
Abstract
With the improvement in survival of patients with tumors, and continuous advancement of diagnostic technology and treatment modalities, instances of multiple primary malignancies (MPMs) are becoming an increasingly common phenomenon. The occurrence of esophageal-relevant MPMs increases the difficulty of diagnosis and treatment, and the overall prognosis is poor. Esophageal cancer related-MPMs tend to occur in areas such as the head, neck, stomach, and lungs. “Field cancerization” is one theoretical basis for the disease, and chemoradiotherapy, environmental life factors, and gene polymorphism are etiological factors. However, the influence of new therapeutic methods on MPM is still unclear, and the relationship between gene polymorphism and MPMs related to esophageal cancer needs further elucidation. Additionally, there is a lack of unified standards for diagnosis and treatment. Therefore, this study aimed to review the causes, clinical features, and prognostic factors of MPMs related to esophageal cancer.
Introduction
Esophageal cancer (EC) is a common malignant tumor of the digestive system. In fact, the incidence of EC was ranked 7th and the mortality ranked 6th among malignant tumors worldwide in 2020. 1 China has a high incidence of esophageal cancer, with approximately 240,000 new cases every year. The incidence of esophageal cancer ranks 6th, and its mortality rate ranks 4th among all cancers in China. 2 Therefore, EC is a significant public health issue in China. Thanks to the continuous improvement of various treatments, the survival of patients with esophageal cancer has significantly improved, and multiple primary malignancies (MPMs) are becoming more common. MPMs occur when there is more than one synchronous or metachronous cancer in the same individual. Increased survival, advanced diagnostic techniques, and treatment modalities, such as radiation and chemotherapy, may contribute to the increased MPM detection rate. The recurrence of MPMs in patients with esophageal cancer makes the disease more complex and difficult to diagnose and treat; therefore, the prognosis is not ideal. Most of the previous literature focused on the diagnosis and treatment of esophageal single primary cancer, with only a few reported analyses of MPMs related to esophageal cancer. This article reviews the most current research on MPMs associated with esophageal cancer and discusses the causes, treatment, and prognosis of MPMs associated with esophageal cancer.
Definition and Status of Multiple Primary Malignancies Associated With Esophageal Cancer
Definition of Multiple Primary Malignancies
Multiple Primary Malignancies, also known as multiple carcinomas, are malignancies that occur in the body simultaneously or two or more primary malignant tumors that occur successively. MPMs can occur between different organs or tissues in the body or within the same tissue or organ. The earliest case of MPMs dates to 1889, when Billroth first reported a case of gastric cancer after surgery for epithelial carcinoma of the outer ear. The clinical diagnostic criteria for MPMs tend to be those proposed by Warren and Gates 3 in 1932, which are as follows: (1) all primary malignancies must be pathologically confirmed as malignant; (2) The pathological morphology of all malignancies is different; (3) Recurrence or metastasis of cancer must be ruled out. In 1961, Meortel 4 divided MPMs into synchronous MPMs (diagnostic interval ≤6 months) and metachronous MPMs (diagnostic interval >6 months) according to the interval between the two cancers, to further clarify the diagnostic criteria for MPM diagnosis.
Multiple Primary Malignancies Associated With Esophageal Cancer
China has the highest incidence and mortality rate of esophageal cancer, with 253,000 new cases and 194,000 deaths per year. 5 Squamous cell carcinoma accounts for most esophageal cancers in China, and the prognosis is very poor; the 5-year survival rate of patients with middle and advanced esophageal squamous cell carcinoma is only about 26%. 6 However, the prognosis of esophageal cancer varies greatly among different stages, and the 5-year survival rate of early esophageal cancer is more than 70%. 7 Within a certain range, with the extension of postoperative survival, the incidence of esophageal cancer related-MPMs increased significantly.8–10 Therefore, MPMs are not uncommon in patients with esophageal cancer.
Incidence of MPMs Associated With Esophageal Cancer.
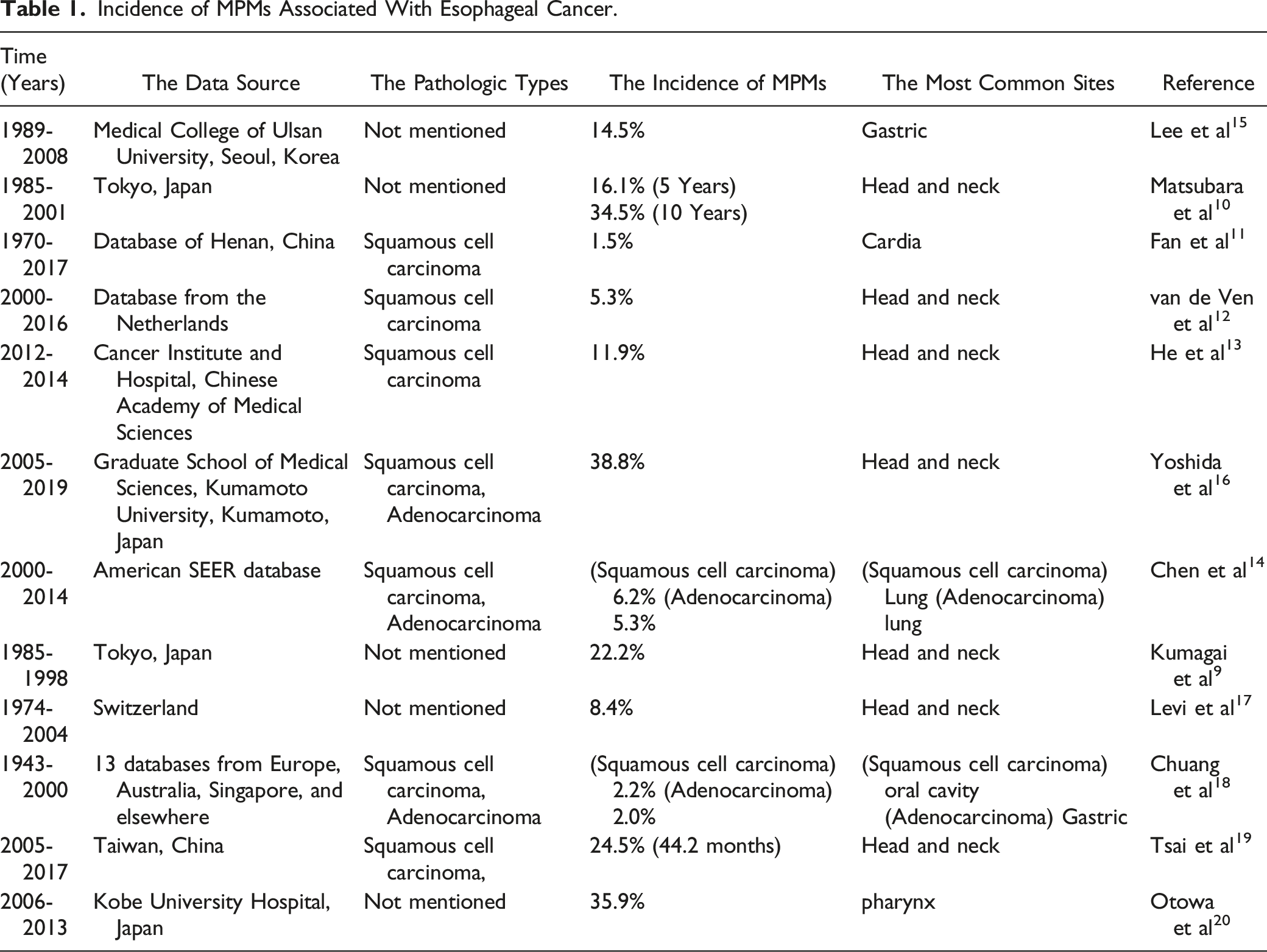
The incidence rate of esophageal cancer in Asian countries, such as China and Japan, is much higher than that in the United States and Europe; which may be due to the different types of esophageal cancer tissues that are affected in cases from these different regions of the world. Esophageal squamous cell carcinoma is more common in Japan and China, while the incidence of squamous cell carcinoma in the United States and Europe is relatively low. 1 Due to the increasingly advanced diagnostic and treatment methods, the survival time of esophageal cancer patients is prolonged, and the incidence of MPMs has therefore increased.8–10 Improvements in diagnostic methods have also led to higher detection rates; therefore, recent studies report higher frequencies of MPMs. In addition, study duration and patient follow-up time were not uniform across studies, which may partially explain large differences in the incidence of MPMs associated with esophageal cancer. This was considered a major limitation when comparing the results across studies. After excluding literature that was published before 2000, we conclude that the incidence of MPMs related to esophageal cancer is between 5% and 38.9%.
Risk factors for MPMs in patients with esophageal cancer include age <70 years, being male, squamous cell carcinoma diagnosis, early disease stage, and history of smoking and alcohol consumption.14,21 Additionally, prior radiotherapy and chemotherapy are risk factors for developing MPMs. The sites of MPMs associated with esophageal cancer that were reported in the literature vary, however, majority of them are concentrated in the head and neck, stomach, colorectum, and lung.7,11,12 MPMs associated with esophageal squamous cell carcinoma are more likely to occur in the oral cavity, pharynx, and esophagus, while MPMs associated with esophageal adenocarcinoma are more likely to occur in esophagus, stomach, and small intestine. 14
For different primary tumors, MPMs occur in different locations. For example, lung cancer related-MPMs tend to occur in colorectum, breasts, and thyroid. Liver cancer related-MPMs are prone to occur in the lungs, colorectum, and thyroid. Breast cancer related-MPMs are more likely to occur in uterus, ovaries, and thyroid.22–24 The location propensity of MPMs may be related to the following factors: (1) The colorectum and lungs are prone to cancer; (2) Some MPMs and primary tumors have similar etiology/pathogenic factors. For example, breast cancer patients are greatly affected by hormone levels in the body, so it is common to encounter a combination of MPMs in the uterus, ovaries, and other parts, because lesions in these organs are also closely related to estrogen levels in women. (3) The location of MPMs is also closely related to treatment techniques. For example, MPMs related to lung, liver, and breast cancer develop easily in the thyroid, because radiotherapy and chemotherapy may induce thyroid cancer. Most MPMs associated with esophageal cancer occur in the head and neck, stomach, colorectum, and lungs. The reasons may include: (1) The stomach, colorectum, and lungs are the most common sites of malignant tumors; (2) bad diet, smoking, drinking, and other factors stimulate esophageal cancer, but also easily induce cancer in the adjacent regions (hypopharynx, cardiac, and others); (3) radiotherapy for esophageal cancer may also induce tumors in adjacent organs, such as the lungs and thyroid, among others. Therefore, the etiology of MPMs in esophageal cancer is discussed in further detail below.
Causes of Multiple Primary Malignancies Associated With Esophageal Cancer
“Field Cancerization” is the Theoretical Basis of Multiple Primary Malignancies
Slaughter’s “Field cancerization” theory 21 is a good model for the development of MPMs; chronic and repeated exposure to carcinogenic substances, such as tobacco and alcohol, leads to genetic mutations that eventually lead to multiple independent lesions in the digestive tract epithelium.
Tumor development is a multi-step process, summarized as the initiation stage, promotion stage, tumor evolution stage, and tumor progression stage.
25
The occurrence of MPMs related to esophageal cancer can be summarized as the following process (Figure 1): (1) Under the stimulation of long-term carcinogenic factors, the esophagus and its adjacent epithelial cells form one or more cloned cells with genetic mutations. (2) These cloned cells proliferate and differentiate continuously, forming a large continuous area of altered genetic cells. (3) Some of these cells showed irreversible malignant transformation and eventually formed esophageal cancer. (4) However, the cells in the adjacent area of esophageal cancer are in the initiation or promotion stage and have not completely evolved into tumor cells. After the diagnosis of esophageal cancer, these areas may degenerate or eventually disappear, or they may eventually progress to become tumor cells. For instance, Tabor et al
26
performed a molecular analysis of non-cancerous adjacent tissue from surgical margins of head and neck tumors and found that at least 1/3 of the cells had tumor-related genetic alterations. Similarly, Wu et al
27
found cloned cells of the same origin as tumor cells in regions adjacent to the head and neck cancer, and found genetic mutations in these adjacent regions that were different from the primary tumor cells, also strongly supporting the “field cancerization” theory. Mechanisms of MPMs associated with esophageal cancer.
Multiple Primary Malignancies Induced by Radiotherapy
Although radiation can treat tumors, it can also induce second cancers in nearby organs.28,29 Factors associated with radiation-induced cancer include (1) age at the time of radiation therapy; the younger the age, the higher the risk of MPMs,30,31 (2) the longer the survival time after radiotherapy, the higher the chance of MPMs,32,33 (3) genetic risk factors, such as carrying an ATM gene mutation will significantly increase the risk of MPMs after radiotherapy, 34 (4) Radiation-sensitive organs such as the lungs, colon, breast, thyroid, and bladder are at higher risk of MPMs after exposure to radiation, 35 (5) Within a certain range, the risk of MPMs increased linearly with the increase in radiotherapy dose.36,37 However, a high radiation dose will directly kill the cells; therefore, the risk of MPMs will be reduced. 38
In addition to causing DNA damage, radiotherapy leads to the formation of initial cloned cells with genetic alterations. It may also continue to act on genetically altered regions around esophageal cancer, further accelerating the transformation from pre-tumor cells to tumor cells. Radiotherapy does not conflict with regional cancer chemistry. For esophageal cancer, receiving radiation can lead to an increased risk of cancer in neighboring organs such as the lungs, thyroid, and larynx,
39
as shown in Figure 2. However, larger, and high-quality studies are needed to further explore the occurrence of MPMs related to radiotherapy and esophageal cancer. Mechanism of MPMs induced by radiotherapy and chemotherapy in esophageal cancer (lung cancer as an example).
Chemotherapy-Induced Multiple Primary Malignancies
MPMs Induced by Chemotherapy Drugs.

Combined Chemoradiotherapy and Multiple Primary Malignancies
Radiation therapy increases the risk of breast cancer in patients with Hodgkin’s lymphoma, while chemotherapy with alkylating agents significantly reduces the risk of breast cancer.53–55 However, the study of Morton et al 49 provided strong evidence for the synergistic promotion of MPMs by radiotherapy and chemotherapy. The risk of gastric cancer was significantly increased (25 cases, two controls; odds ratio [OR], 77.5; 95% CI, 14.7-1452) when patients received both radiation to the stomach ≥25 Gy and high dose procarbazine (≥5600 mg/m2). The risk was significantly reduced (OR, 2.8; 95% CI, 1.3-6.4) when patients received radiation to the stomach ≥25 Gy but procarbazine <5600 mg/m2. The risk was also reduced (OR, 2.8; 95% CI, 1.3 to 6.4) among patients who received procarbazine ≥5600 mg/m2 but radiation to the stomach ≤25 Gy. The reason may be related to the synergistic destruction of cellular DNA by radiotherapy and chemotherapy. 56 The effect of combination therapy on MPMs appears to be at two extremes. Its effect on MPMs associated with esophageal cancer is also unclear, and the potential effect of combination therapy on increasing/decreasing the incidence of MPMs needs more exploration.
Multiple Primary Malignancies Are Induced by Environmental and Life Factors
Many studies10,57 have shown that risk factors for recurrent MPMs in esophageal cancer include male sex, squamous cell carcinoma diagnosis, early-stage of esophageal cancer, smoking and alcohol consumption as risk factors, further supporting the “field cancerization.” Moreover the incidence of MPMs increased significantly with prolonged postoperative survival.7–10 It is hypothesized that men who have been exposed to risk factors, such as smoking and alcohol consumption, for a considerable time have a longer life expectancy after diagnosis of esophageal cancer with an earlier stage and a greater chance that the preneoplastic cells in the adjacent epithelium will become tumor cells. Smoking and alcohol consumption are also risk factors for head and neck cancer. The fact that patients with esophageal cancer are more likely to have MPMs further confirms the “field cancerization.”
Gene Mutation and Multiple Primary Malignancies
The occurrence and development of cancer are closely related to the dysregulation of the cell cycle, the inactivation of tumor suppressor genes, and the activation of proto-oncogenes. Genetic mutations play an important role in MPMs development. For example, Lynch syndrome, which includes mutations in several genes (MLH1, MSH2, MSH6, PMS2, and EPCAM), is associated with an increased risk of colorectal, gastrointestinal, liver, kidney, brain, and skin cancers. 58 Another gene involved in multiple tumors is the BRCA gene. 59 Mutations in the BRCA gene increase the risk of breast and ovarian cancers, as well as pancreatic and prostate cancers. Smoking and drinking alcohol are closely related to TP53 gene mutations. As a molecular change associated with various human malignant tumors, TP53 gene mutations are closely related to various malignant tumors such as esophageal cancer and lung cancer. Yokoyama et al 60 showed that ADH2 and ALDH2 gene polymorphism was associated with MPMs of the digestive tract. The presence of ADH2*1/2*1 or ALDH2*1/2*2 genotypes would lead to an increased risk of oropharyngeal cancer and esophageal cancer. When the two genotypes were present at the same time, the risk of oropharyngeal cancer and esophageal cancer showed multiple increases (OR = 121.77 (31.87-465.33) and 40.40 (17.85-91.45), respectively). In addition, Janxin et al 61 found that multiple SNP loci in the Han population in the Henan Province of China are associated with genetic susceptibility to esophageal and gastric cancer, and genetic variation of rs4785204 and rs4924935 may explain the high incidence of esophagogastric MPMs in this population.
Prognostic Factors of Multiple Primary Malignancies Associated With Esophageal Cancer
Prognosis of Multiple Primary Malignancies With Esophageal Cancer and Single Primary Esophageal Cancer
The prognosis of MPMs associated with esophageal cancer is closely related to the diagnostic interval. In general, the OS of synchronous MPMs is less than that of single primary esophageal cancer.62,63 However, whether there is a difference in prognosis between heterogeneous MPMs and single primary cancer remains controversial. Some studies14,64 believe that the combination of esophageal cancer and other primary cancers does not affect the prognosis, or that the prognosis is even better than that of esophageal single primary cancer.
Both synchronous MPMs and metachronous MPMs have a worse prognosis than single primary esophageal cancer (SEC). The reasons for the erroneous conclusion that SEC has a better prognosis are as follows. First, the prognosis of synchronous MPMs and metachronous MPMs is very different. 62 Therefore, when comparing the prognosis of MPMs with SEC, it is important to distinguish whether MPMs are simultaneous or metachronous. Furthermore, metachronous MPMs are more commonly seen in patients with early-stage disease and young age.12,14 These patients can usually tolerate more aggressive treatment regimens and already have a longer life expectancy, and it is easy to conclude that MPMs have a better prognosis without differentiation of esophageal cancer stages. Confounding factors such as the esophageal cancer stage should be adjusted for to compare the prognosis of metachronous MPMs with that of SEC. Additionally, during the interval from the diagnosis of esophageal cancer to the diagnosis of MPMs, patients with SEC may die due to disease progression, postoperative complications, and other causes. Moreover, the longer the interval, the more SEC patients are likely to die during this period, which may lead to greater error.
Chen et al
14
and Mukhtar et al
64
came to this conclusion for the following reasons: (1) When comparing the prognosis of MPMs associated with esophageal cancer and primary esophageal cancer, confounding factors such as esophageal cancer stage were not controlled, because MPMs were more likely to appear in patients with early esophageal cancer and patients with longer survival time; the study by Mukhtar et al
64
points to this as a possible reason for their conclusion. (2) Their study did not account for the fact that patients with SEC may die of various causes within the time interval between diagnosis of MPMs (Figure 3A). Comparison of the prognosis of MPMs and SEC, the time interval in yellow represents the total survival time of the patients while that in blue represents the interval from diagnosis of esophageal cancer to diagnosis of MPMs. (A) The researchers ignored the fact that some patients with SEC had died during the time interval, and finally concluded that the prognosis of MPMs was better than that of SEC. (B) The ratio of MPMs to SEC was set at 1:3 for propensity matching, and the 3 patients with SEC must also be guaranteed to be alive during the interval.
To analyze the effect of MPMs during the treatment of esophageal cancer on the prognosis of patients with esophageal cancer, we can use the propensity matching method. For example, in the retrospective study, propensity matching was conducted according to the ratio of 1 to 3. For one patient with multiple primary cancers related to esophageal cancer, MPMs occurred 6 months after the diagnosis of esophageal cancer, the 3 reference subjects must also be guaranteed to be alive within 6 months after the diagnosis of esophageal cancer (Figure 3B). In addition, factors such as the stage of esophageal cancer and the age of patients in SEC group should be essentially consistent with MPMs. We hope this approach will avoid the influence of confounding factors, such as stage and age, on the outcome. Additionally, this method may mitigate the effects of interval deaths of patients with SEC on the overall prognosis. Literature does not currently show that this method can avoid these confounding factors. We hope future researchers pay attention to this problem and draw more accurate conclusions about the prognosis of esophageal cancer related-MPMs.
Prognostic Factors and Treatment of Multiple Primary Malignancies Associated With Esophageal Cancer
The physical condition of tumor patients can greatly affect the prognosis, which is also true for MPMs associated with esophageal cancer. 57 Age, stage of esophageal cancer, and whether there are underlying diseases will affect the prognosis.
The interval for MPMs diagnosis is also important14,62: the longer the interval, the better the prognosis. The prognosis of synchronous MPMs was significantly worse than that of heterogeneous MPMs, and this rule applies to other types of MPMs as well.65,66 The possible reason is that patients were diagnosed with multiple malignant tumors in a short period, and the body could not tolerate radical treatment, resulting in a poor prognosis.
In addition to the stage of esophageal cancer, the prognosis of MPMs was significantly correlated with the malignancy and stage of other primary tumors. Chen et al 14 conducted a study confirming that esophageal cancer combined with prostate cancer has the best prognosis among all MPMs as prostate cancer itself has a good prognosis. 67 In the early stages of prostate cancer, the 15-year survival rate is more than 80%; therefore, it does not have a significant impact on prognosis. In the study by Lee et al, 15 the prognosis of esophageal cancer combined with head and neck cancer was the worst among all MPMs. The 5-year survival rate was only 9.2%, which was much lower than that of esophagus cancer combined with stomach cancer (52.7) and, also much lower than that of esophagus cancer combined with lung cancer (27.0%). The authors speculated that the surgical area of head and neck cancer is complex and adjacent to vital organs; therefore, it could not be completely resected.
Different treatment methods have a great impact on MPM prognosis. Wen et al 57 reported that surgery, radiotherapy, and chemotherapy are protective factors for the prognosis of MPMs. The studies of Otowa et al 20 and Lee et al 15 also proved that surgical treatment of MPMs was tolerable and had a good prognosis. However, Natsugoe et al 68 found a higher postoperative mortality rate (8.5-9.3%) for MPMs associated with esophageal cancer. In addition, Lv et al 65 reported that MPMs patients who received surgery-based combined therapy (surgery combined with chemotherapy or radiotherapy) had a longer survival time than those who received surgery alone. Therefore, it is necessary for clinicians to integrate the conditions of MPMs patients, strictly grasp the indications of surgery, and choose radiotherapy or chemotherapy and other comprehensive treatment methods when necessary.
Limitations
As mentioned in section 1.2, esophageal cancer related-MPMs has an incidence of between 5 and 38.9%, as shown in this review. The large incidence range may be related to the small number of studies that were included in this review, together with the differences in follow-up times in these reported studies.
The “Field cancerization” is closely related to the occurrence of MPMs, which suggests that MPMs may be derived from the same clonal cell; therefore, the definition and diagnostic criteria of MPMs may need further clarification. In addition, therapeutic factors such as radiotherapy, chemotherapy, and gene polymorphism can also induce MPMs. However, the influence of emerging therapies such as immunotherapy, targeted therapy, and combination therapy on MPMs needs more exploration.
The prognosis of MPMs remains controversial; however, Chen et al 14 and Mukhtar et al 64 concluded that the prognosis of MPMs with esophageal cancer stage does not greatly differ from that of SEC, and may be even better than that of SEC. However, Chen 14 and Mukhtar et al 64 did not consider the influence of different stages of esophageal cancer on prognosis, and did not account for the fact that patients with SEC may die of various causes within the time interval between diagnosis of MPMs. Therefore, theoretically, the prognosis of MPMs combined with esophageal cancer is significantly worse than that of SEC. However, larger, higher-quality studies need to be conducted to confirm this.
Conclusion
MPMs associated with esophageal cancer is a common clinical phenomenon. The known causes include “Field cancerization” and treatment related MPMs. Its prognosis is worse than that of SEC at the same stage, so early diagnosis is particularly important. For patients with high risk factors, it is necessary to strengthen the screening of high-risk sites such as head, neck, and stomach. In view of the complex condition of MPMs associated with esophageal cancer, it is necessary to choose an individualized treatment plan that takes the patient’s physical condition and the treatment opinions of various disciplines into account.
Footnotes
Appendix
Acknowledgments
Author Contributions
Yu Cui: Writing - Original Draft, Visualization, Wenxia Ren: Data Curation, Lu Yang: Writing - Review & Editing, XueDue: Visualization, Bangxian Tan: Writing - Review & Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.