited health knowledge. An often-cited point of confusion among PCPs in regard to cancer screening is that of conflicting guidelines. Clinical recommendations for mammography screening ages and frequency are a shifting landscape and depending upon the authority which the clinician relies upon, patients may be getting screening far later than others.
The results of this study have important implications for public health programs in Vermont targeting women who are not getting mammography screening, most importantly the You First program. You First is a free program run by the Vermont state Department of Health (VDH), funded by two grants from the federal Center for Disease Control and Prevention. The program is designed to help improve access for disadvantaged women to get diagnostic and preventive health services. Current projects include providing access to breast and cervical cancer early detection screening, as well as heart health screening and heart disease prevention. The You First Patient Navigator helps guide members from screening to diagnosis to treatment. The You First Lifestyle Program Coordinator and Health Coach helps members achieve their fitness and nutrition goals for better heart health. Diagnostic services are a keystone to care-coordination regimens; barriers to diagnostic and preventive health services create a cascade of other access barriers.
You First has found inequitable access to healthcare services which is compounded by Vermont’s status as an overwhelmingly white state. You First collects and reports data on program enrollment based on federally defined racial ethnic groups. Yet different types of individuals within the same racial and ethnic categories may face different barriers. Programs like You First designed to address systemic racism potentially suffer from a lack of specificity about the critical heterogenous differences within racial and ethnic categories. The results from our study fill in some of the gap in knowledge. Previous studies in other parts of the county and nationally have addressed barriers to accessing mammography, such as transportation, language, and knowledge deficit.33,34 Our results agree with this previous research and add that individual perceptions and emotions like trust in the health system are important contributors to improve screening rates among the Nepali women. Future research will have to focus on other underserved populations and to what extent these aspects affect decisions to get mammography screening.
Limitations
This was a pilot qualitative study among one of the underserved populations in the relatively small and rural state of Vermont. This study was hypothesis generating and results cannot be generalized. Further study on equity of access to (and uptake of) mammography screening along racial, ethnic, and socioeconomic lines should be undertaken to drive cancer surveillance and prevention policies forward in a data-driven way. Because all races are not alike, approaches to bridging the disparities in screening be contextualize approaches for driving access to mammography screening. medical center and its community primary care partners should critically evaluate the language access supports available to patients and their families: steps should be taken to ensure that patients are receiving communications from their medical home in a language and format which they can understand and reliably receive.
While mammography coverage exists in ACA, most beneficiaries are not aware of this provision. To this end, several measures should be taken to increase beneficiaries’ awareness on this coverage. The impact of primary care providers’ roles in mammography screening rates cannot be overstated, and should be a target of future research, especially considering the ever-shifting landscape of clinical recommendations, which often conflict with one another, leaving some patients in the dark.
Conclusions
Health behaviors are not monolithic within racial or cultural groups. In fact, racial/ethnic disparities may be a reflection of other underlying barriers, such as transportation barriers in rural areas and language barriers. It may also be a reflection of underlying cultural norms and beliefs or perceptions.
It is therefore important to further detangle social, behavioral, structural and policy factors that are sources of lower screening rates among non-white populations. Discrete choice modeling may be one way of providing more insight into the tradeoffs and relative importance of the factors influencing cancer screening uptake. This modeling could be beneficial to perform among both providers and patients to understand what may influence a provider to recommend screening, and what may motivate a patient to seek it.
Mammography is a critical tool in reducing the burden of breast cancer morbidity and mortality in our communities, and ensuring equitable access is of paramount importance. This work has identified several areas for future research to better guide policy making and clinical practice.
Footnotes
Acknowledgments
We would like to thank individuals at the Community Health Centers of Burlington (CHCB) for their support for this project and their feedback on our work. We gratefully acknowledge the valuable contributions provided by Dr. Michelle Dorwart. Any errors in the manuscript are the sole responsibility of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.