
Abstract
Introduction
The Florida-California Cancer Research, Education, and Engagement (CaRE2) Health Equity Center is a triad partnership committed to increasing institutional capacity for cancer disparity research, the diversity of the cancer workforce, and community empowerment. This article provides an overview of the structure, process innovations, and initial outcomes from the first 4 years of the CaRE2 triad partnership.
Methods
CaRE2 serves diverse populations in Florida and California using a “molecule to the community and back” model. We prioritize research on the complex intersection of biological, environmental, and social determinants health, working together with scientific and health disparities communities, sharing expertise across institutions, bidirectional training, and community outreach. Partnership progress and outcomes were assessed using mixed methods and four Program Steering Committee meetings.
Results
Research capacity was increased through development of a Living Repository of 81 cancer model systems from minority patients for novel cancer drug development. CaRE2 funded 15 scientific projects resulting in 38 publications. Workforce diversity entailed supporting 94 cancer trainees (92 URM) and 34 ESIs (32 URM) who coauthored 313 CaRE2-related publications and received 48 grants. Community empowerment was promoted via outreaching to more than 3000 individuals, training 145 community cancer advocates (including 28 Community Scientist Advocates), and publishing 10 community reports. CaRE2 members and trainees together have published 639 articles, received 61 grants, and 57 awards.
Conclusion
The CaRE2 partnership has achieved its initial aims. Infrastructure for translational cancer research was expanded at one partner institution, and cancer disparities research was expanded at the two cancer centers.
We aspire to eliminate cancer health disparities among Blacks and Latinos living in California and Florida, and contribute to paving the way to eliminate disparities in these populations across the US.Significance Statement
Introduction
Black or African American (B/AA) and Hispanic/Latino (H/L) individuals now comprise nearly 33% of the United States (U.S.) population, with a projected minority majority shift by 2045. 1 Unfortunately, significant disparities in cancer incidence, outcomes, research, and biomedical workforce representation exist within these underserved populations. 2 Despite these disparities, there is limited understanding of the complex intersection of biological, environmental, and social determinants of cancer health disparities, considering the genetic makeup, cultural diversity, and various ancestral origins across B/AA and H/L populations. Furthermore, another disparity persists relative to the dearth of highly trained underrepresented minority (URM) cancer researchers, particularly B/AA and H/L scientists.2,3 A well-trained and diverse workforce that leverages multiple perspectives to address the needs of underserved patient populations is vital to reducing these disparities.2-4 Finally, there is often limited engagement and involvement of minority populations and communities in cancer research. To address these needs, we established the Florida-California Cancer Research, Education, and Engagement (CaRE2) Health Equity Center, which was funded as one of the 16 Comprehensive Partnerships to Advance Cancer Health Equity (CPACHE) in September 2018. The purpose of this article is to disseminate to the cancer community key details about our partnership’s structure, process innovations, and initial outcomes of implementing the innovations over the first 4.5 years of the CaRE2 triad partnership.
Materials and Methods
Partners’ Main Scientific Focus
CaRE2 Overall Specific Aims and Benchmarks for Success (2018-2023).
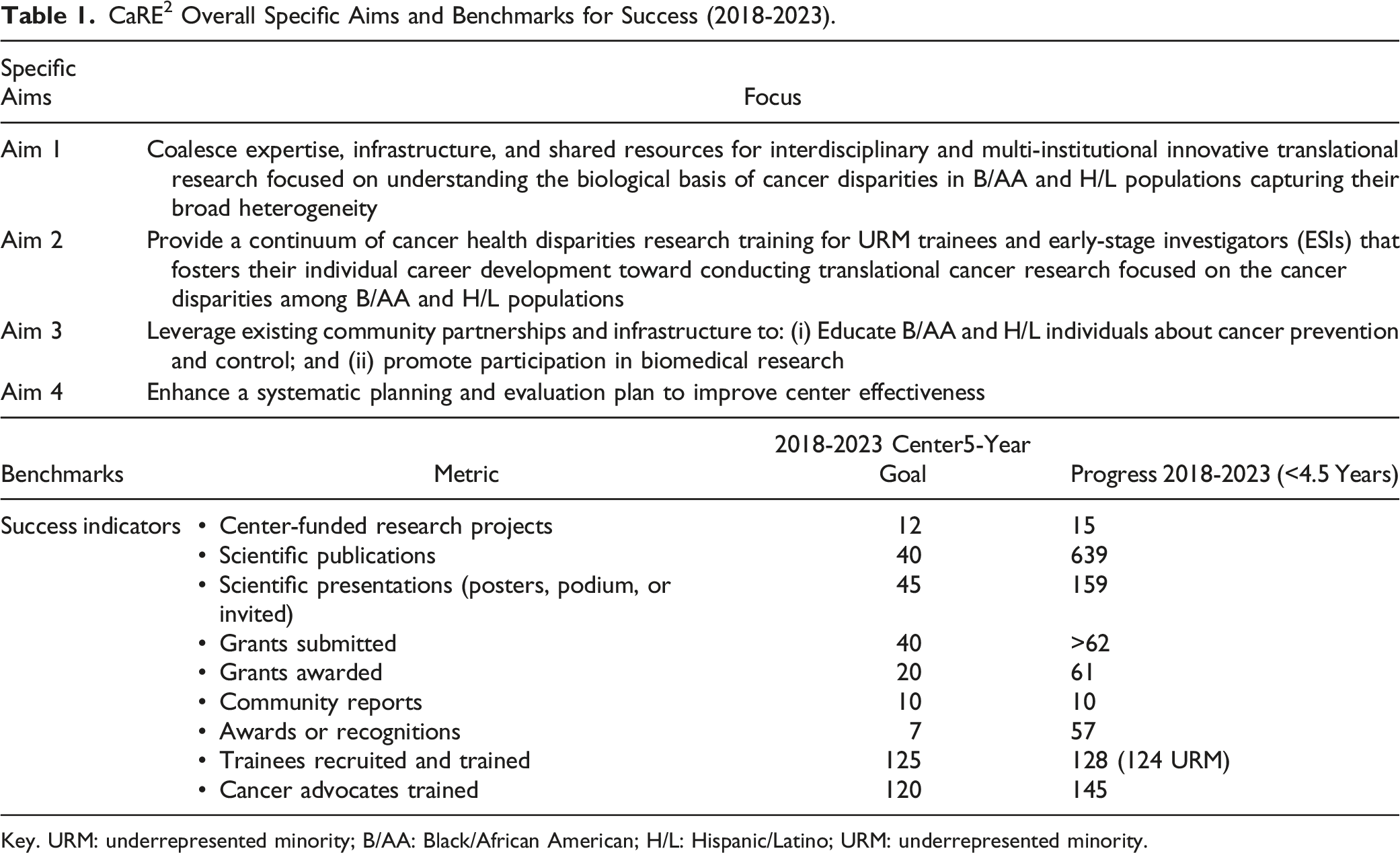
Key. URM: underrepresented minority; B/AA: Black/African American; H/L: Hispanic/Latino; URM: underrepresented minority.
Organizational Structure and Management Overview
The CaRE2 partnership is strengthened by an investigative team with significant experience in cancer disparities research, translational sciences, research training, and community outreach. A team of six Multiple Principal Investigators (MPIs), two from each partner institution direct and administer the CaRE2 partnership (Figure 1). The MPIs form a leadership team of multidisciplinary scientists who are national leaders in cancer health disparities and are supported by an Executive Leadership Committee (ELC), an Internal Advisory Committee (IAC), and a Program Steering Committee (PSC). Top administrators at FAMU, UFHCC, and USC NCCC are committed to providing the Center with a strong foundation. Leadership and oversight for the CaRE2 Center is structured to maximize strong academic and community partnerships, effective communications among all groups, compliance with all policies and procedures, scientific excellence, training scholarship, research education, mentoring, community-centered outreach, effective monitoring, and continuous quality improvement (CQI). In addition, the leadership team collaborates with three CaRE2 administrators, one at each institution, who help to administer and coordinate networking activities at each institution. CaRE2 Health Equity Center: Structure and Initial Outcomes.
The MPIs established an innovative approach for sharing leadership responsibilities. The primary administrative responsibilities rotate on a 4-month schedule among the partners: UF leads Sept–Dec, USC leads Jan–April, and FAMU leads May–Aug. During the leadership trimester, the lead partner assumes responsibility for official Center-related communication with the NCI Program Officer, PSC, IAC, and ELC as well as organizing the meetings and functions occurring during the trimester (e.g., partnership meetings, PSC meeting, annual report). This delineation of responsibility minimizes the chance that key administrative tasks could be missed and threatens the success of the partnership.
Figure 1 also displays the organizational structure of the Center’s four cores, two shared resources, and six research projects. A highly innovative feature of the CaRE2 organization structure is that each component includes principal investigators from each of the three partnering institutions, including all cores, shared resources, and projects, each with equal responsibility and voice. The CaRE2 partnership cores are highly integrated into the research platform to support the overall center mission in a synergistic manner (Figure 2). At the center of our partnership are highly collaborative and innovative translational cancer research projects supported by our cores and shared resources, whose overall structure is summarized in the following section. Interaction across the CaRE2 center components.
Description of Cores, Shared Resources, and Research Projects
The
The
The
The
The two
The Research Projects include two full research projects and one pilot research project funded in 2018 and three additional pilot research projects funded in 2021. Additionally, we supported other projects (supplements or developmental research program projects that were funded with institutional leverage funding). Two of the Administrative Supplements focused on COVID-19 research and outreach activities to improve our understanding of and to reduce the impact of the pandemic among B/AA and H/L communities. An innovative feature of the CaRE2 organizational structure is that we foster team science by requiring each full and pilot project to include a PI from each institution who has responsibility for specific aspects of the project specific aims. An important expectation of this team science model is that publications and future grants emanating from the project will include all three investigators. This organization model is specifically designed to reduce silos in translational cancer research to promote optimal sharing and translation of knowledge, skills, and technology to rapidly move cancer health disparities research forward.
Innovations
The CaRE2 Center contributes to the CPACHE program by addressing gaps in knowledge and novel translational cancer disparities research in racially and ethnically diverse bicoastal populations of B/AA and H/L individuals in Florida and California. Our partnership provides a diverse academic platform to study and better understand cancer disparities in B/AA and H/L from coast to coast. Our multi-disciplinary program and aligned resources allow us to plan and conduct innovative research in cancer health disparities covering the spectrum from the molecular underpinnings of cancer health disparities to clinic-based and community-based interventions that will help improve outcomes among minority populations. In addition to the innovations previously described, four key innovative features of CaRE2 Center are: 1. 2. 3. 4.
Results
Like other research teams around the world, the COVID-19 pandemic, which began approximately 6 months into Year 2 of our grant cycle, posed challenges and lead to innovative approaches. Restrictions imposed by the pandemic prevented face-to-face meetings, inter-institutional visits by trainees, and clinical activities such as collecting specimens for our partnership research projects. Restrictions also delayed laboratory-based translational research studies and prematurely ended important experiments with mandated euthanasia of animals as labs closed urgently. After the COVID-19 crisis period, the phenomenon of the great migration led to the transition of several key personnel to prestigious positions at other organizations. Although we were proud that our Center work facilitated our colleagues to obtain important career advancements, CaRE2 teams required reconfiguration and reformed relationships and work plans to achieve aims. Hiring into vacated positions required more time than usual as the bicoastal communities emerged from the pandemic and caused at times the workload to be unevenly distributed. Despite the hinderance to our work, the pandemic also challenged the teams to deploy technologies such as Zoom not only for collaboration but for offering training and community outreach. We learned that trainees and community members were able to engage in activities, socialize, and complete impressive projects via Zoom and other social media platforms. Despite these challenges, and as described in the results section shows, our partnership achieved our aims for 2018–2023.
Accomplishments: Scientific Projects and Cores
Scientific Projects
To date, our partnership has funded 15 translational cancer disparities research projects, which include 2 Full Projects, 4 Pilot Projects, 3 Administrative Supplements, 1 Diversity Supplement, and 5 Developmental Research Projects. Altogether, our Center has contributed to more than 639 publications, with 38 directly resulting from our funded projects, 313 from CaRE2 trainees and ESIs, and more than 288 from the CaRE2 members’ individual research programs that were relevant to cancer health disparities. CaRE2 members and trainees received 61 grants directly related to Center work. Table 1 shows a summary of the benchmark metrics.
Project 1
The study provided new discoveries of mitochondrial peptides overexpressed in PCA and in Black individuals. Major findings included the identification of novel Mitochondrial Derived Peptides, which are derived from ORFs that are differentially expressed in PCA from B/AA men and in response to androgens. The impact of these studies and discoveries is new knowledge for molecular determinants of PCA disparities. Four undergraduate students were trained as part of this research project, including students from FAMU who traveled to USC with Dr Reams for 2 weeks, and received a bioinformatics bootcamp and practical laboratory experiences in Drs. Cohen’s and Carpten’s laboratories. As a follow-up, Drs. Carpten, Salhia and Reams are collaborating on a new study using single-cell Multiome (RNA-seq and ATAC-seq) assays on frozen prostate specimens from B/AA and White patients.
Project 2
Whole exome sequencing of tumor and uninvolved tissue from a series of B/AA, H/L, and NHW PDAC patients has revealed local ancestry patterns across B/AA, H/L, and NHW patients (Figure 3) and somatic mutation frequencies for comparison with other datasets (i.e., TCGA). The study has also led to the development and synthesis of novel nanoparticle coated Gemcitabine analogs (GemEnps) by FAMU ESI Dr Agyare, which were tested on novel patient derived primary PDAC organoid cell models by Dr Han and xenografts (PDX) models derived from B/AA and NHW patients.12,13 Self-identified race and ancestry of patients with pancreatic cancer.
Pilot Project 1
Using human pancreata of healthy donors obtained from pancreatic islet procurement centers, the team established the methodology to conduct sequencing of donor’s RNA from pancreatic cultures on matrigel using samples from B/AA, H/L, and NHW individuals. Using RNA sequencing they identified 10 transcriptional drivers of ADM and using genome-wide association data from the Multiethnic cohort study, they identified associations between Ptf1a and Rbpjl SNPs and pancreas cancer risk. Of significant impact is that two URM students, Alyssa Gosling (UF postbac) and Corey Perkins (UF graduate student) participated in this project, with one being a manuscript coauthor (Corey Perkins). 14 Finally, Dr Fredenburg is a URM ESI Pathologist at UF who obtained a diversity supplement related to this work with mentoring by Dr Schmittgen. The preliminary results of her study assessing the role of microRNAs in head and neck cancer disparities set the stage for her receiving a Department of Defense (DoD) Career Development Award in 2022. Impactfully, Dr Fredenburg mentored 3 CaRE2 postbacs who are coauthors on abstracts and manuscripts and received awards. Several publications emerged from this study that are published.14-18
Pilot Project 2
This team is collaborating with a DoD grant (Rhie, PI) to expand the assessment of epigenomic alterations in PCA, showing early synergy among this research team. Dr Falzarano, a pathologist at UF, has identified and reviewed the tissues and methylation assessment is underway with completion planned by mid-2023. Postbac and URM students involved in this project have presented at a national cancer conference. Several publications including research and review papers are in preparation.
Pilot Project 3
This team has successfully immortalized human alveolar epithelial cells and generated monoclonal cell lines; developed a gene editing strategy to replace KRAS G12 C in B/AA LUAD cell lines; designed a lung 3-D bioprinted model for drug testing; tested PCAIs and conducted functional analyses of these treated cells showing p-AKT levels are stimulated after treatment. Impactfully, several CaRE2 URM postbacs are working on this project in each of the three laboratories. All three postbacs submitted abstracts and attended national cancer conferences, and all three received Minority Scholar in Cancer Research travel awards. Several publications that include postbac trainees are in preparation.
Pilot Project 4
To date, the team has analyzed genomic data obtained from 20 B/AA and 20 H/L pancreatic cancer patients; established 8 pairs of 3D organoid models with defined ECM and mechanical properties to mimic stroma from B/AA and NHW patients; synthesized 6 chemo drug analogs; established toolbox for drug and drug combination test. Dr Rogers who is an URM ESI Medical Oncologist and received a career development award, provides critical translational and clinical insights about the research. Importantly, Dr Rogers trained a URM postbac, Guettchina Telisnor, who performed research and published a review manuscript on pancreatic cancer disparities. 19
Cores
Despite the challenges imposed by the COVID-19 pandemic,
Following are a variety of comments from our trainees. One CaRE2 trainee reported that his mentor was “encouraging, resourceful, helpful and [showed] patience” while indicating that he would like “more community outreach days.” Another trainee commented about our health disparities training, “The graduate certificate was extremely vital to my experience as a post baccalaureate fellow. I think it coupled well with the research projects that I have been part of and will help in my matriculation as a medical student and clinician. One postbac stated “I want to thank the CaRE2 team for their help with my research, especially my mentor, Ite Offringa. Dr Offringa has been the most incredible mentor a student could ask for due to our shared enthusiasm for innovation. In addition, I want to thank my colleagues from the CaRE2 Health Equity Center for their unconditional support in my development as a scientist.” Another postbac stated “The CaRE2 program broadened my understanding regarding the importance of collaboration in cancer disparities research” and “I have grown in more ways than I can imagine in one year. I have improved as a writer, a collaborator, [and as] a leader from my experience in this program. I am also immensely grateful that I will be supported to attend AACR and present my projects.”
Guided by the Community Advisory Board’s feedback, the • recruited 200 B/AA or H/L to a research contact registry facilitating research and clinical trial participation; • reached out to and educated o ∼ 750 people about prostate health care awareness, information on how to screen, treat, and live with prostate cancer through six ProTalk Facebook Live events and visiting more than 20 barbershops in person; o 225 individuals via virtual/in-person events about awareness, knowledge, and testing for PCA among B/AA men; o more than 3000 people through social media channels and our website, • published and distributed 10 community reports, which are also available on our website (https://care2healthequitycenter.org/cancer-information-and-education-materials/), • adapted a Toolkit and developed another, and • presented at national conferences, with publications in preparation. COC community members have commented about their experiences during several of the above activities:
Community Scientist Research Advocates commented, “Great program, I loved the diversity of backgrounds and education levels throughout the groups” “When I signed up for CaRE2 I wasn't quite sure what to expect, or if I would even get selected to participate, but now I am so grateful for the opportunity it presented my fellow group members, and myself to learn about how Community Advocacy works.” “I think the program is great and afforded me the opportunity to expand” Other community members stated that they signed up to be on the CaRE2 Contact Registry because “I wanted to be informed and educated on Cancer studies and how to best prevent or fight this disease.” “I like to stay informed and help others.” “My opinion matters.” “I want to help improve the health of my community, future generations, and self.” Finally, a community member who participated in the CaRE2 Connects with Our Community stated that it “Helped to continue connecting and highlighting the important and impactful work being done by CaRE2 researchers, physicians and administrators.”
Guided by feedback the CaRE2 coauthor network analysis (A) 2018-2019, (B) 20208-2019, (C) 2022 (9 months).
The
The
Discussion
We have successfully managed the bicoastal distance and time difference between Florida and California with an effective model of face-to-face meetings during scientific national conferences and biweekly/monthly meetings via Zoom, which allowed us to communicate regularly and productively. We have fostered and facilitated innovative translational research that addresses cancer disparities from the molecular to the societal level and back. Our research has been conducted by a cadre of racially and ethnically diverse, well-trained URM scientists in partnership with consumer advocates (cancer survivors and advocates) and prioritized on cancers for which disparities have been documented or are understudied among B/AA and H/L populations. We have built novel and innovative research platforms and infrastructure at FAMU, the partnership ISUPS. The accomplishments related to these activities included the growth and expansion of a Living Biorepository with patient-derived cancer models from underrepresented patients for the development and testing of novel drugs created by FAMU investigators, as well as transfer of technology on cancer-model development through organoid and PDX training. We advanced, supported, and tracked the careers of URM trainees: namely postbac, graduate, postdoc, and ESIs. Of specific priority is fostering the acquisition of competitive independent research grants (R-type or equivalent) for URM ESIs, especially scientists at FAMU. We developed innovative approaches to deliver cancer research knowledge using culturally appropriate and multimedia approaches, build a workforce of trained cancer advocates, including community scientists, and train URM scientists who can engage in bi-directional community engagement.
We leveraged additional partnership opportunities within our triad partnership as well as with other CPACHE partnerships. An unexpected opportunity occurred due to the impact of the COVID-19 pandemic and was possible given the existing trust that we had built over the years with our community partners, which allowed us to quickly pivot to address the COVID-19 pandemic in our catchment communities. Specifically, we fostered their participation in COVID-19 vaccine clinical trials and the uptake of the COVID-19 vaccine among the B/AA and H/L populations with funding from an NIH CEAL Award led through UFHCC and an administrative supplement led through USC.
Moving forward, we will continue to expand collaborations to understand further the biological and environmental etiology of cancer disparities by expanding our focus to migration studies and global cancer health studies including B/AA and H/L populations outside the U.S. We have built strong collaborations with partners in Africa to explore the molecular features of prostate cancer in men from West Africa using transcriptome sequencing. This collaboration has led to supplemental funding from the NCI Center to Reduce Cancer Health Disparities (CRCHD) and NCI Center for Global Health.
We are also seeking novel collaborations with other entities, including other CPACHE partnerships, to synergize our efforts and effectively address cancer disparities nationally. For example, we will collaborate with Tempus, a company with molecular sequencing data from over 100,000 individuals, including many B/AA and H/L patients, to analyze the genomic features of cancers of interest for our partnership to validate our research findings. We will continue to seek other collaborative opportunities to expand the impact of our partnership.
Despite the many successes during the first funding cycle of the CaRE2 Health Equity Center, several limitations merit consideration. First, the laboratory-based research projects’ progress was slowed by the COVID-19 pandemic and publications for several aims are still in process. Second, there have been a large number of the Center’s investigators who transitioned to important positions at other institutions, which necessitated reconfiguration of teams and development and implementation of succession plans. The impact of these transitions would have been more disruptive to the Center’s work had our structure been less robust. Third, the Center’s initial focus was on integration across the three institutions with insufficient attention to integration within the center’s cores and projects as they worked to achieve their aims. Fourth, our initial trainee tracking processes were not as robust as needed for long-term tracking. Finally, with our laser focus on the big picture—our a priori established benchmarks of success—we missed opportunities to strengthen our evaluation of Center processes and other metrics that indicated successful achievement of all core and project aims. Identification of these limitations provides opportunities to strengthen the center as it moves toward sustainability.
Conclusion
Since its establishment in 2018, the CaRE2 Health Equity Center has established a structure and innovative processes enabling achievement of its foundational benchmarks. These initial outcomes are likely a function of the commitment of our investigators who embraced the team science model while they also encouraged and supported trainees to publish existing and new data and apply for grants to launch their scientific careers. Through our community outreach and bidirectional input, we have empowered our communities to understand, participate in, and advocate for cancer research. These efforts have created expanded infrastructure for translational cancer research at FAMU and cancer disparities research at the UFHCC and USC NCCC. Greater impact is expected in the future as the CaRE2 continues to mature and innovate.
Footnotes
Acknowledgements
We thank our NCI Program Officers, LeeAnn Bailey PhD, Branch Chief of the Integrated Networks Branch and Whitney (Barfield) Steward, Program Director for their thoughtful guidance regarding programmatic actions. We are grateful to our Community Advisory Board and community health educators for their tireless efforts to eliminate cancer health disparities and to Amelia Greenlee for her support of our work. For their constant advice and critical review of our program, we thank our Program Steering Committee members: Clayton Yates, PhD (Chair), Zhenbang Chen, PhD, Antonio Baines, PhD, Laura Fejerman, PhD, Virgil Simons, Robert Winn, MD, Camille Ragin, PhD, and Mary Scroggins.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by Grant Numbers U54CA233396, U54CA233444, U54CA233465 from the National Institutes of Health (NIH), National Cancer Institute (NCI). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NCI. The final peer-reviewed manuscript is subject to the National Institutes of Health Public Access Policy.