
Abstract
Objective
We investigated the prognostic value of cyclin-dependent kinase 5 (CDK5) in a true population-based cohort of patients with colon cancer.
Methods
1. Immunohistochemical (IHC) staining was used to retrospectively analyse the expression of CDK5 in colon cancer tissue samples of 296 patients. The χ2 test, Kaplan-Meier method and Cox proportional regression model were used to analyse the difference between the patients with differential expression of CDK5 and with different stages (metastatic and nonmetastatic); 2. The number of tumour-infiltrating lymphocytes (TILs) in tumour sections was determined, and its relationship with prognosis was explored.
Results
1. Among 296 patients stained for CDK5, 18 cases (6.09%) showed negative expression, 77 cases (26.01%) showed weak expression (+1), 124 cases (41.89%) showed medium positive expression (2+), and 77 cases (26.01%) showed strong positive expression (3+). The expression of CDK5 was neither related to mismatch repair nor TILs (p > .05). In non-metastatic patients, longer progression-free survival (PFS) and cancer-specific survival (CSS) were observed in patients with high CDK5 expression (2+ or 3+) than low CDK5 expression (- or 1+), while in metastatic disease, the opposite was true (p < .001). 2. TILs in 226 patients were detected in the study. Among them, 115 cases (50.88%) showed a low number of TILs (TILs-L), and 111 cases (49.12%) showed a high number of TILs (TILs-H). Patients with a TIL ratio greater than .2 had a significantly better CSS (p < .001) or PFS (p = .008) than patients with a lower TIL ratio. By multivariate analysis, TILs-H was a protective factor for CSS, however failed to reach a significant difference (hazard ratio: .59, 95% CI: .33∼1.06, p = .079), and so was the PFS (HR: .65, 95% CI: .29∼1.43, p = .279).
Conclusion
High expression of CDK5 indicates a good prognosis in nonmetastatic colon cancer, while it is the opposite in metastatic colon cancer, and the expression of CDK5 is unrelated to TILs. Patients with TIL-H have a better prognosis, with a proper cut-off value of 20% for colon cancer.
Introduction
Colon cancer is the third most common gastrointestinal malignancy in the United States. The incidence rate has declined recently in European and American countries, but it is still increasing in China. However, due to the heterogeneity of colon cancer, many existing biomarkers have limited effects in early diagnosis or predicting clinical outcomes. Therefore, additional prognostic markers are needed to stratify the clinical prognosis of colon cancer. In this case, cyclin-dependent kinase 5 (CDK5) might be a promising marker.
CDK5 is a unique member of the cyclin-dependent kinase family. Recently, CDK5 has been reported to play a key role in tumorigenesis and progression. The team of professor Nelkin discovered the tumour-promoting effect of CDK5 first in prostate and pancreatic cancers and found that CDK5 was related to the ral gene in the K-RAS pathway,1,2 for which targeted therapy has been successfully applied in colon cancer.3,4 In patients with advanced colon cancer who were treated with oxaliplatin, high expression of CDK5 was associated with a shorter time to progression (TTP) (median 8.10 months vs 18.23 months, P = .043), while no difference was observed among patients treated with irinotecan (median 8.95 months vs 8.42 months, P = .450). 5 This study partially suggested the predictive effect of CDK5 in colon cancer, but the underlying mechanism deserves further elucidation.
Alternatively, a study in medulloblastoma cell lines showed that CDK5 could also specifically upregulate the expression of programmed death 1 ligand (PD-L1) on the tumour surface. 6 Inhibiting the infiltration of T lymphocytes in the tumour microenvironment (TME) could eventually lead to tumour immune escape. The low expression of CDK5 in non-small cell lung cancer could suppress the expression of PD-L1, indicating that the expression of CDK5 might be related to tumour immunity. 7 Tumour-infiltrating lymphocytes (TILs) are a crucial component of the TME and reflect the antitumour immune response of the host.8-10 In some solid tumours, TILs are crucial for inhibiting cancer progression and have implications for the success of active cancer immunotherapy. High levels of TILs were associated with favourable outcomes in a real-world immunotherapy cohort of patients.11-13
Previously, a team at Southern Medical University found that CDK5 was highly expressed in colon cancer, and the expression was positively correlated with late staging and poor histological differentiation. 14 However, only 89 patients were enrolled. Our study aimed to detect the expression of CDK5 and TILs in colon cancer to clarify their clinical significance and explore their relationship.
Materials and methods
Clinical Data
Retrospectively analyzed 296 patients with colon carcinoma who had undergone radical colon resection at the Affiliated Jinhua Hospital, Zhejiang University School of Medicine between September 12, 2016, and May 25, 2022 (Supplementary Figures S1). All cases were confirmed pathologically, and the latest follow-up date was February 9, 2023. Haematoxylin and eosin (H&E)-stained tumour sections were reviewed by 2 experienced pathologists to ensure the accuracy of the pathological diagnosis, and confirmed by another pathologist with higher professional titles in case of the inconformity of the results. Postoperative follow-up was performed by a dedicated person in outpatient clinics, door-to-door visits, or telephone follow-ups. The recorded survival time (cancer-specific survival, CSS) was from the time of surgery to the time of the last follow-up, the time of death, or the time of being lost to follow-up. No radiation treatment was administered to any of the patients. Chemotherapy after surgery was applied according to the National Comprehensive Cancer Network (NCCN) guidelines or the Chinese Society of Clinical Oncology (CSCO) guidelines. All patient information had been deidentified. All sample and data collections were performed with the approval of the Affiliated Jinhua Hospital, Zhejiang University School of Medicine. This study was reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology reporting specifications. 15
Methods
Immunohistochemical staining of CDK5
(1) The production of a colon cancer tissue microarray: ① Identify the colon cancer tissue wax block according to the patient’s name and the corresponding surgical pathology number; ② Sort the paraffin blocks in the order of pathology number, corresponding to the basic information of the patient; ③ Punch holes in the paraffin block to obtain samples, which were placed into the wells of the tissue microarray to make a tissue array with 80 wells per plate; and ④ Tissue chip slices and subsequent patches and baking sheets were prepared for immunohistochemical (IHC) staining.
(2) IHC staining of CDK5: ① The prepared wax block of colon cancer tissue chip was cut into 3 μm sections, the sections were placed in a thermostat, the temperature was set to 60 °C, and the sections were baked for 1 hour; ② The cells were stained on the automatic immunohistochemistry instrument (Leica Bond-MAX, Germany); and ③ The cells were incubated with rabbit monoclonal antibody (Biyuntian, China) and placed in a 4°C constant temperature refrigerator overnight. The cells were incubated with universal secondary antibody (Leica Bond, Germany) at room temperature and rinsed with PBS solution 3 times. Then, DAB colour development, haematoxylin counterstaining, dehydration, and mounting microscopy were performed.
(3) Scoring IHC staining intensity: Under the microscope, 2 senior pathologists independently reviewed and scored the cells according to the number of positively stained tumour cells and staining intensity, and confirmed by another pathologist with higher professional titles in case of the inconformity of the results. The scoring standards were as follows: 0 points (negative), 1 point (weak positive), 2 points (medium positive), and 3 points (strong positive). Staining was graded according to the following criteria: 0 (no staining), 1 (weak staining = light yellow), 2 (medium staining = yellowish brown), and 3 (strong staining = brown), as shown in Supplementary Figures S2.
The Number of TILs
(1) The evaluation of TILs: ① The H&E-stained tissue section according to the patient’s name and corresponding surgical pathology number was identified; ② The number of TILs in the H&E-stained section in 5 fields of view were evaluated microscopically. The lowest, highest and average values were recorded.
(2) The standards of the evaluation were as follows:
16
(1) Selection of the tumour area: TILs should be evaluated in the area of deepest tumour infiltration. Define the substrate area. (2) Determined type of inflammatory infiltrate: All mononuclear cells (including lymphocytes and plasma cells) should be scored. (3) Assessing the percentage (%) of stromal TILs: The denominator used to determine the % of stromal TILs is the area of stromal tissue (i.e., area occupied by mononuclear inflammatory cells over the total intratumoral stromal area), not the number of stromal cells (i.e., fraction of total stromal nuclei that represent mononuclear inflammatory cell nuclei). (4) TILs outside of the tumour border were excluded. TILs in tumour zones with crush artefacts, necrosis, regressive hyalinization and a previous core biopsy site were excluded.
Statistical Analysis
R version 4.0.5 software was used for all statistical analyses. χ2 and Fisher’s exact tests were used to analyse enumeration data. Measurement data are presented as the mean ± standard deviation (‾x ± s). A t test was used to compare normally distributed data, and the Mann‒Whitney U test was used to compare nonnormally distributed data. The cut-off values of TILs was obtained by restricted cubic spline (RCS). The primary endpoints were PFS and CSS, and PFS was defined as the time from the first diagnosis of the cancer to progression of the carcinoma or the loss of follow-up. CSS was defined as the time from the first diagnosis of the cancer to death due to the carcinoma or the loss of follow-up. The duration of survival was calculated according to the Kaplan-Meier method, and differences of the survival curves were assessed using the log-rank test. The correlation between clinicopathological characteristics and prognosis was analysed according to the Cox risk proportional regression model. All P values were two-sided, and statistical significance was determined at P < .05.
Results
Clinical Characteristics
Descriptive characteristics of 296 patients in the study population.

aStaging based on the eighth AJCC system of the colorectal carcinoma. P < .05: the differences were considered statistically significant. TIL was unevaluable in some patients due to the limited biopsy specimen of the lesions.
AJCC: American Joint Committee on Cancer, NA: Nonapplication, AC: Adenocarcinoma, SRCC: Signet ring cell carcinoma, MMR: Mismatch repair, TIL: Tumor infiltrating lymphocyte, TIL low: 0≤ TIL ratio ≤ .2; TIL high: .2< TIL ratio ≤1.
Expression of CDK5 and the Number of TILs and Their Relationships with the Clinicopathological Features of Patients with Colon Cancer
To investigate the relationship between clinicopathological features and CDK5 as well as TILs in colon cancer, IHC staining was used to test the expression of CDK5 and the number of TILs in HE-stained tumour sections was determined. The expression of CDK5 was detected in 296 colon cancer tissue microarrays with IHC staining and recorded the results. We scored CDK5 according to the intensity of IHC staining. The results suggested that CDK5 in colon carcinoma was mainly expressed in the cell membrane or cytoplasm. Among them, 18 cases (6.09%) showed negative expression, 77 cases (26.01%) showed weak expression (+1), 124 cases (41.89%) showed medium positive expression (2+), and 77 cases (26.01%) showed strong positive expression (3+). Through initial exploration, it was found that the CDK5 expression with 4 categories was not related to the prognosis clearly (Supplementary Figures S3), so we divided CDK5 expression into high (2+ or 3+) and low levels (- or +) for further investigation. A score ≥2 points was defined as high expression, and a score ≤1 point was defined as low expression. CDK5 expressed at low levels (- or +) in 95 cases (32.09%) and at high levels (2+ or 3+) in 201 cases (67.91%). The expression of CDK5 was not related to the age, gender, tumour site, T stage, mismatch repair (MMR), or TILs (P > .05). However, CDK5 high expression was more frequent in mucinous adenocarcinoma or metastatic disease (P < .05), as shown in Table 1.
In addition, H&E staining was used to detect the number of TILs and interestingly, it was found that TILs were related to CEA levels in peripheral blood (P = .033). All samples were jointly evaluated by 2 pathologists who were unaware of any clinical information. An RCS curve corresponding to a cut-off of 20% indicated that tumours showing a proportion of TILs ≤20% were defined as “low number of TILs” (TILs-L), whereas tumours showing a proportion of TILs >20% were defined as “high number of TILs” (TILs-H), as shown in Figure 1(A). Thus, 115 cases (50.88%) showed TILs-L, and 111 cases (49.12%) showed TILs-H. The number of TILs was related to AJCC stage (P = .021), MMR status (P = .001) and N classification (P = .016), but not to the age, gender, histology, or chemotherapy, with all P values greater than .05. The correlation between CDK expression and TILs and the clinical features is shown in Figure 1(B). Colour blue indicated that the 2 variables in the cell were positively correlated. Conversely, colour red indicated that the variables were negatively correlated. The relevance is shown by the size of the filled pie block (Figure 1(B)). TILs-H patients had a lower level of CEA, as shown in Figure 1(E). TILs were not related to the age, albumin levels in peripheral blood, body mass index (BMI) or the CDK5 ratio (P > .05), as shown in Figure 1. Correlation between TILs and clinical features. (A) The RCS curve of TILs. (B) Corrgram of clinical features and TIL intercorrelations. (C) The relationship between TILs and CDK5 ratio. (D) The relationship between TILs and age. (E) The relationship between TILs and CEA in peripheral blood. (F) The relationship between TILs and body mass index. (G) The relationship between TILs and albumin in peripheral blood.
Influences of MMR Status, TILs on Survival of Colon cancer
Mismatch repair deficiency (dMMR) and TILs-H were believed to be associated with a preferable survival. With the intent to prove the results, we attempted to explore the influences of MMR status and TILs on survival of colon cancer. As a result, the PFS of patients with dMMR status was better than those with proficient mismatch repair (pMMR), with a significant difference (P = .012). However, the difference of CSS was not significant between patients with dMMR status and those with pMMR status (P > .05). The outcomes of PFS and CSS differed significantly in favour of TIL-H (≥20%) (P < .05), as shown in Figure 2. Influence of MMR and TILs on the survival of the cohort. (A) Progression-free survival curves according to MMR. (B) Cancer-specific survival curves according to MMR. (C) Progression-free survival curves according to TILs. (D) Cancer-specific survival curves according to TILs.
The Impact of CDK5 on Prognosis in Different Stages and its Subgroup Analysis
Previous research in which only 89 colorectal patients were enrolled, found that the high expression of CDK5 was correlated with late stage and poor histological differentiation, thus indicating a poor survival.
14
To further verify the relevance, we attempted to explore the influence of CDK5 on prognosis of colon cancer in a larger cohort. Consequently, in the entire cohort, patients with high expression of CDK5 had either better PFS or CSS than those with low expression, however, it failed to reach a significant difference (P > .05). Interestingly, for patients with nonmetastatic disease (stage II-III), high CDK5 expression suggested a better PFS and CSS (P < .001). Contrary to the above results, for patients with stage metastatic disease, low CDK5 expression represented a better PFS and CSS (P < .05), as shown in Figure 3. Influence of CDK5 on tumour progression and survival. (A) Progression-free survival curves according to CDK5 expression in the entire cohort. (B) Cancer-specific survival curves according to CDK5 expression in the entire cohort. (C) Progression-free survival curves according to CDK5 expression in patients with nonmetastatic disease. (D) Cancer-specific survival curves according to CDK5 expression in patients with nonmetastatic disease. (E) Progression-free survival curves according to CDK5 expression in the stage IV cohort. (F) Cancer-specific survival curves according to CDK5 expression in the stage IV cohort.
Due to the phenomenon of different effects of CDK5 in metastatic and non-metastatic diseases, a further subgroup analysis was performed to evaluate whether there was differential survival in subgroups of patients with high and low CDK5 expression. As shown in Figure 4, there were both significant differences in PFS and CSS between the subgroups with high and low CDK5 expression that were analysed (P < .001). Subgroup analysis of risk for tumour death and tumour progression. (A) Subgroup analysis of the risk of cancer-specific survival in patients with high and low CDK5 expression. (B) Subgroup analysis of the risk of progression-free survival in patients with high and low CDK5 expression.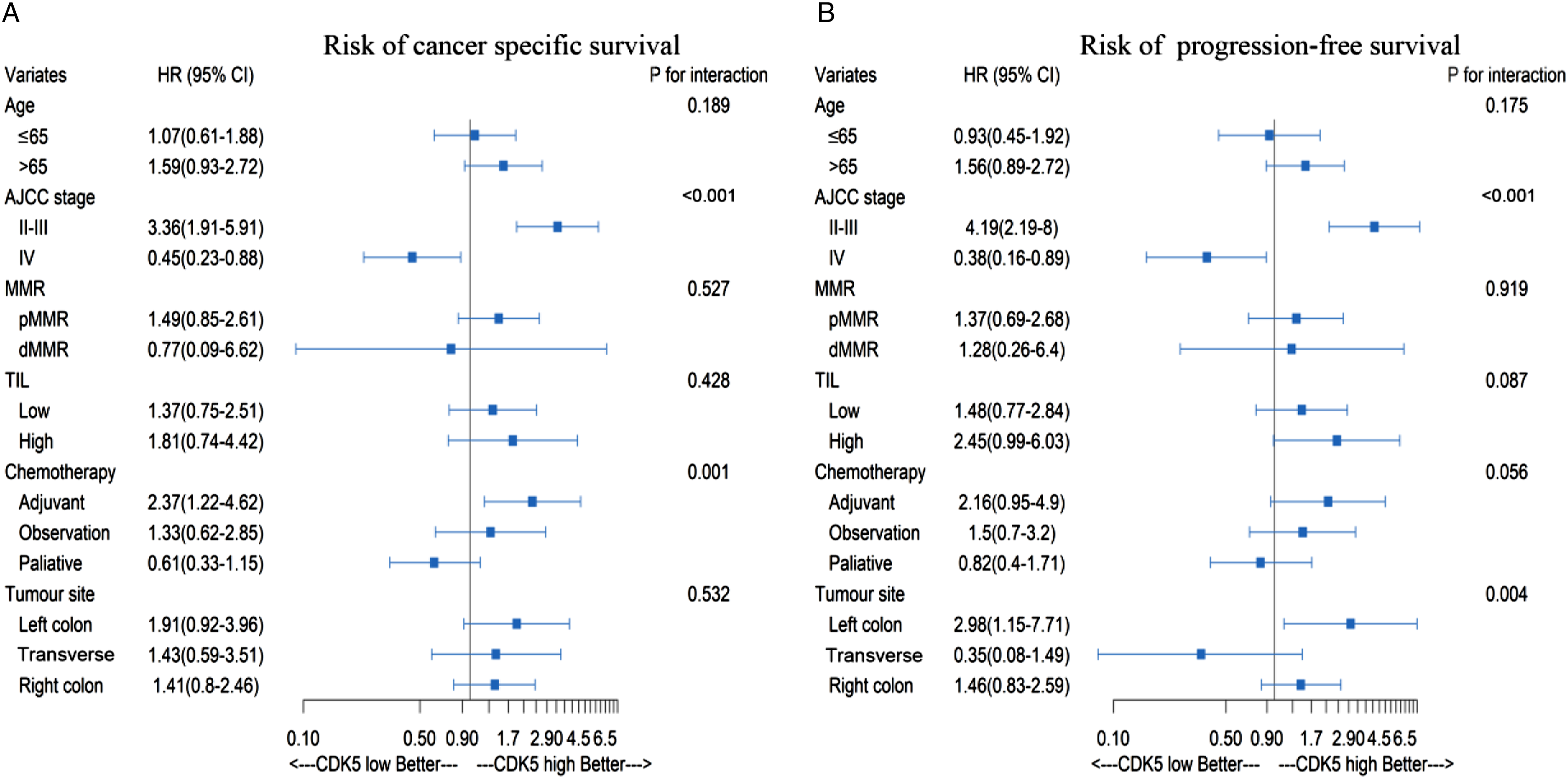
Univariate Analysis and Multivariate Analysis of PFS and OS
To investigate the probable impact of CDK5 and TILs on the PFS and OS of colon cancer, Univariate analysis and multivariate analysis were carried out according to the Cox risk proportional regression model.
Univariate Analyses of Predictors of cancer-specific survival (CSS) and Progression-free Survival (PFS) In the Study Population.

Factors which share a P value less than .20 in the univariate analysis were further enrolled into the multivariate analysis.
aunivariate and multivariate analyses were conducted using cox regression model.
bstaging based on the 8th AJCC system of the colorectal carcinoma. AJCC, American Joint Committee on Cancer; HR, hazard ratio. P < .05: the differences were considered statistically significant.
NA: Nonapplication, TIL: Tumor infiltrating lymphocyte, TIL low: 0≤ TIL ratio ≤ .2; TIL high: .2< TIL ratio ≤1.
Multivariate Analyses of Predictors of cancer-specific survival (CSS) and Progression-free Survival (PFS) In the Study Population.

Factors which share a P value less than .20 in the univariate analysis were further enrolled into the multivariate analysis.
a univariate and multivariate analyses were conducted using cox regression model.
b staging based on the eighth AJCC system of the colorectal carcinoma. AJCC, American Joint Committee on Cancer; HR, hazard ratio. P < .05: the differences were considered statistically significant.
NA: Nonapplication, TIL: Tumor infiltrating lymphocyte, TIL low: 0≤ TIL ratio ≤ .2; TIL high: .2< TIL ratio ≤1.
PFS. In a univariable analysis, AJCC stage, and the ratio of TILs, MMR status and chemotherapy were identified as statistically significant factors affecting PFS (P < .05), as shown in Table 2. In the multivariable analysis, stage IV (HR: 14.27, 95% CI: 6.26∼32.54, P < .001) and palliative chemotherapy (HR: 3.12, 95% CI: 1.12∼8.71, P = .030) remained independent and significant factors affecting PFS, as shown in Table 3.
Probable Mechanism of CDK5 on Prognosis in Different Stages
Base on the results that CDK5 had different effects in metastatic and non-metastatic diseases, we attempted to explore the probable mechanism of this phenomenon by the localization of the CDK5. By observing the HE-stained section under a microscope, we found that in stage II or III colon cancer, CDK5 was localized primarily in the cell membrane or cytoplasm, whereas in 53.6% (37/69) of the stage IV colon cancer, CDK5 accumulated in the nucleus (Figure 5). This result indicated that CDK5 located in the nucleus or cytoplasm may have different biological influences, which called for further verification in a large cohort in future. CDK5 staining in the cytoplasm and nucleus. (A) and (B) The expression of CDK5 in stage II colon cancer. (C) and (D) The expression of CDK5 in stage III colon cancer. (E) and (F) The expression of CDK5 in stage IV colon cancer.
Discussion
In this study, by detecting the expression of CDK5 in a tissue microarray of colon cancer, we found that CDK5 had different prognostic effects in metastatic and nonmetastatic colon cancer. In nonmetastatic colon cancer, patients with high CDK5 expression had longer PFS and OS. However, in metastatic colon cancer, patients with low CDK5 expression had a better prognosis (P < .05). Through the RCS curves, we explored how the Tils influenced the survival of the patients. The results showed that the prognosis of patients with a ratio of TILs greater than .2 was significantly better than that of patients with a lower ratio.
Cyclin-dependent kinases (CDKs) are important kinases that regulate the malignant biological functions of tumour cells. They are a class of proline-directed serine/threonine protein kinases that play a key regulatory role in the cell cycle and participate in the regulation of proliferation, transcription and certain specific metabolic cascades. Among them, CDK5 is an important member that is mainly involved in neuronal growth and signal transduction by combining with activating factors (P35/P39) in neurons after mitosis. Initial research found that CDK5 activity was more related to the development of the brain and the occurrence of Alzheimer’s disease.17,18 During neural development, CDK5 controls cell movement, adhesion, and cytoskeleton formation, all of which are related to the occurrence and development of tumours. 19 In recent years, studies have found that the abnormal expression of CDK5 is related to the occurrence and development of prostate cancer, pancreatic cancer, medullary thyroid carcinoma, hepatocellular carcinoma and other cancers.2,20-24 However, CDK5 plays different roles in different types of cancer, and the role of CDK5 in colon cancer has not been reported. 14 Previous studies have investigated the role of CDK5 in apoptosis and found that the expression of CDK5 in colon cancer tissues was significantly higher than that in normal tissues. The expression of CDK5 was positively correlated with AJCC stage, differentiation degree, tumour size and N stage (P < .05), but only 89 patients were enrolled in the study and the colon and rectum were not studied separately. 14 Therefore, we enrolled 296 patients for this study to make the results more credible.
At present, researchers have found that CDK5 and its activator p35 are involved in the occurrence and development of various tumours and play an important role in gastric cancer. The average OS time of patients with low expression of CDK5 was significantly shorter than that of patients with high expression (40 months vs 75 months). In vitro functional experiments showed that the proliferation and cloning ability of gastric cancer cells were closely related to the intracellular location of CDK5. CDK5 can inhibit the proliferation and cloning of gastric cancer cells by accumulating only in the nucleus. 27 In colon cancer, we found that CDK5 played different roles in metastatic and nonmetastatic colon cancer. To explore its mechanism, we compared CDK5 staining in metastatic and nonmetastatic colon cancer. In nonmetastatic colon cancer, CDK5 was localized primarily in the cytoplasm, whereas in metastatic colon cancer, more than 50% CDK5 accumulated in the nucleus, which may be related to the results, and further research is needed.
Recent studies have shown that CDK5 also plays a crucial role in tumour immune escape. MMR was firstly conceived respectively in 1964 by Evelyn Witkin and Robin Holliday to explain brominated nucleotide processing in bacteria and gene conversion in yeast, 26 which could help to repair mismatched nucleotides in DNA resulting from recombination between parental DNAs, polymerase misincorporation errors, as well as chemical or physical damage to nucleotides. Besides the roles in correcting replication errors, the MMR system was also related to the repair and cytotoxicity of DNA lesions. 21 However, there was insufficient data focusing on the correlation between CDK5 and MMR, and so was the TILs. Moreover, our results failed to confirm the correlation between CDK5 and MMR or TILs. dMMR tumours produced cytosolic DNA by regulating Exo1, which could exert a positive effect on immunotherapy by activating cGAS-STING pathway of tumour cells and dMMR patients generally had a good prognosis.27-29 TILs were lymphocytes that left the blood circulation and migrated to the vicinity of the tumour, including B cells and T cells. For example, cytotoxic T lymphocytes could induce the production of tumour-associated antigens and the cytokine IFN-g. IFN-g played a key role in anti-tumour immunity by inducing cell cycle arrest, differentiation, apoptosis, angiostasis and tumouricida macrophage activity. 30 Dorand 31 reported that CDK5 was involved in the expression of IFN-γ-induced programmed death 1 ligand (PD-L1). In medulloblastoma, 32 CDK5 could specifically regulate the expression of PD-L1 on the tumour surface and played an important role in the tumour immune microenvironment. Activation of PD-1/PD-L1 could lead to the inactivation of immune cells and form an inhibitory TME. In this case, tumour cells could evade immune surveillance and exhibit immune escape. Therefore, knockdown of CDK5 could reduce the expression of PD-L1 and tumour immune escape, suggesting that CDK5 might be a potential target for tumour immunotherapy. TILs have gained momentum as evidence strengthens the clinical relevance of this immunological biomarker. Accumulating evidence suggests that the extent of lymphocytic infiltration in tumour tissue could be assessed as a major parameter by evaluating H&E-stained tumour sections. 26 High TIL levels were associated with favourable outcomes in a real-world immunotherapy cohort of patients with various cancers, such as breast cancer, lung cancer, gastric cancer and other cancers.11-13 TILs have been investigated in various settings in colon cancer, but most studies included heterogeneous study populations with both colon and rectal cancer. Preoperative treatment of rectal cancer with radiotherapy is known to decrease the number of TILs 33 and thus might complicate the interpretation of the prognostic value. A total of 296 patients with colon cancer were enrolled in this study. The TIL ratio was evaluated by H&E staining, and the results were similar to those above. Univariate Analyses indicated that patients with TIL-H had longer PFS and OS. In this study, we used TILs to evaluate the relationship between CDK5 and immunity, but no significant difference was found (P > .05). However, patients with dMMR status were more likely to be Tils-H (P < .05).
Our research still has some shortcomings. First, the expression of CDK5 and the number of TILs were read manually, and the results were subjective and might have errors. Second, the insufficient follow-up time for some patients might affect the results. Finally, there is currently no uniform standard for reading TILs. We evaluated it according to a study in breast cancer, and there might be some bias in the results.
Conclusion
In summary, we suggest that high expression of CDK5 indicates a good prognosis in non-metastatic colon cancer, while low expression of CDK5 indicates a good prognosis in metastatic colon cancer. The expression of CDK5 is unrelated to TILs. Patients with TIL-H have a better prognosis, with a proper cut-off value of 20% for colon cancer.
Abbreviations
CDK5, cyclin-dependent kinase 5; IHC, Immunohistochemical; TILs, tumor-infiltrating lymphocytes; (H&E)-stained, hematoxylin and eosin; OS, overall survival; PFS, progression-free survival; HR, hazard ratio; PD-L1, programmed death 1 ligand; PD-1, programmed cell death protein 1; TME, tumor microenvironment; NCCN, National Comprehensive Cancer Network; RCS, restricted cubic spline; CEA, carcinoembryonic antigen; BMI, body mass index; CSS, cancer-specific survival; MMR, mismatch repair; dMMR, mismatch repair deficiency; pMMR, proficient mismatch repair
Supplemental Material
Supplemental Material - Higher Levels of Tumour-Infiltrating Lymphocytes (TILs) are Associated with a Better Prognosis, While CDK5 Plays a Different Role Between Nonmetastatic and Metastatic Colonic Carcinoma
Supplemental Material for Higher Levels of Tumour-Infiltrating Lymphocytes (TILs) are Associated with a Better Prognosis, While CDK5 Plays a Different Role Between Nonmetastatic and Metastatic Colonic Carcinoma by Qinghua Wang, Ruihua Yin, Xiaoxiao Chen1, Bin Hu, Bingjing Jiang, Wanfen Tang, Xia Zhang, Xiayun Jin, Mingliang Ying, and Jianfei Fu in Cancer Control
Supplemental Material
Supplemental Material - Higher Levels of Tumour-Infiltrating Lymphocytes (TILs) are Associated with a Better Prognosis, While CDK5 Plays a Different Role Between Nonmetastatic and Metastatic Colonic Carcinoma
Supplemental Material for Higher Levels of Tumour-Infiltrating Lymphocytes (TILs) are Associated with a Better Prognosis, While CDK5 Plays a Different Role Between Nonmetastatic and Metastatic Colonic Carcinoma by Qinghua Wang, Ruihua Yin, Xiaoxiao Chen1, Bin Hu, Bingjing Jiang, Wanfen Tang, Xia Zhang, Xiayun Jin, Mingliang Ying, and Jianfei Fu in Cancer Control
Footnotes
Authorship Contributions
Design and drafting the manuscript: Qinghua Wang, Xiaoxiao Chen. Acquisition of data, collection and review of the literature: Ruihua Yin, Wanfen Tang, Xia Zhang, Xiayun Jin. Imaging and pathological evaluation of tumour: Mingliang Ying, Bin Hu, Bingjing Jiang. Critical revision of the manuscript for important content: Jianfei Fu.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by The Key Program of the Jinhua Municipal Science and Technology Bureauu (grant number 2022-3-099); This study was partially funded by the General Project of the Natural Science Foundation of Zhejiang Province (grant number LY19H160020); This study was partially funded by The Key Program of the Jinhua Municipal Science and Technology Bureau (grant number 2019-3-013); This study was partially funded by The Key Program of the Jinhua Municipal Science and Technology Bureauu (grant number 2021-3-080); This study was partially funded by The General Program of the Jinhua Municipal Science and Technology Bureauu (grant number 2022-4-089); This study was partially supported by a grant from the Key Program of Scientific Research of Jinhua Central Hospital (grant number JY2021-1-01). This study was partially supported by a grant from the General Program of Scientific Research of Jinhua Central Hospital (grant number JY2021-2-10).
Ethical Approval
This project and manuscript were reviewed and approved by the Affiliated Jinhua Hospital, Zhejiang University School of Medicine (NUMBER: 2021-20). All studies were conducted with oral consent from patients or their families.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.