
Abstract
Purpose
This study aims to determine the optimal cut-off value of Ki-67 to better predict the recurrence of early low-risk endometrial cancer (EC).
Methods
Seven hundred and forty-eight patients diagnosed with low-risk EC from West China Second Hospital of Sichuan University and the First Affiliated Hospital of Chongqing Medical University were retrospectively analyzed. The receiver operating characteristic curve (ROC) and Youden index were used to calculate the optimal cut-off value of Ki-67 expression. The clinicopathological indexes between two groups divided by cut-off value of Ki-67 were compared. The univariate and multivariate regression analyses were performed to investigate risk factors connected to the recurrence of early low-risk EC. The survival analysis was shown in Kaplan–Meier curve.
Result
Thirty-three patients were detected with tumor recurrence after primary surgery (4.4%); 33% was the optimal cut-off value of the Ki-67 index. A high Ki-67 was significantly associated with age (P = .002), myometrial invasion (P < .001), and the expression of P53 (P = .007). The multivariate regression analysis verified that Ki67 ≥ 33% was an independent prognostic factor for predicting recurrence. The recurrence-free survival (RFS) and the overall survival (OS) in high Ki-67 group was significantly lower than that in low Ki-67 group (P < .001 and P = .029, respectively). The prognostic values of ER, PR, and P53 in combination with Ki-67 were superior to each single predictor.
Conclusions
The optimal cut-off value of Ki-67 for predicting recurrence is 33%, which quantitatively defines the specific value of Ki-67 that causes high-risk recurrence in early low-risk EC.
Indroduction
Endometrial cancer (EC) is regarded as one of the common malignant tumors of the female reproductive system. According to cancer statistics, there are approximately 63,000 patients suffering from endometrial cancer each year in the United States, and its morbidity and mortality are gradually increasing yearly with a mortality rate up to 18%.1,2 A great majority of patients (70%–80%) can be diagnosed at the early stage and surgery is the major curative strategy, the 5-year overall survival can be more than 80%. 3
The European Society for Medical Oncology (ESMO) and Japan Society of Gynecologic Oncology guidelines (JSGO) have classified endometrial cancer into three risk groups, the early low-risk EC was defined as tumor confined to the uterine corpus with myometrial invasion less than 50% and histological grade 1 or 2, endometrioid pathological subtype.4–6 Several studies have confirmed that factors such as surgical stage, histological grade, pathological type, depth of myometrial invasion and lymphovascular space invasion, squamous differentiation, and tumor size are related to the recurrence of endometrial cancer.7–12 However, some patients with low-risk endometrial cancer still suffer relapse or metastasis after surgical treatment in clinic on the occasion of without unfavorable factors such as stage, tumor grade, and pathological type, which is one of the main causes leading to death of patients in such subtype. Nevertheless, the prognostic factors related to the recurrence of low-risk endometrial cancer in early stage are indistinct and ambiguous, and most relevant studies are simply focus on the analysis of some classical factors. There is limited capacity for traditional clinical parameters to predict endometrial cancer recurrence, which remind us more exploration on relapse and prognosis should be carried out.
With the development of molecular biology, immunohistochemical markers have been used as the important indicators to predict the cancer prognosis. Ki-67 index, as a nuclear antigen correlated to cell cycle, reflects cell proliferation and can be easily detected by immunohistochemistry. It does not show in the cells of mature tissues and express in all stages of cell proliferation (G1, S, G2, and M). It contributes to better estimate the aggressive biological behavior of malignant tumor cells. Previous studies have reported that Ki-67 is seriously connected with tumor development, metastasis, and prognosis.13,14 As the reports on breast cancer illustrated, Ki-67 plays a crucial role in prognostic evaluation and Ki-67 expression>20% has been verified as an independent risk factor of poor prognosis. 15 However, there is lack of theoretical consensus on the relationship between Ki-67 and the prognosis of endometrial cancer, particularly the exploration of cut-off value and clinical application significance of Ki-67. It is necessary to taking further exploration on the relationship between Ki-67 and the prognosis of endometrial cancer, especially among early low-risk endometrial cancer, it is more valuable to evaluate prognosis and guide treatment of patients with such subtype patients.
Therefore, the purpose of this study is to investigate the optimal cut-off value of Ki-67 in predicting recurrence of early low-risk endometrial cancer.
Materials and Methods
Study Population
The clinical data of patients diagnosed with endometrial cancer in the West China Second Hospital of Sichuan University and the First Affiliated Hospital of Chongqing Medical University between January 1, 2013 and April 7, 2022 were retrospectively recorded. All of them underwent primary surgical treatment including at least total hysterectomy and bilateral salpingo-oopherectomy with or without pelvic or para-aortic lymphadenectomy. The cases conforming to following criteria were included: (1) Patients diagnosed as stage IA endometrial cancer according to 2019 International Federation of Gynecology and Obstetrics (FIGO) guidelines without high grade endometrial cancer. (2) postoperative pathological type was endometrioid adenocarcinoma. Besides, the exclusion criteria were as follows: (1) Age ≥60 years; (2)Patients accompanied with secondary endometrial cancer or other malignancies and fatal complications; (3) Patients accompanied by lymphatic vascular infiltration (LVSI); 4)Patients lost follow-up; (5) Treatment inconsistent with standard surgical approach; (6) The medical record was incomplete. The information of clinicopathological data were recorded completely including age of patients, stage, BMI, grade, myometrial invasion, lymphadenectomy, and immunohistochemical markers. This study complies with the ethical standards of the Helsinki Declaration and has been authorized by the Ethics Committee of the Ethics Committees of West China Second Hospital of Sichuan University (343, December 19, 2022) and the First Affiliated Hospital of Chongqing Medical University (2020-166, March 18, 2020). All patients have provided verbal declaration of informed consent for research implementation and publication. All patient details have been de-identified. The reporting of this study conforms to REMARK guidelines. 16
Histology and Immunohistochemistry
Postoperative specimens were immediately fixed in formalin and sent to the corresponding institution for pathological analysis using uniform standard procedure. All samples were made into paraffin-embedded specimens. Secondly, H&E staining was used to confirm the lesions, and each sample was made into a 2 mm thick wax block. Then, the immunohistochemistry (IHC) of estrogen receptor, progesterone receptor, Ki-67, and P53 was performed using an automated immunostainer (Leica Bond-Max, Milton Keynes, UK). The antibodies, such as ER (SP1, rabbit antibody, ready-to-use), PR (SP2, rabbit antibody, ready-to-use), Ki-67 (MXR002, rabbit monoclonal antibody, 1:500), and P53 (MX008, mouse monoclonal antibody, 1:500), were used in IHC. Percentage of positive cells by immunohistochemical staining represents the expression level of ER, PR, P53 and Ki-67.
The results of tumor type, differentiation, infiltration extents, lesions size, and quantification of immunohistochemical markers were initially interpreted by a junior professional gynecological pathologist, and then reviewed by a superior physician. According to relevant research reported, the expression of ER and PR were defined as negative if the positive staining cells were less than 10% of the tumor cells, respectively, 17 While tumors with more than 25% of the tumor cells showing P53 positive staining were regarded as positive. 18 The level of Ki-67 expression was expressed by the percentage of positive staining cells (0%–100%).
Recurrence and Follow-up
All the patients were scheduled to follow-up from the day of surgery and complied with the normative strategy as follows: every 3 months for the first 2 years after surgery, every 6 months for the next 3 years, and annually for 5 years later. The gynecological examinations, serum tumor markers, vaginal cytology, and diagnostic imaging examinations were as necessary during regular follow-up, especially some abnormal phenomena occur. The location of recurrence occurred in the vagina or pelvis was recognized as a local recurrence, whereas distant recurrence included para-aortic lymph node metastasis, abdominal metastasis, or metastasis to other organs. 4 Recurrence-free survival (RFS) was calculated as the time from surgery to relapse or the last follow-up date, while overall survival (OS) was the time from surgery to death or the last follow-up date.
Statistical Analysis
Continuous variables were expressed by median, and rank sum test were used to compare differences. Categorical variables were expressed by frequency and percentage, and the comparison was conducted by using Chi-square test. The area under the receiver operating characteristic curve (ROC) examined the effectiveness of variable to predict recurrence and Youden index (sensitivity+specificity-1) was used to calculate the optimal cut-off value of the variable. Predictors for relapse in early low-risk endometrial cancer were determined by univariate and multivariate COX regression analysis. The recurrence-free survival and overall survival were shown in Kaplan–Meier curve and log-rank test was used to examine the survival differences. All statistical analyses were implemented using SPSS software (IBM SPSS 26). The P value <.05 in two sides test was regarded as statistically significant.
Result
Clinicopathological Characteristics in Study Patients
A total of 1505 patients with stage IA endometrial cancer who only underwent surgery was registered, after screening according to the inclusion and exclusion criteria, 748 patients were finally included in this retrospective study (Figure 1). The median age of the patients was 50 years (range 23-59 years). Among 748 patients, 526 (70.3%) were exhibited in high differentiation and 222 (29.7%) were found to be moderately differentiated. Lesions confined to endometrium were in 252 patients (33.7%) and superficial muscular infiltration was in 496 patients (66.3%). The expression level of Ki-67 was between 0 and 90% (median 30%). The median follow-up time was 60 months (range 7–103 months). Finally, 33 cases (4.4%) developed recurrence and 17 cases encountered death, among which 17 cases (2.2%) reported local recurrence and 16 cases (2.1%) reported distant recurrence. The remainder items were shown in Table1. The flowchart of screening of patients. Clinical and Pathological Characteristics of the Patients. BMI, body mass index; ER, estrogen receptor; PR, progesterone receptor.

The optimal Cut-Off Value of Ki-67
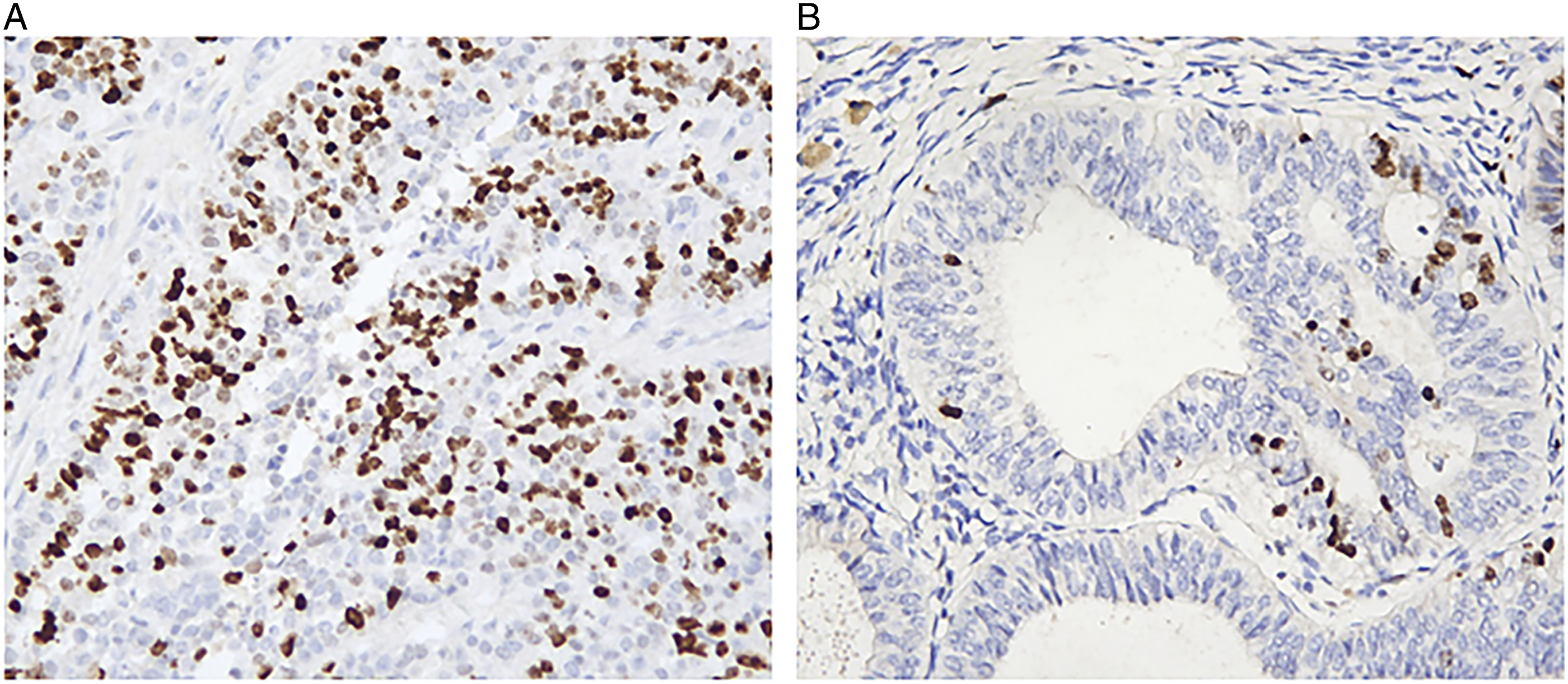
The relationship between recurrence of low-risk endometrial cancer and expression level of Ki-67 was shown in ROC curve (Figure 2). It revealed that the optimal cut-off value of Ki-67 expression corresponding to maximum of the Youden index was 33% (n = 748, AUC = .739, sensitivity 78.8%, specificity 57.1%, P < .001, 95% CI = .665-.813). The Ki-67 immunohistochemical analysis of this cut-off value in a representative sample was shown in Figure 3. The receiver operating characteristic curve (ROC) analysis of the relationship between Ki-67 expression level and recurrence. The solid line: The Ki-67 line. The dotted line: Reference line. The blackspot: the optimal cut-off value of Ki-67 expression. The immunohistochemical analysis of Ki-67 in a representative sample. (A) The Ki-67 expression was reported at 60%. (B) The Ki-67 expression was reported at 5%.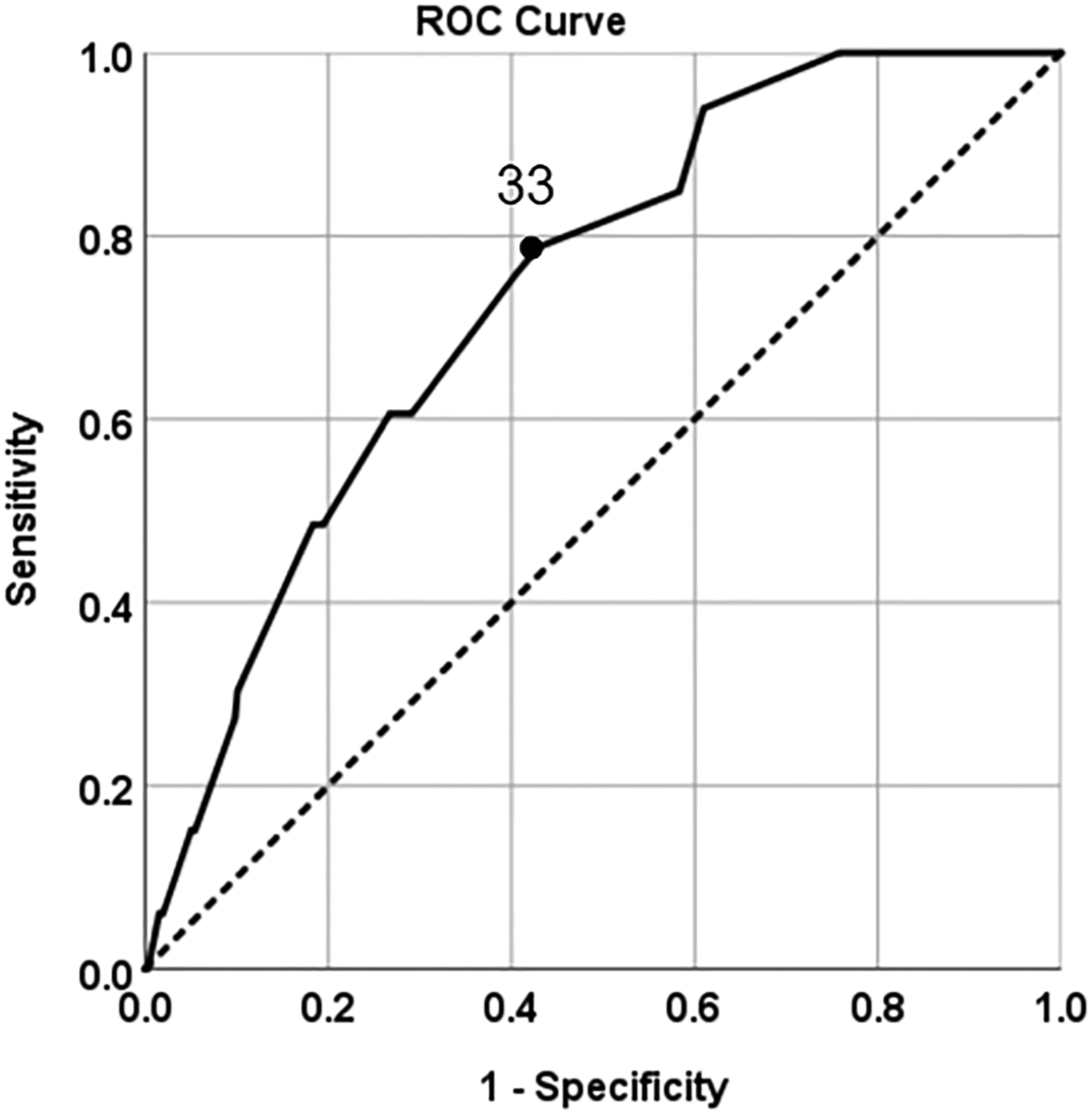
Correlation Between Ki-67 Expression and Clinicopathological Characteristics
Relationship Between the Expression Level of Ki-67 and Clinicopathological Features.
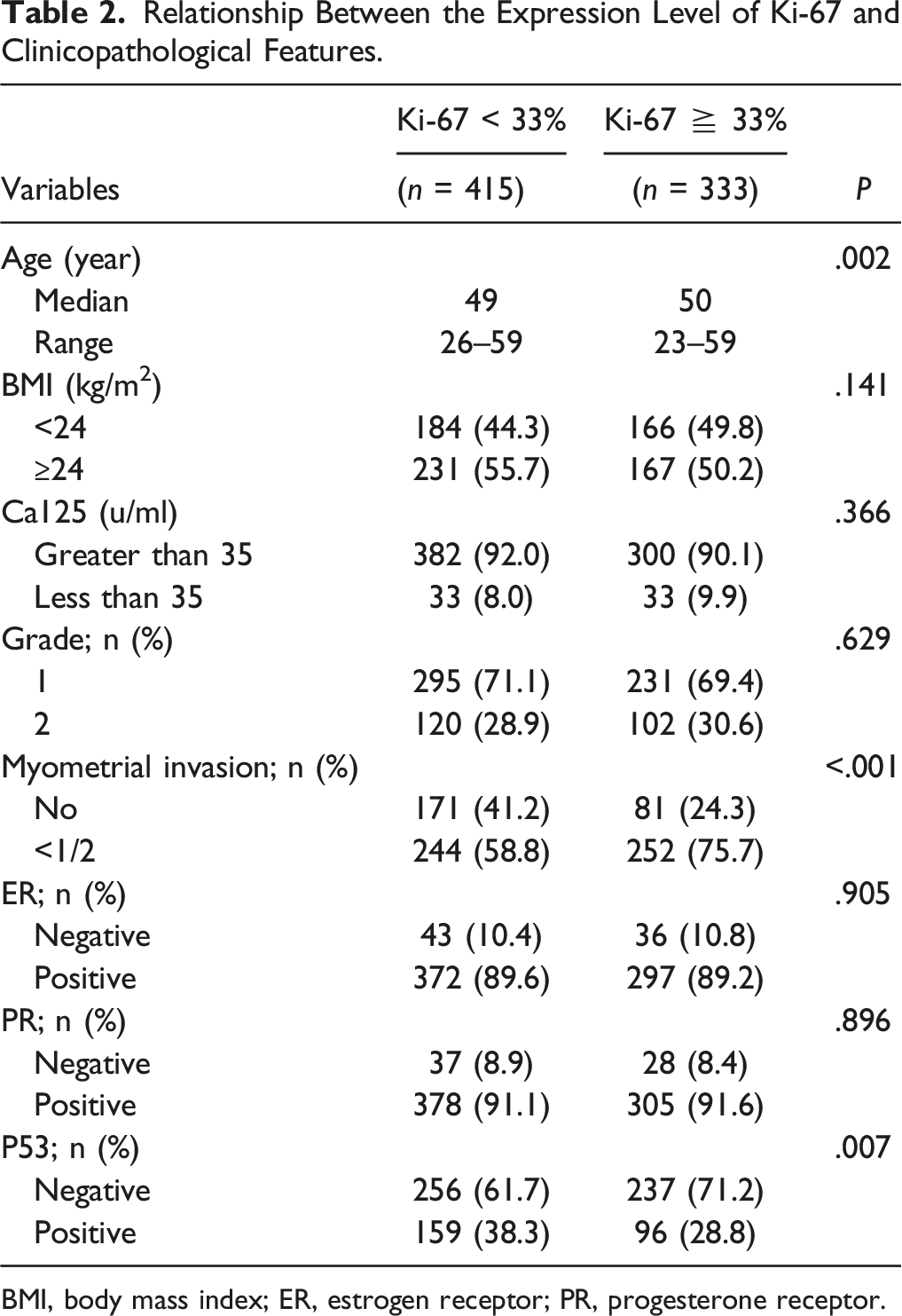
BMI, body mass index; ER, estrogen receptor; PR, progesterone receptor.
Predictors for Relapse in Low-Risk Endometrial Cancer and Survival Analysis
The Factors Predicting Recurrence in Early Low-Risk Endometrial Cancer by the Univariate and Multivariate COX Regression Analysis.
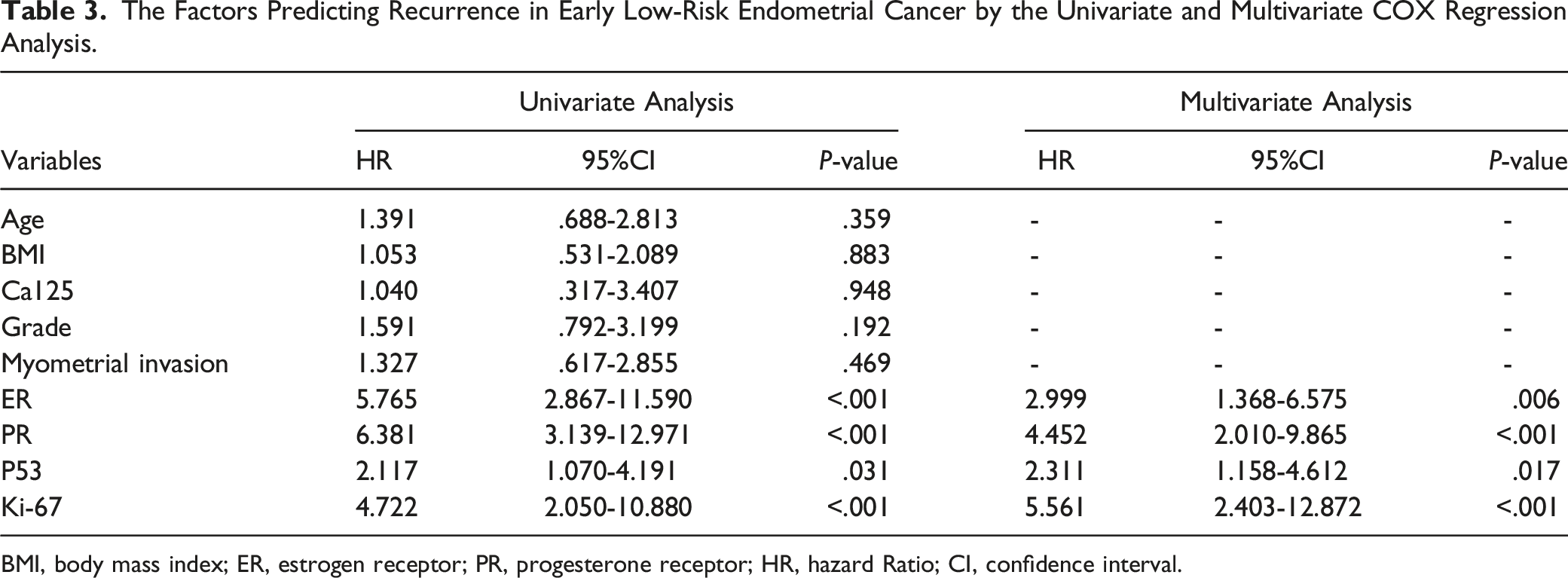
BMI, body mass index; ER, estrogen receptor; PR, progesterone receptor; HR, hazard Ratio; CI, confidence interval.

(A) The recurrence-free survival of patients in the low Ki-67 group and the high Ki-67 group. The solid line: The survival curve of the patients with Ki-67 < 33%. The dotted line: The survival curve of the patients with Ki-67≧33%. (B) The overall survival of patients in the low Ki-67 group and the high Ki-67 group. The solid line: The survival curve of the patients with Ki-67 < 33. The dotted line: The survival curve of the patients with Ki-67≧33%.
The Prognostic Value of ER, PR, and P53 Combined with Ki-67
Considering that this multivariate analysis showed that ER, PR, and P53, as independent risk factors of cancer recurrence, were closely related to the prognosis of endometrial cancer. Therefore, we used the ROC curve to compare the prognostic value of ER, PR and P53 combined with or without Ki-67 (Figure 5). And we found that the prognostic values of Ki-67 combined with ER and PR (AUC = .794, 95% CI = 71.1%–87.8%) was superior to each single predictor, including ER (AUC = .651, 95% CI = 54.1%–76.1%), PR (AUC = .645, 95% CI = 53.4%–75.6%), ER and PR (AUC = .738, 95% CI = 63.6%–83.9%). Similarly, Ki-67 combined with P53 (AUC = .731, 95% CI = 65.2%–81.1%) was superior to the single predictor, P53 (AUC = .591, 95% CI = 48.9%–69.3%) (Table 4). The prognostic value of ER, PR, and P53 combined with Ki-67.
Discussion
The Prognostic Value of Ki-67 Combined With P53 and ER or PR.

In this present study, the recurrence rate in low-risk endometrial cancer was shown as 4.4%, exactly consistent with 4%–7% reported in previous research.5,21 It seems to be considerable merely considering the absolute recurrence rate in this subtype, which may attribute to the fact that multitudinous patients can get a diagnosis at an early stage and timely treated before the tumor progress to serious malignant invasion. Nevertheless, with respect to the increasing incidence of endometrial cancer worldwide, clinicians inevitably undertake the obligation to manage early low-risk endometrial cancer recurrence, the investigation of some potential unfavorable prognostic factors resulting in relapse must gain great value for preventing tumor recurrence. Besides, ROC curve analysis revealed that 33% was the optimal cut-off value of Ki-67 for the recurrence in early low-risk endometrial cancer. Even if the specificity was only 57.1%, the maximum value of the Youden index guarantees the greatest sensitivity while assures the highest specificity rather than only concentrate on the specificity or sensitivity. In addition, this study provided a specific value to explain the high or low expression level of Ki-67 rather than just vaguely saying the expression is high or low, which enable Ki-67 to assess the recurrence risk in a more quantitative and standardized form. With the cut-off value 33%, patients in the high Ki-67 group were reported to accompany with invasive clinical factors and immunohistochemical markers, such as older age, myometrial invasion, and positive P53 expression. This is because Ki-67 is considered as a tumor proliferation index and reflects the increased aggressiveness of tumors. This is why there is high Ki-67 in some low-risk tumors and this may also explain why there was a poor prognosis in some low-risk patients. As previous studies displayed, it supported the hypothesis that high-level Ki-67 expression may generate negative outcome.13,22 Moreover, it was timely presented in multivariate analysis that Ki-67≧33% was an independent risk factor for recurrence of early low-risk endometrial cancer. The 3-year recurrence-free survival and overall survival in patients with Ki-67≧33% were detected a statistically significant reduction. Previous studies have suggested that for early endometrioid adenocarcinoma, postoperative adjuvant radiotherapy, or chemotherapy is not recommended considering patients without high-risk factors such as advanced stage, poor differentiation and pathological type. However, this study indicated that under the situation that low-risk endometrial cancer was without aggressive clinical parameters, the immunohistochemical markers show the very particularly significance. So, it should value that active and comprehensive postoperative management was supposed to be taken for patients who were encountering high Ki-67 expression, including more frequent postoperative follow-up to manage the disease, or appropriate postoperative adjuvant treatment to be employed for decreasing recurrence instead of simply follow-up. Postoperative radiotherapy can effectively control local recurrence in early patients and chemotherapy can reduce the recurrence rate and improve the overall survival of advanced patients.23,24 Moreover, in this study, we also demonstrated that combining ER, PR, P53, with Ki-67 to evaluate the prognosis of endometrial cancer can further reinforce the prognostic value of a single index, especially verify the value of Ki-67, which is providing a theoretical basis for the application of molecular indices in early low-risk endometrial cancer in the future.
As respected in studies on endometrioid adenocarcinoma, it has demonstrated that age >60, myometrial invasion and poor differentiation are high-risk indicators related to prognosis and recurrence.25–27 Kyung et al has reported that the grade and myometrial invasion were prognostic factors affecting recurrence of patients with stage I endometrioid cancer, for stage IA only myometrial invasion was the high risk factor, while for stage IB only grade was the high risk factor. 27 Obviously, even in early stage, there will be differences in the prognostic factors that affect recurrence for cancer in different stages. Therefore, in this study, we just contained early low-risk endometrial cancer and it elaborated that age, myometrial invasion and tumor differentiation were lack of significantly statistical connection with recurrence. This conclusion illuminated that traditional tumor morphology was restricted by the subjective factors and the classic clinical parameters have been insufficient to effectively predict the recurrence of such early low-risk endometrial cancer. At present, immunohistochemical markers which proved to be seriously associated with tumor recurrence have been commonly applied in clinical practice, the sensitivity and specificity superior to traditional morphological features. Thus, only stratifying endometrial cancer at risk based on clinical parameters is inundated with one-sidedness and deficiency. In addition, this study has confirmed that the immunohistochemical markers Ki-67 and ER, PR, and P53 are associated with poor prognosis of patients. It is prospective that immunohistochemical indicators may be used as criteria for early stage endometrial cancer risk stratification, which establishes theoretical evidence for accurate risk assessment. Combining clinical parameters and immunohistochemical indicators may effectively improve the judgment of tumor biological behavior and prognosis, which is beneficial to guide physician to take more individualized and comprehensive strategies for patients under the same clinical condition to avoid undertreatment.
Retrospective characteristic is one of the shortcomings of this study, and we do not conduct the calculation and justification of the sample size. But we tried to minimize bias through recording the clinical information of all patients inquired from the medical record system in detail. Secondly, unified pathological review fails to be performed in present study and the determination of immunohistochemical expression level may be affected by specimen fixation, detection methods or subjective factors. While what was ensured is that all postoperative specimens were uniformly detected by the corresponding authoritative pathology center according to the standard procedure and the results were evaluated by two qualified professional gynecological pathologists. Then, the current Endometrial Cancer ESMO Clinical Practice Guideline has updated the classification of low-risk patients. Since the patients in this study underwent surgery at a time between January 1, 2013 and April 7, 2022, we classify the patients according to previous criterion which is a limitation of this study. However, the finding of this study is still significant for guidance of low-risk patients. Finally, according to the genomic characterization of endometrial cancer, The Cancer Genome Atlas (TCGA) defined four subgroups related to prognosis: P53-mutant, microsatellite instability (MSI), POLE-mutant and no specific molecular profile (NSMP). 28 The inevitable expensive cost and high requirements for technology and equipment of gene sequencing result in its limited clinical application. So, we classified the patients based on the clinical and immunohistochemical parameters. Further studies on molecular classification were required in future.
Conclusion
In conclusion, this study has demonstrated that the optimal cut-off value of Ki-67 for predicting the recurrence of early low-risk endometrial cancer is 33%, which quantitatively defines the specific value of Ki-67 that causes tumor recurrence. It is critical to assess recurrence risk and guide the formulation of postoperative adjuvant treatment to reduce recurrence of this subgroup patients.
Footnotes
Acknowledgment
Thanks to The First Affiliated Hospital of Chongqing Medical University for providing the data for analysis.
Author’s Notes
Each author has confirmed compliance with the journal’s requirements for authorship. Institution performed study: The west China Second Hospital of Sichuan University and The First Affiliated Hospital of Chongqing Medical University.
Authors’ Contributions
Xue Xiao performed project development, data analysis. Mingzhu Jia conceived the idea, performed project development, data collection and analysis, Manuscript writing. Jiangchuan Pi performed the data collection and data analysis. Juan Zou, Min Feng, Huilin Chen, Changsheng Lin, Shuqi Yang, and P Jiang performed the data collection and investigation. All authors verify and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported financially by National Natural Science Foundation of China: Research on the molecular mechanism of protein kinase complex cdk12/cyclin k regulating self-renewal of stem cells (82071651), Science and Technology Bureau Project of Chengdu: Personalized Precision Immunotherapy for Ovarian Cancer (2017-GH02-00030-HZ), and National Key Research and Development Plan: Research on energy metabolism rule and intervention technology application of different exercise loads in different populations (2022YFC3600304).
Synopsis
We have confirmed that the optimal cut-off value of Ki-67 for predicting the recurrence of early low-risk endometrial cancer is 33%.