
Abstract
Introduction
Devastating cancer-related events are not uncommon, and these events have weakened communication performance and induced stress among health care providers (HCPs), particularly physicians. This study aimed to investigate the perspective of HCPs emotionally affected by poor clinical outcomes due to the failure of cancer therapy.
Methods
A cross-sectional, online survey was conducted over 3 months among HCPs practicing in the field of oncology in Saudi Arabia, comprising physicians, pharmacists, and nurses. Data were analyzed using Statistical Package for Social Sciences version 26.0. A P-value <.05 was considered statistically significant.
Results
This study demonstrated a positive correlation between HCPs’ length of experience and emotional impact of treatment failure, albeit this was not statistically significant (P = .071). Analysis of their perspective toward failure of cancer therapies revealed a significant impact of occupation and sex (P = .014 and P = .047, respectively). Moreover, occupation played a significant role in shaping the viewpoint of HCPs toward the need for conducing further research to test the appropriateness of treatment protocols on local patients (P = .022). Despite the emotional responses of HCPs to suboptimal clinical outcomes, factors such as work burnout, lack of concentration and patience, work or personal problems, and under appreciation were frequently identified as triggers of such outcomes.
Conclusion
Our results revealed that poor clinical outcomes observed among cancer patients are emotional triggers for HCPs practicing in the oncology field. The emotional response is often perceived negatively, and can potentially lead to a decline in the quality of care provided to these patients.
Keywords
Introduction
Although survival rates after cancer remission have significantly improved over the years, cancer relapse remains a major concern for patients and health care providers (HCPs).1–3 Devastating cancer-related events, such as cancer relapse or recurrence, are not an uncommon experience by patients, 2 and HCPs remain at the forefront of delivering such difficult news to patients and their families. As a result, HCPs may experience increased emotional distress and feelings of fear, stress, and anxiety. 3 Some devastating news that HCPs may have to convey include irreversible side effects of treatments and cancer relapse or progression as well as discuss hospice care, palliative care, and even resuscitation options when no other therapies are available. 4 In such situations, it becomes extremely challenging for HCPs to separate their emotions from these difficult consequences. Dealing with such circumstances requires the HCPs to manage the stress associated with the uncertainty of patient response and to have a high level of competence in managing all their emotional anticipations. 4
Several studies have investigated the impact of traumatic events on HCPs.5,6 Brown et al conducted a simulated patient consultation approach among 24 physicians, expert experience (≥4 years) and novice experience (1-3 years), and evaluated their stress response and communication performance when delivering bad vs good news. 5 The results of the study showed no difference in communication performance, depression anxiety stress score (DAS), and fatigue between the two groups at the beginning of the study; However, a significant increase in stress, reflected by elevated heart rate (HR), was associated with delivering bad news compared to delivering good news in both groups. This increase in stress was found to be related to fatigue and inexperience with delivering bad news. Additionally, poor communication performance was found to be related to burnout and fatigue levels. Another study by Cohen et al 6 was conducted to examine the impact of delivering good or bad news by medical students by evaluating their stress levels through monitoring blood pressure (BP) and HR during simulated physician–patient scenario. Although systolic BP and HR during preparation of delivering the news did not significantly differ between the good news group vs the control group, they were significantly higher in the bad news group vs the control group. Moreover, those in the bad news group had significantly higher stress levels and disrupted mood compared to the other groups. Furthermore, the study by Dulmen et al 7 on medical students revealed that anticipation of delivering bad news increased cortisol levels, cardiovascular activity (BP and HR), and anxiety. Interestingly, Shaw et al 8 reported similar apparent stress levels in both junior and senior physicians, indicating that medical experience was a negligible factor in reducing the stress of delivering difficult news over time. Nevertheless, senior physicians reported using problem-focused coping (PFC) strategies, such as selecting patients with better prognosis or an optimal environment for such disclosures, to reduce the impact of the difficult news and emotional interaction.
Despite the physiological and psychological impact of delivering bad news among physicians highlighted by previous study,5–8 limited research examining the impact of bad news on their emotions, perception on clinical performance and quality of care provided to patients thereafter. Therefore, our study aimed to assess the impact of delivering bad news on the emotions, perception of performance, and quality of care provided by clinicians practicing in the field of oncology.
Materials and Methods
A cross-sectional, online survey was conducted between January and March 2022 on HCPs practicing in the oncology field in Saudi Arabia. The HCPs comprised of physicians, pharmacists, and nurses. Participants were recruited through social media such as WhatsApp and were requested to complete the questionnaire one-time only to avoid response duplication. Those expressing willingness to complete the survey were included in the study. Since no such study has been conducted in the oncology field before, the questionnaire was developed after a review of literature,3–6,8–14 and a convenient sample approach was adopted. Participants were assured that the shared information was used solely for research purposes and would be kept private during the investigation. Participants who did not meet the inclusion criteria were omitted from the study. Ethical approval was obtained from the Institutional Review Board (reference number: E-22-6611).
The questionnaire was divided into 3 sections. The first section included 11 questions that identified participants emotionally affected by poor outcomes and assessed their perspective toward failure of cancer therapy. The second and third sections were initially measured on a Five-level Likert scale ranging from strongly agree to strongly disagree, but was later modified to a three-level scale (Agree, Disagree, and Neutral). The second and third sections included 4-7 statements that assessed the perspective of HCPs on the reasons and consequences of poor performance using a three-level Likert scale. The Arabic questionnaires were subjected to a pilot study, among randomly selected participants (n = 7), to examine the readability and ease of administration before the actual study. The results of the pilot study are not included in the main study. The Cronbach’s alpha score of the questionnaire was estimated at 0.847, indicating that the questionnaire was ready to be carried-out for the study.
Statistical Analysis
A descriptive analysis was used to assess the responses of HCPs and Chi-square test was used for categorical variables analysis. A P-value <0.05 was considered statistically significant, and the data were analyzed using Statistical Package for Social Sciences version 26.0 (SPSS Inc., Chicago, IL, USA). Figure 1 shows the details of the responses and design. Flow chart of the study.
Results
Baseline characteristics (N = 80).

Majority (91%) of the HCPs (those who responded yes or maybe) had tendencies to be emotionally affected by poor clinical outcomes of patients treated for cancer (Figure 2A). This was not influenced by sex, age, or occupation (Pearson Chi-Square: P = 0.568, P = 0.884, P = 0.468, respectively). However, it was notable that the length of experience in the oncology field tended to have a positive association with emotions (P = 0.071), such that 70.2% (33 of 47) of those with experience ≥6 years and 67% (22 of 33) of those experienced <6 years answered “Yes” to being emotionally influenced. On the other hand, 4.3% of those with experience ≥6 years responded “No” and confirmed being emotionally un-affected by poor clinical outcomes compared to 15.2% of those with experience <6 years. Further details are provided in Figure 2B and 2C.
Perspective toward poor clinical outcomes among health care providers who are or tended to be emotionally influenced (N = 73).
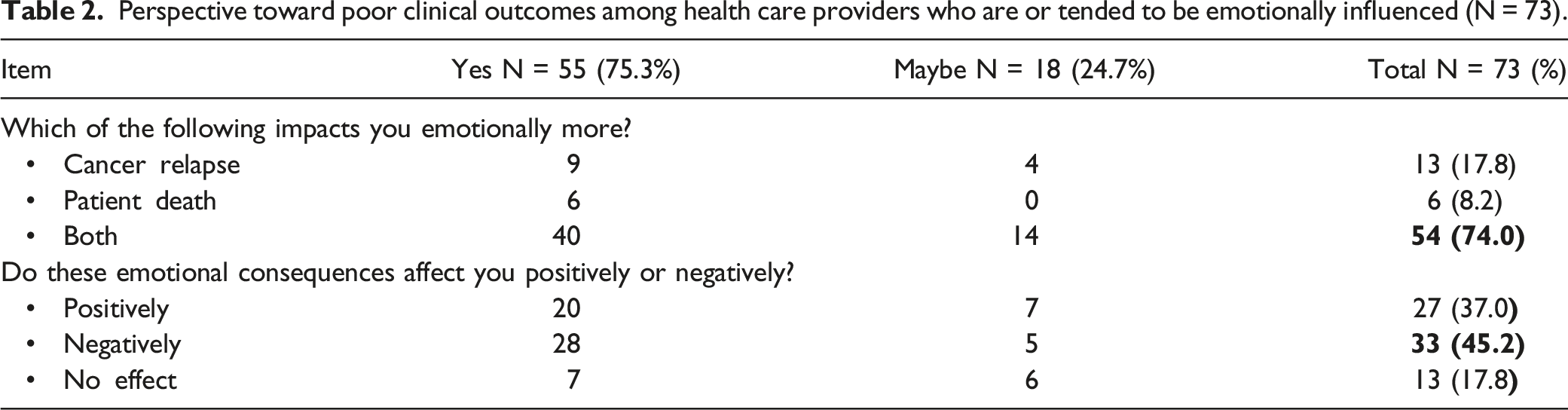
Additional analysis was conducted on the perspective of HCPs toward the failure of cancer therapies. Approximately half confirmed that delivering difficult news, such as cancer relapse and poor prognosis, had an impact on their general provision of patient care, which affected patients who have not relapsed (Figure 3). Moreover, approximately 60% denied low quality of care, work burnout, missteps in treatment protocols, or inappropriateness of treatment as reasons for cancer relapse or patient mortality. However, majority (≥75%) of the respondents questioned the efficacy of treatment modalities on their patients and felt the urge to conduct research to test efficacy, as some participants stated that these medications were tested on western populations and might produce different effects due to their genetic differences. Further analysis involving baseline characteristics was conducted to understand whether they contributed to these variations. Occupation and sex showed significant associations. For example, 52.4% of pharmacists speculated that low quality of care in their practice site as a reason for failure of cancer therapy while 71.4% of physicians (35 out of 49) and 66.7% of nurses (2 out of 3) denied that (P = 0.014). Additionally, more females (22.2%; 6 out of 27) than males (8.7%; 4 out of 46) considered low quality of care as a reason for failure of cancer therapy while this was denied by 69.6% (32 of 46) and 40.7% (11 of 27) of males and females (P = 0.047), respectively. With respect to following protocols correctly, 67.3% of physicians denied this as a reason for failure of cancer therapy, while 66.7% of pharmacists and nurses answered “maybe” (P = 0.005). Regarding the perception of HCPs toward the need to conduct research and test the appropriateness of treatment protocols on their patients, it was significantly affected by the occupation (P = 0.022), where 71.4%, 100%, and 66.7% answered “yes” while 28.6%, 0%, and 33.3% answered “no” among physicians, pharmacists, and nurses, respectively. Further details on justifications of those who thought inappropriateness of treatment or missteps in treatment protocols as reasons for cancer relapses or patient mortality are provided in Supplementary Table 1. Impact of emotions among health care providers who had tendencies to be emotionally influenced (n = 73) on their perspective toward failure of cancer therapy (relapse or death). *Responses significantly affected by occupation. # Responses significantly affected by sex.
Perspective of health care providers toward reasons contributing into poor clinical outcomes observed in cancer patients (N = 80).

Perspective of health care providers toward consequences of poor clinical outcomes observed in cancer patients (N = 80).

Discussion
The present study examined whether devastating clinical outcomes observed in cancer patients provoked emotional responses from HCPs in the oncology field and if these responses affected the performance and quality of care delivered to patients diagnosed with cancer. Around 91% of HCPs had tendencies to be emotionally influenced by poor clinical outcomes, which is often perceived negatively. This is concerning since negative emotions have been related to a decline in the overall performance of HCPs, both personally and professionally, and linked with suboptimal quality of care delivered to patients.15,16 Although results related to the impact on performance from our study is still to be investigated, our findings resonate with these results, as approximately half of the HCPs who were emotionally influenced confirmed the impact of failure of cancer therapies on the quality of care provided to their patients, including those who have not relapsed or had disease progression.
Several factors, including sex, age, occupation, and length of experience in the oncology field, could influence the emotional response of HCPs to poor outcomes, and their perceptions on these emotions and failure of cancer therapies. In this study age, sex, and occupation had no effect on the emotional response of the respondents. With respect to the length of experience, it was generally assumed that with multiple exposure to cases and over time, the emotions of HCPs would acclimatize; however, our results revealed that longer experience in the oncology field tended to have a positive association in those who were emotionally influenced (P = .071). Interestingly, a study by Shaw et al 8 showed that longer experience in the medical field had no influence on the stress level of participants delivering bad news and emotional interaction when compared to those with less experience. However, their findings revealed that more strategies to reduce emotional interactions were used by the former group, which probably led to the speculation that an increase in emotional interactions if these strategies were not adopted. Another study reported no impact of experience on the stress level, fatigue, and communication performance of participants. 5 Despite variation in results, there seems to be a consensus on no impact of experience on stressfulness and emotional response of HCPs to bad news or poor outcomes observed in cancer patients.
Our study revealed that majority of HCPs questioned the efficacy of cancer therapies used to treat their patients and highlighted the need to conduct further research to test these treatments on local patients before adopting them in treatment protocols. This is partly attributed to the genetic disparities that is believed to be associated with variable responses amongst patients from different ethnicities. Accordingly, published literature also states that race and genetic differences have long been known to impact the incidence of and survival with various cancers, besides patient response to treatments. 17 Therefore, when conducting scientific research, it is important to note such genetic disparities, in addition to other factors, including, but not limited to sex, age, and ethnicity, as they may significantly influence the study results and affect generalizations. 18 Although a diverse inclusion of participants in a study might maximize generalizations, shortcomings arise and not all populations would be adequately represented. 18 Thus, further research is warranted on the efficacy and overall clinical outcomes related to the use of cancer therapies (chemotherapies brands or generics and biological therapies including biosimilars) in different populations. Clinical trials conducted in Saudi Arabia are necessary to develop tailored and population-centered protocols based on such genetic variations.
Finally, delivery of bad news is an extremely burdensome task on clinicians and often occurs in the oncology settings. 3 To adequately support professionals in the workplace and assist in overcoming such a difficult task, a tailored, problem-solving approach to delivery of difficult news must be adopted. 16 One approach to this is the consensus method, which encompasses a consensus among a panel of oncologists, surgeons, general practitioners, nurses, human rights representatives, and other HCPs. Based on the available data, the panel then establishes a joint decision on the presented case. 3 Offering stress-management interventions such as counseling, workshops, and training programs have also shown to be beneficial in reducing occupational stress among HCPs. 16 Overall, this would potentially ameliorate the impact of the delivering difficult news on emotions, clinical performance, and quality of care.
This study has some limitations. First, this was a descriptive study that focused on assessing perspectives and beliefs of HCPs in the field of oncology and the impact of poor outcomes from different points of view. Second, the study lacked assessment tools that could have been used to objectively determine physiological, psychological, emotional outcomes (i.e., simulated case scenarios, depression/anxiety assessment scales, and BP and HR monitoring), and consequent impact on the clinical performance. Despite these limitations, this study remains to be crucial in unveiling the existence of these issues. Subsequently, further investigations can be conducted to determine the clinical impact of these events, as well as demonstrating strategies to fix these. Third, the participation rate was considered low with respect to the whole sample and extremely low from nurse practitioners, which limited the generalizability of the results. Despite these limitations, to the best of our knowledge, this study is the first to establish the foundation of research on this issue in the oncology field, which can potentially be simulated in other clinical fields.
Conclusion
Poor clinical outcomes are emotional triggers for HCPs, particularly in those practicing in the field of oncology. These outcomes could be perceived negatively and potentially lead to a reduction in the quality of care provided to patients with cancer. Work burnout and self-isolations, among other factors, were considered reasons of poor clinical outcomes, whereas psychological and physical stress could be attributed to these outcomes. Length of experience and age of HCPs tended to affect the emotional response and perception to these emotions. Occupation and sex had a significant influence on the perspective toward reasons of cancer therapy failure and the necessity of conducting research on treatment protocols used for local patients.
Supplemental Material
Supplemental Material - The Impact of Cancer Relapse and Poor Patient Outcomes on Health Care Providers Practicing in the Oncology Field
Supplemental Material for The Impact of Cancer Relapse and Poor Patient Outcomes on Health Care Providers Practicing in the Oncology Field by Abdulrahman Alwhaibi, Miteb Alenazi, Bana Almadi, Nora aljabali, Sahar Alkhalifah, Wajid Syed, Reem Alsaif, Salmeen D Bablghaith, and Mohammed N Al-Arifi in Cancer Control
Footnotes
Acknowledgments
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author (Abdulrahman Alwhaibi) received a fund from the Researcher Supporting Project number (RSPD-2023R572), King Saud University, Riyadh, Saudi Arabia, to support the publication of this article. The funding agency had no role in designing the study, conducting the analysis, interpreting the data or writing the manuscript.
Ethics Approval
This study received an approval from the institutional review board at King Khalid University Hospital (Research Project No. E-22-6611).
Data Sharing Statement
AA, MA, SB and MA have access to the data and take responsibility for integrity of the data and analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.