
Abstract
Objective
Racial disparities among women with cervical cancer have been reported but are understudied in Caribbean immigrants. The objective of this study is to describe the disparities in clinical presentation and outcomes between Caribbean-born (CB) and US-born (USB) women with cervical cancer by race and nativity.
Methods
An analysis of the Florida Cancer Data Service (FCDS), the statewide cancer registry, was performed to identify women diagnosed with invasive cervical cancer between 1981 and 2016. Women were classified as USB White or Black and CB White or Black. Clinical data were abstracted. Analyses were done using chi square, ANOVA, Kaplan-Meier and Cox proportional hazards models, with significance set at P < .05.
Results
14 932 women were included in the analysis. USB Black women had the lowest mean age at diagnosis, while CB Black women were diagnosed at later stages of disease. USB White women and CB White women had better OS (median OS 70.4 and 71.5 months, respectively) than USB Black and CB Black women (median OS 42.4 and 63.8 months, respectively) (P < .0001). In multivariable analysis, relative to USB Black women, CB Blacks (HR .67, CI .54–.83), and CB White (HR .66, CI .55–.79) had better odds of OS. White race among USB women was not significantly associated with improved survival (P = .087).
Conclusion
Race alone is not a determinant of cancer mortality in women with cervical cancer. Understanding the impact of nativity on cancer outcomes is crucial to improve health outcomes.
Keywords
Introduction
Cervical cancer is the third most common gynecologic cancer in the U.S. and one of the leading causes of death among women worldwide.1-3 In 2023, it is estimated that 13,960 new cases of invasive cervical cancer will be diagnosed, and approximately 4,310 women will die from cervical cancer in the U.S.3-5 Florida has one of the highest incidences of cervical cancer in the country6,7 and an estimated incidence of 1200 cases for 2023. 5 While screening interventions have lowered the incidence of cervical cancer overall, Black and Hispanic women in the U.S. continue to be disproportionately affected by cervical cancer incidence and mortality. 8 Black women specifically are more likely to have cervical cancer diagnosed at a higher stage and less likely to receive optimal treatment. 9
Currently, there are over 4 million Caribbean-born (CB) immigrants living in the United States. 10 The vast majority migrate from Cuba (29.7%), Dominican Republic (26.3%), Jamaica (16.9%), and Haiti (15.4%). In the state of Florida, 76% of foreign-born individuals migrate from Latin America and the Caribbean and comprise 21% of the population. 11 Given Florida’s diversity, assessment of health outcomes by not only race, but also Caribbean nativity, is feasible, and may suggest health disparities in subpopulations that may otherwise be masked if evaluated by race alone. The objective of this study was to examine the differences in cervical cancer outcomes between CB and US-born (USB) women within and across race and nativity.
Methods
Data Sources
The Florida Cancer Data System (FCDS) database is a state cancer registry that gathers information from 230 hospitals; all cancer cases are required to be reported to the FCDS by legislative mandate. Data is reported to FCDS following the North American Association of Central Cancer Registries (NAACCR) guidelines and data dictionary v22 12 (Supplementary Table S1). The study was completed under a state-approved institutional review board (IRB) for coding and abstraction of the data.
Study Cohort
We selected all cervical cancer cases identified with the ICD-O-3 codes C53.0, C53.1, C53.8, and C53.9 diagnosed between January 1st, 1981 and December 31st, 2016 (latest available data points in FCDS to date). Self-identified Black or White women were included if they were born in a country in the Caribbean (Bahamas, Cuba, Dominica, Dominican Republic, Guyana, Haiti, Jamaica, Trinidad and Tobago, and the US Virgin Islands; other countries in the Caribbean were not reported given the absence of datapoints in FCDS) or the United States. We excluded cases of non-invasive cancer.
Data Collection
Captured variables included race, country of birth, age at diagnosis, date of diagnosis, date of death of last follow-up, vital status, stage of disease, type of insurance, tumor grade, tumor histology, lymph vascular invasion, tobacco use, date of first treatment and receipt of chemotherapy, radiation therapy or surgery. The variables race and country of birth were combined to generate 4 categories: USB White women, USB Black women, CB White women, and CB Black women. Stage of disease was categorized as reported in FCDS following NAACCR guidelines: localized, regional, and distant (FIGO stage is not available in FCDS); type of insurance, as private, Medicare only, Medicaid only, other insurance (which included having both Medicare and Medicaid) and No insurance. Tumor grades were grouped as I–II and III–IV. Tumor histology was classified following a previous study 13 which characterized tumors as either squamous carcinoma or non-squamous carcinoma (List of histologic subtype codes provided in Supplementary Table S2). Lymph vascular invasion was binary (Yes/No). The dates of the first chemotherapy, radiation therapy, and surgery were used as a proxy to code for receipt of chemotherapy, radiation therapy or surgery respectively (Yes/No). Further details regarding treatment modality (ie, type of chemotherapy or simple vs radical hysterectomy) was not available. Tobacco use was classified as never or ever smoker. Time to treatment was defined as time from date of diagnosis to date of first treatment in weeks. Overall survival (OS) was defined as time from date of diagnosis to all-cause death or last follow-up in months corresponding to vital status (death/alive, respectively). Cancer specific death is not available in FCDS. Patients had follow-up censored at the date of last contact. A complete list of variables available in FCDS and all collapsed categories used in this study is available in Supplementary Table S1.
Statistical Analysis
All available data were included in the analyses, even when individual patient data was missing. Chi square was used to assess associations between categorical variables and groups defined by race and country of birth. The analysis of variance (ANOVA) and the Kruskal–Wallis tests were used to assess differences in continuous variables among race and country of birth groups. OS was estimated by the Kaplan–Meier method. Comparison between survival curves of combined race and country of birth categories were assessed by the log-rank test for all stages, broken down by each stage category and for all other explanatory variables. Univariable and multivariable Cox proportional hazards regression analyses were carried out to assess effect of explanatory variables on OS. The multivariable model was adjusted for race/country of birth, stage of disease, age at diagnosis, type of insurance, tumor grade, tumor histology, receipt of chemotherapy, radiation therapy and surgery. Results were reported as hazard ratios (HR) with 95% confidence intervals (95% CI). All tests were two-sided, with statistical significance set at P < .05. Statistical analysis was performed using the SAS software 9.4 (SAS Institute Inc., Cary, NC, USA) and R software 4.2.
Results
A total of 58,515 women were diagnosed with cervical cancer between 1981 and 2016 in the state of Florida (Figure 1). Of these women, 14,932 met the inclusion criteria for this study. 12,569 women were born in the United States and 2,363 were born in the Caribbean. Table 1 demonstrates the clinical and demographic characteristics of each group. The mean age at diagnosis was lowest in USB Black women at 50.6 years in comparison to other cohorts, P < .0001. CB Black women were diagnosed at later stages of disease and, as with USB Black women, had higher grade disease at diagnosis. The rate of squamous cell carcinoma was similar between USB and CB Black women (75.1% and 76.3% respectively), while USB and CBB White women had lower rates of squamous cell histology relative to Black women (64% and 67% respectively, P < .0001). USB White and CB White women had the lowest rates of distant disease at diagnosis (14.1% and 14.4%, respectively) in comparison to USB and CB Black women (16.4% and 17.4%, P < .0001). CB Black women had the highest median time to treatment, lower rates of surgical intervention, and higher rates of chemotherapy among the 4 groups (P < .0001). CB women were less likely to be insured and had a higher median time to treatment than USB women. The highest percentage of uninsured women was among CB Black women. USB White women had the highest proportion of smokers (53.9%). There was a statistically significant difference in lymphovascular space invasion among subgroups, with White patients more frequently demonstrating this pathologic finding (USB Black women 23.3% vs CB Black women 25.8% vs USB White women 32.3% vs CB White women 36.1%, P = .0342). Flow diagram. Clinical and demographic characteristics of study cohort (N = 14 932). *Caribbean born includes Bahamas (60), Cuba (1324), Dominica (1), Dominican Republic (99), Guyana (15), Haiti (593), Jamaica (254), Trinidad (4), US Virgin Islands (13) White Caribbean includes Bahamas (7), Cuba (1291), Dominican Republic (82), Guyana (7), Haiti (8), Jamaica (17), Trinidad (1), US Virgin Islands (3) Black Caribbean includes Bahamas (53), Cuba (33), Dominica (1), Dominican Republic (17), Guyana (8), Haiti (585), Jamaica (237), Trinidad (3), US Virgin Islands (10). **Unstaged/Unknown categories were excluded from analysis. +ANOVA: Same letter (a,b,c,d,e) indicates differences in groups. †Kruskal-Wallis Test: Same letter (a,b,c,d,e) indicates differences in groups.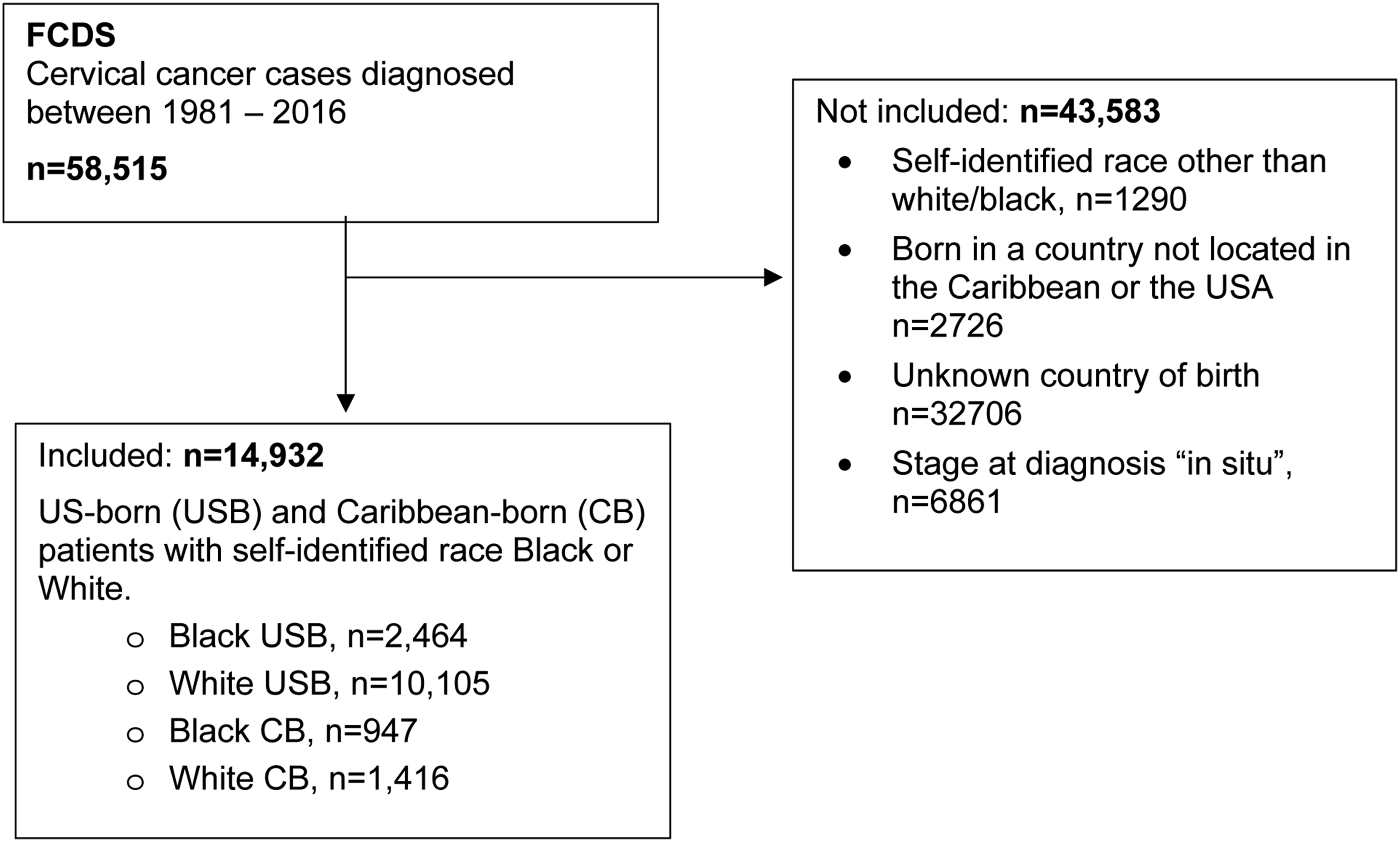

USB White women and CB White women had better OS (median OS 70.4 months [95% CI 65.5–75.6] and 71.5 months [95% CI 61.7–87.9], respectively) than USB Black and CB Black women (median OS 42.4 months [95% CI 37.7–47.7] and 63.8 months [95% CI [48.3–76.8], respectively) (P < .0001, Figure 2(A)). When stage was localized, relative to USB Black women (median OS 111 months [95% CI 92.9–128]), USB White women (median OS 169 months [95% CI 160.7–179]) and CB White women (median OS 193 months [95% CI 171.4–232)] had longer OS (P < .0001), Figure 2(B)). In regional disease, CB White women (median OS 53.3 months [95% CI 42.9–62.3]) and CB Black women (median OS 49.3 months [95% CI 38–71.8]) had a better OS compared to USB Black women (median OS 36.2 months [95% CI 31.6–44.3] (P = .04, Figure 2(C)). In distant disease, CB Black women (median OS 17.7 months [95% CI 13.7–24.7]) and CB White women (median OS 14.2 months [95% CI 12.3–20.2]) had better OS compared to USB Black women (median OS 10.2 months [95% CI 8.7–11.4]) (P = .0009, Figure 2(D)). Overall survival by other explanatory variables is included in Supplementary Figure S3. Overall survival by race and place of birth in all stages (A), and in localized (B), regional (C), and distant (D) stages.
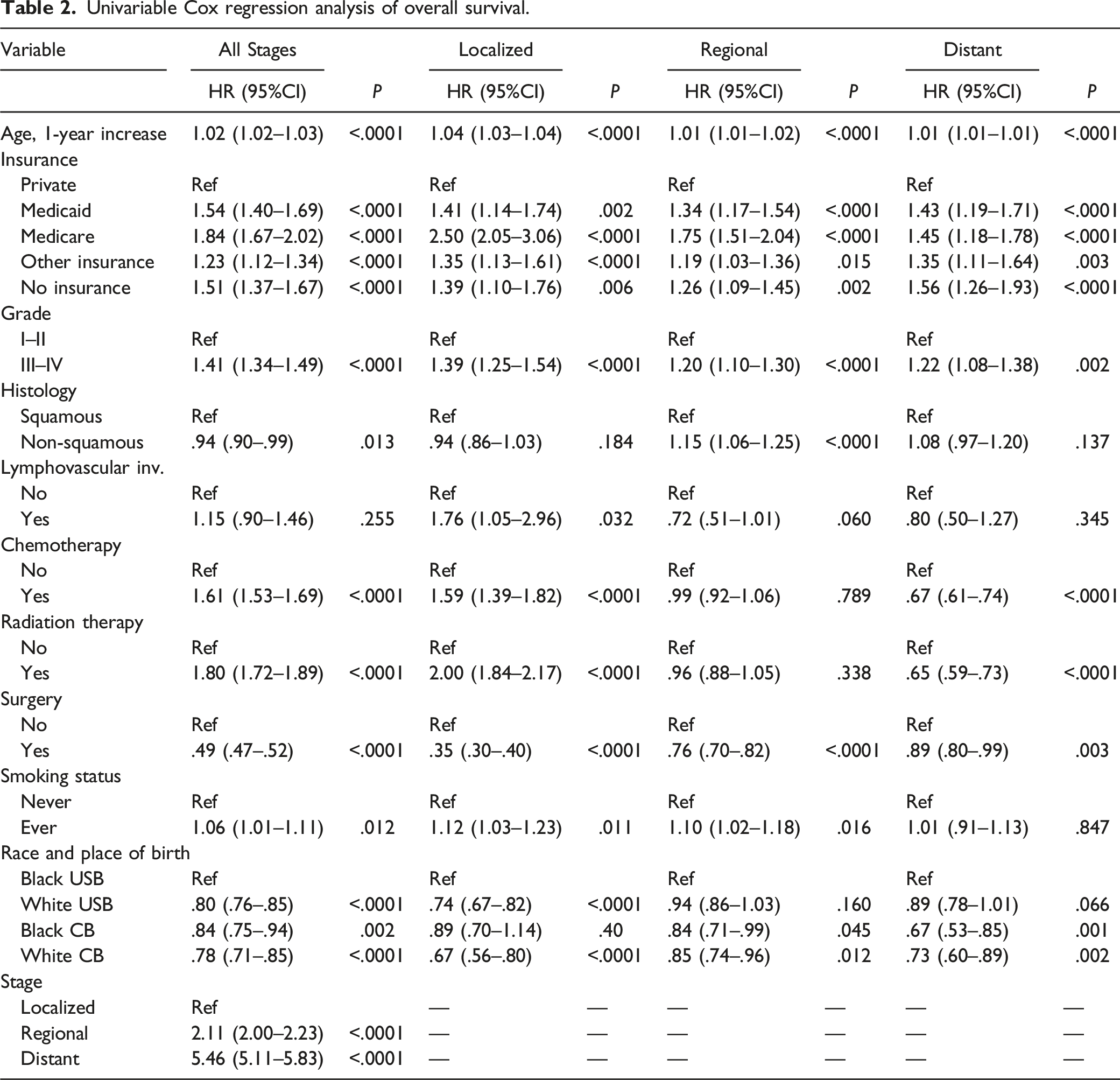
Univariable Cox regression analysis of overall survival.
Multivariable Cox regression analysis of overall survival.

Discussion
Summary of Main Results
Our data illustrate that differences in cervical cancer outcomes exist between Black and White women based on Caribbean nativity. Although USB White had better OS, CB women had better outcomes in distant disease. Black women born in the U.S. had the lowest OS survival in comparison to all racial groups, which is consistent with national data. 9 These reports, however, have not previously considered differences in subpopulations by nativity.
Results in the Context of Published Literature
Our findings are consistent with previous studies examining cancer outcomes among immigrants.14,15 Pinheiro et al 14 demonstrated that individuals from Haiti and Jamaica living in Florida have lower rates of mortality in comparison to the USB Black population for most cancers. Moreover, the cervical cancer mortality rate was higher in USB Black women in Florida (4.4/100,000) relative to the national average for Black women (3.4/100,000).1,14 Cervical cancer mortality rates, specifically among Haitian and Jamaican immigrants, were lower in these groups in comparison to USB Black women in Florida. Among women with breast cancer, CB patients with breast cancer were diagnosed at more advanced stages of disease (44.2% vs 35.2%, P = .016), were more likely to have ER/PR-positive breast cancer and undergo chemotherapy and radiation when compared with USB Black women. 16 Nonetheless, CB women showed a better overall survival (HR = .75; 95% CI .59–.96; P = .024) in comparison to USB Black women.
Differences in survival by nativity have been previously identified among subpopulations of women with other gynecologic cancers.17,18 Schlumbrecht et al reported that among CB women treated for ovarian cancer, Hispanic ethnicity is significantly associated with improved survival outcomes, regardless of race. 17 Additionally, among a cohort of women diagnosed with endometrial cancer, Caribbean immigrants had a higher prevalence of high-grade endometrial cancers. 18 Although high-grade histology was found to be predictive of worse survival in this study, Caribbean nativity was associated with a better OS, HR .65 (.40–1.07), although not statistically significant.
One of the most noteworthy findings in this study is the variation in OS by Caribbean nativity in advanced cervical cancer. The CB Black women were diagnosed at later stages of disease in comparison to all other racial groups. CB Black women also had lower rates of surgical intervention and higher rates of chemotherapy among the 4 groups (P < .0001). Surgical intervention is primarily used as a modality of treatment for early stages of disease. Therefore, the lower rates of surgical intervention and higher rates of chemotherapy in this population are likely reflective of later stages at diagnosis. Similarly, in our univariable and multivariable analyses adjuvant therapy with chemo/radiation were associated with increased mortality. However, we believe that this correlation, once again, is secondary to late stages of disease at diagnosis, as opposed to the treatment modality. Additionally, distant disease at diagnosis was associated with worse overall survival, yet CB Black women had better survival outcomes than both USB Black and White women with advanced cervical cancer. Studies have shown that foreign-born individuals are less likely to participate in cancer screening.19,20 CB immigrants are also more likely to be publicly insured in comparison to other immigrant groups. 9 Furthermore, CB women have been shown to have less knowledge regarding HPV, cervical cancer screening, and HPV vaccination.21-24 This would explain our findings showing that CB Black women were diagnosed at later stages of disease. Additionally, cervical cancer rates in Caribbean countries are much higher than rates in the US.1,14 Nonetheless, immigrant men and women have up to an 18% and 13% lower risk of all-cause mortality, respectively, than their USB counterparts. 25 Differences in access to care may explain this finding. Immigrant populations tend to live in the inner city with access to large health centers. In contrast, the White rural population may lack of access. More information would be needed to assess these findings.
Several explanations account for differences noted across stage at diagnosis. The first is the Healthy Immigrant Effect (HIE) which posits that immigrants to the U.S. are healthier than the USB population and represent a healthier subset of migrants than those who remain in their native country.20,26,27 This may be pronounced among recent and younger immigrants. 27 Additionally, contributing factors for these differences may be due to healthier lifestyles and practices before and immediately after migration, as well as baseline protective factors inherent to their countries of origin. Culturally based protections such as social, familial support and strong religious beliefs have also been proposed as a contributing factor. These influences remain persistent in reducing the risk of disease, and resistant to the negative effects of acculturation, as has been shown among Hispanics. 27 Furthermore, immigrants also tend to reside in urban areas, which may increase their access to large hospital centers, as opposed to those who residing in rural areas. Interestingly, the HIE phenomenon among US immigrants appears to wane within 10–15 years of arrival, and their health outcomes begin to reflect that of their native-born counterparts. 27
Across various health outcomes, the nativity gap has been shown to be most prominent among Blacks. 26 Differences in life experiences and social structures may account for some of the differences. Chronic exposure to racial prejudice and discrimination has been suggested to trigger adaptational responses that to chronic “wear and tear,” leading to increased health risk in USB Black women. 28 Though CB Blacks may also experience racial discrimination in their native countries to a degree, internalized racism is less distressing for foreign-born Caribbean Black in comparison to USB Blacks P = .013. 29 Social support networks may also vary in CB born populations. Among CB individuals close friends in addition to extended familial support has been shown to be an essential part of survival upon arrival to the U.S.25,30 CB rely only on this network to gain entry into the U.S., access employment and housing opportunities, and maintain close ties with their ethnic communities post-migration.25,30
Implications for Practice and Future Research
Variations in HPV prevalence by subtype exist across countries in the Caribbean and Africa.31,32 While HPV subtypes 16/18 cause most cervical cancers in the US, higher rates of non-16/18 HR-HPV infections are found in women of Caribbean origin. 32 Countries such as Jamaica and Tobago have a higher prevalence of HPV-45 and -52, respectively. 32 Furthermore, HPV distribution in Curaçao showed a lower prevalence of HPV-16 in women with invasive cancer (38.5%), CIN III (46.3%), and CIN II (30.8) (30), 33 in comparison to prevalence reported in the literature. Smith et al demonstrated that the prevalence HPV-16/18 in women with cervical cancer was higher in Europe, North American and Australia (74–77%) in comparison to Africa, Asia, South/Central America (67–70%). 34 Moreover, HPV-16 was significantly under-represented in adenocarcinoma (33%) compared with squamous cell carcinoma (55%). Conversely, HPV-18 was significantly over-represented in adenocarcinoma (37%) in comparison to squamous cell carcinoma (13%). 35 When examining patient outcomes by HPV subtype, among women whose tumors test positive for HPV-18, there was a lower rate of survival (HR 2.59, CI 1.08–6.22). 36 Our data showed a difference in histology by race, and not nativity; however data regarding HPV subtypes was not available. The implication of HPV genotypes on the incidence and outcomes of cervical cancer in the Caribbean vs U.S.-born women remains unknown and warrants further investigation.
Strengths and Limitations
Strengths of this study are that we analyzed results from a large statewide dataset of the representative of Florida. Also, the women in this dataset represent a wide variety of countries in the Caribbean who currently reside in the U.S. The Caribbean immigrant population in Florida is also reflective of the percentage of Caribbean immigrants in the general U.S. population, with most immigrants coming from Cuba, Haiti and Jamaica. Even though many women were excluded for missing data on country of origin, the remaining cohort was still robust. Also, this study not only highlights heterogeneity among the Black population, but also shows differences in the White populations in the United States, particularly White Hispanics. Current trends predict that 1 in 5 Americans with be foreign-born by 2050. 37 As the non-Hispanic White population will be less than 50%, the Hispanic populations are projected to significantly increase. 37
Our study is limited in that the analyses were conducted on a single dataset representative of outcomes only for the state of Florida which may not be applicable elsewhere in the country. Also, individual level and group level risk factors were not entirely captured from this dataset. Uncaptured data which would be relevant include specifics about treatment modality, duration and compliance. Also, this analysis does not include Black women born in other regions (ie, African immigrants), who also contribute a significant portion of the Black immigrant population in the U.S. While we recognize these limitations, we also want to highlight that Florida’s diversity allows us to assess cervical cancer outcomes based on nativity and not race, with the goal to improve outcomes in a diverse population.
Conclusion
Among a diverse population of women with cervical cancer, race alone was not a determinant of cancer mortality. Historically, all Black individuals were categorized into one group however important determinants of disease in Black subpopulations may be masked. Our data underscore the importance that nativity has on cervical cancer outcomes. Recognizing the heterogeneity of the Black population is an important step to delivering personalized medical care and understanding on a more individual basis the factors that contribute to survival from the disease.
Supplemental Material
Supplemental Material - Differences in Cervical Cancer Outcomes by Caribbean Nativity in Black and White Women in Florida
Supplemental Material for Differences in Cervical Cancer Outcomes by Caribbean Nativity in Black and White Women in Florida by Patricia P. Jeudin, Alex P. Sanchez-Covarrubias, Amanda R. Thiele, Isildinha M. Reis, Erin Kobetz, Sophia H. L. George, and Matthew P. Schlumbrecht in Cancer Control
Footnotes
Acknowledgments
The Florida cancer incidence data used in this report were collected by the Florida Cancer Data System under contract with the Florida Department of Health (DOH). The views expressed herein are those of the author(s), and do not necessarily reflect those of the contractor or DOH. The authors would also like to thank the Sylvester Comprehensive Cancer Center for its ongoing support of this work.
Author Contributions
PJ, AS-C, and MS devised the project, the main conceptual ideas, and research question. PJ, AS-C, IMR, and ART analyzed the data and wrote the paper with input from all authors. IMR, EK, and SHLG provided input and edits on the final draft of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Approval for review and analysis of database was obtained from The Florida Department of Health Institutional Review Board, IRB Approval #0004682.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.