
Abstract
Objectives
There is limited guidance on how to effectively educate cancer survivors to adopt and maintain specific diet and physical activity recommendations, especially among underserved and under-resourced populations. Here, the objective is to present the development of a behavioral and theoretically-based multi-modal diet and physical activity intervention program for Hispanic/Latina breast cancer survivors, Mi Vida Saludable (My Healthy Life).
Methods
The development process was based on the 6 steps of the Nutrition Education DESIGN Procedure: (1).
Results
The resulting behavioral intervention consists of 2 components. The first component is in-person group education consisting of 4 lessons over 1 month. Each 4-hour group lesson includes a hands-on cooking component, a physical activity component, and facilitator-led nutrition education and discussion, with 2 field trips to a local grocery store and farmers’ market. The second component is an e-Health program that includes weekly text messages, biweekly emailed newsletters, and ongoing website access.
Conclusion
The systematic DESIGN Procedure provided practical guidance for developing a behaviorally-focused, theory-based, and culturally sensitive program that addresses both dietary and physical activity behaviors for delivery both in-person education and through eHealth. The Procedure may be useful for developing other behaviorally focused and theory-based interventions.
Introduction
Breast cancer is the most commonly diagnosed cancer among women and is the most common cancer among Latinas. 1 While Latinas have lower incidence of breast cancer than woman who are non-Hispanic white, they are more likely to be diagnosed with invasive breast cancer at a younger age and at an advanced stage, and are more likely to die younger than non-Hispanic white women.2,3 These disparities may be due to a number of factors, such as lack of access to medical services and high chronic disease comorbidities, such as diabetes and obesity.
Lifestyle behaviors, including certain dietary patterns (eg, low fruit and vegetable intake, high intake of energy-dense foods) and physical inactivity, are risk factors for breast cancer recurrence. 4 The American Institute for Cancer Research (AICR) states that more than 30% of breast cancer recurrences and deaths are preventable by post-diagnosis lifestyle modifications. AICR and American Cancer Society (ACS) recommendations for cancer survivors include eating a diet high in fruits/vegetables and low in fat and added sugar, and engaging in regular physical activity.4,5 Despite these recommendations, most cancer survivors, including breast cancer survivors, do not meet these guidelines.6,7 Studies have shown that intake of F/V and diet quality can vary across Hispanic subgroups,8-10 as Latina breast cancer survivors include populations stemming from multiple cultural and national backgrounds.11-13 Our prior work has shown low fruit/vegetable intake and low physical activity in Latina breast cancer survivors living in Northern Manhattan.14,15
Simply providing recommendations for improving diet and activity behavior is not sufficient to change and maintain these behaviors long term.16,17 Effective nutrition and physical activity education to support behavior change requires effective motivation and facilitation, including providing environmental supports.16,18-22 Nevertheless, after a breast cancer diagnosis, current clinical practice is typically a brief nutrition consultation with a registered dietitian and/or the provision of educational pamphlets and/or digital materials on diet and nutrition. The availability of nutritional counseling services for breast cancer patients varies across cancer centers and are not reimbursed by many insurance plans. 23 Few culturally-tailored resources and programs exist for Hispanic/Latina populations to improve diet and physical activity, particularly in the Spanish language.
Nutrition and physical activity education programs are more effective if they are systematically developed and administered, behaviorally-focused, theory-based, and culturally tailored.24-26 Moreover, these programs are more effective if they are logistically feasible and tailored for a specific population based on their needs.5,25,26 Intervention frameworks, such as RE-AIM,
27
PRECEDE-PROCEED,
28
the Behavior Change Wheel,
29
Intervention Mapping
30
translate research into practice and are useful for community-based interventions that incorporate individual, educational, environmental and ecological levels of factors. However, these frameworks do not provide practical guidance on the development of specific health education program curricula, group sessions, and materials. The Nutrition Education DESIGN Procedure (DESIGN) was developed to fill this gap.
16
It is unique in that it provides a detailed procedure for designing group direct education (eg, lesson plans for group sessions) and indirect education (eg, handouts, newsletters, recipes, email, online venues) aimed at individual-level behaviors and determinants of change. DESIGN stands for: (1).
DESIGN was used to create ¡Cocinar Para Su Salud! (Cook for Your Health), a culturally-tailored curriculum for Hispanic/Latina breast cancer survivors, which we previously tested in a randomized, controlled trial to examine its effect on increasing fruit and vegetable intake and reducing dietary fat over 6 months.15,36,37 The intervention was based on Social Cognitive Theory 38 and the Transtheoretical Model. 39 Activities and education material targeted increasing self-efficacy and behavioral capability with observational learning and reinforcement through supportive group education and hands-on skills building lessons. Compared to the control group, participants in the 9-session program increased fruit and vegetable intake at 3 and 6 months, and also at 12 months (+2 servings/day) (P < .05 at all timepoints); both groups decreased dietary fat intake at 6 months with no differences between groups. Key determinants of behavior change were self-efficacy and change in taste preferences. 40 Participant feedback and class attendance logs suggested reducing the length of the intervention to improve retention and adherence. In addition, with the rise in the use of electronic media among the Latinx population comparable to the general population, 41 we hypothesized that future nutrition education through such media may address barriers such as time constraints and scheduling conflicts.
This article describes the use of the systematic DESIGN Procedure 16 to modify the nine-session culturally-tailored ¡Cocinar Para Su Salud! curriculum into a program called Mi Vida Saludable (My Healthy Life) with 2 intervention components: direct group education and electronic health (e-Health) communication. The intended audience is Hispanic/Latina breast cancer survivors living in Northern Manhattan and the program was designed to be tested in a National Cancer Institute (NCI) funded 2x2 factorial-designed randomized controlled trial with 4 arms: group education alone, e-Health alone, group education plus e-Health, and control (with the control arm participants receiving all study materials at the end of their participation). 11 Mi Vida Saludable had the same dietary behavior change goals as ¡Cocinar Para Su Salud! which were to increase fruits and vegetables and to decrease foods with excessive fat and sugar. Mi Vida Saludable also added the behavior change goal to increase physical activity.
The group education component of Mi Vida Saludable consisted of 4-hour sessions. Each session included hands-on cooking, physical activity, and facilitator-led nutrition and physical activity education and discussion. Two sessions had field trips, one to a local grocery store and one to a farmers’ market. The number of sessions was reduced from ¡Cocinar Para Su Salud! to determine if fewer sessions could have the same behavior change impacts, as fewer sessions could improve retention and adherence, and facilitate wider implementation.
The e-Health component had the same behavior change goals as the group education component. It used the same psychosocial theory (described in more detail below) and was implemented through text messages, emailed newsletters, and access to a website over 11 months. The goal of testing this intervention component was to determine if this would result in similar behavior change as the in-person group sessions as this could address barriers such as intervention delivery costs, time constraints, and scheduling conflicts, and facilitate broader dissemination.
Description of the program design process for a behavioral research intervention can be useful to guide the development of future behavior-focused, theory-driven, and culturally-tailored group and e-Health education diet and physical activity interventions in breast cancer survivors and other populations.
Methods
Participants
Eligibility criteria for the intended population were self-identified Latinas age 21 years or older with a history of stage 0 to III breast cancer who were ≥ 90 days beyond surgery, chemotherapy, and radiation therapy (current use of endocrine therapy allowed) without evidence of recurrent/metastatic disease. Women were Spanish- or English-speaking, lived in the New York area, and had low intake of daily fruits/vegetables (<5 servings per day) and/or low levels of weekly moderate-to-vigorous physical activity (<150 minutes per week). Women needed to have the ability to receive newsletters, email and/or text messages via computer, smartphone, or cellphone. Technology literacy was not required. From the outset, the research team was aware that the population of Latina breast cancer survivors living in Northern Manhattan is highly diverse in terms of national background, socioeconomic status, and level of acculturation.15,42,43 The intervention was designed to be broadly applicable to this population. Written, informed consent was obtained for participants who engaged in the pilot testing (n = 19). All procedures were approved by the Columbia University Institutional Review Board.
Development Team
The team developing the intervention included public health researchers, education researchers, community health educators, and members of community organizations involved in the delivery of nutrition and culinary education to cancer survivors. The team included research staff and community health educators reflective of the local population, including team members of Dominican, Mexican, Puerto Rican, Colombian, and Peruvian national backgrounds.
Results
Step 1: Decide Behaviors
Step 1 identifies the behaviors to address via the behavioral intervention targeting an underlying health issue. A thorough needs assessment of the intended population and a review of the literature and government and professional association recommendations determine the behavior change goal(s) for an intervention.
Mi Vida Saludable Targeted Behavior Change Goals.

Step 2: Explore Determinants
Step 2 identifies a list of potential determinants (or mediators) of behavior change that could be modifiable influencers of behavior change for the specific behavior change goal(s) and population, including outcome expectations, perceived barriers, self-efficacy, preferences, behavioral capabilities, social support, and action goal setting. Potential determinants are considered as contributors to motivating or facilitating behavior change. Motivating determinants provide inspiration and incentives for behavior change and are typically addressed early in the intervention to raise awareness of risks of the current behavior and benefits of change. Facilitating determinants help people believe they are capable of initiating a behavior change and are typically addressed in an intervention after participants have been motivated to develop specific skills to make behavioral changes. Potential determinants are explored with the population through methods such interviews, focus groups and/or questionnaires to help select the appropriate psychosocial theory in Step 3.
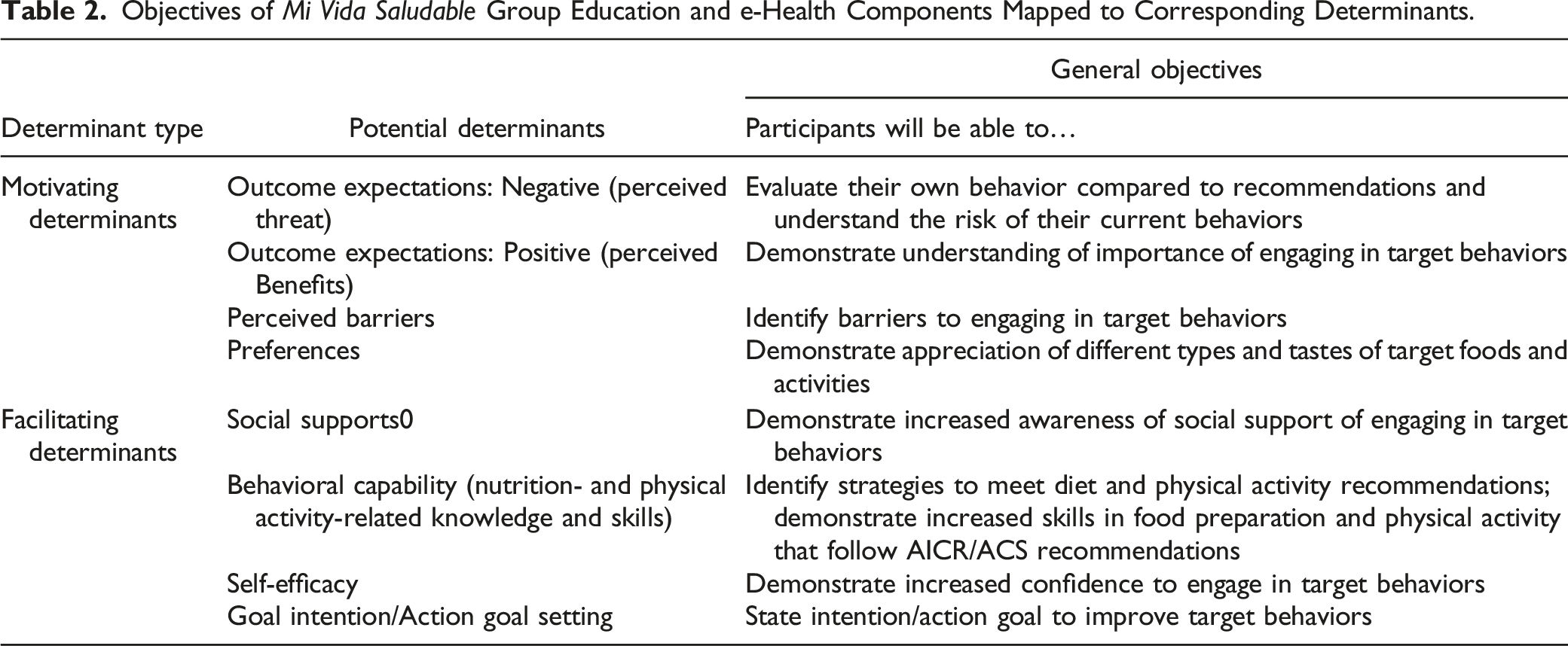
Objectives of Mi Vida Saludable Group Education and e-Health Components Mapped to Corresponding Determinants.
Outcome expectations are physical, social, and/or self-evaluative beliefs about negative outcomes of current behaviors and about positive outcomes or benefits from performing the behavior change goal. 48 Theory-based determinants, including positive outcome expectations (perceived benefits), have been shown to contribute to meaningful changes in diet and physical activity. 46 Thus, in the intervention participants are presented with the benefits of eating more fruits and vegetables and less fat and sugar and increased physical activity to decrease recurrent cancer risk.
Perceived barriers are beliefs about challenges or costs of taking action, and self-efficacy is the level of confidence to successfully carry out the intended behavior. 48 Perceived barriers and self-efficacy are often paired because people increase their confidence in their ability to make behavior changes as they overcome behavior-specific barriers. In the intended population, perceived barriers include family responsibilities and time constraints; preference for “familiar” vegetables and ways of cooking; and the commonly found low-cost “meat packages,” often supplemented with “free” sodas, in their neighborhood stores. 49 To overcome common barriers, during the intervention, participants brainstorm ways to overcome barriers and learn quick and easy healthy cooking methods, how to create culturally-relevant meals, how to access culturally appropriate healthy options at local grocery stores, and how to engage in physical activities that can be done at home and in their neighborhoods. Self-efficacy is increased by being provided appropriate food and nutrition knowledge and guided practice in the targeted behaviors. The ¡Cocinar Para Su Salud! intervention, using such activities, increased participants’ confidence in making healthier dietary choices, and led to increased fruit and vegetable intake up to 12 months,15,40 similar to findings in other diet and physical activity interventions.45,46,50
Preferences are personal inclinations towards specific foods or physical activities, which can be modified by repeated exposures to new tastes, foods, and activities. 16 Taste or food preferences have predicted dietary fat intake among breast cancer patients and survivors. 51 The ¡Cocinar Para Su Salud! trial found that taste preferences for fruit and vegetables mediated increased intake. 40 Consequently, this intervention focused on providing opportunities to try new culturally-relevant foods and modes of physical activity so they could identify and choose those that they enjoy.
Behavioral capabilities refer to the food and nutrition- and physical activity-related knowledge and cognitive and behavioral skills that participants can use to modify their behaviors and maintain the changes in their lives going forward. Thus, the intervention provides participants with knowledge about the AICR/ACS recommendations for diet and physical activity, which foods are low in fat and added sugar, proper portion sizes of foods high in fat and added sugar, and appropriate types and amounts of physical activity. Cognitive skills include estimation of portion sizes of fruits and vegetables and the amount fat in foods and sugar in drinks. Behavioral skills included preparing foods that follow AICR/ACS recommendations learned through demonstrations followed by hands-on skill-building cooking activities with feedback, enhancing food shopping skills through visits to a supermarket and farmers’ market, and increasing physical activity by learning how to use the wearable physical activity tracker given to all participants.
Social support and action goal setting have both been shown to predict physical activity and dietary behavior.45,52 Social support includes emotional, instrumental, information, and appraisal support provided by individuals in social networks to each other. Social support and social networks have been shown to be important in Latino populations53,54 and in similar Latina breast cancer survivor populations with whom we have worked. 55 Social support is incorporated here by creating a safe and supportive group environment56,57 and by participants cooperatively cooking together and eating the meal they have cooked. Goal intention and action goal setting create specific, measurable, attainable, realistic, and time-sensitive goals (ie, SMART goals) in order to achieve behavioral goals. 16 Systematic reviews have found goal-setting, along with attendant self-monitoring, to be one of the most effective components associated with increased physical activity and improved diets.22,47,58 Consequently in this program, participants are taught goal setting skills for specific behaviors or actions and are provided with action planning forms to facilitate the process.
Step 3: Select Theory-based Model
The purpose of Step 3 is to choose a behavior change theory or theories in order to provide a guide for selecting the specific motivating and facilitating determinants to address the targeted behavior changes. These theories are based on research evidence and are applied depending on specific group demographics, group dynamics, and target behaviors.
In the Mi Vida Saludable program, the determinants identified in Step 2 align with Social Cognitive Theory, which posits that behavior is influenced by personal, social, and environmental factors.
20
Recent randomized controlled trials testing dietary and physical activity change in breast cancer survivors broadly use Social Cognitive Theory, with some resulting improvements in fruit and vegetable intake and physical activity.31,33,46 These trials report some description of the educational materials, but have not reported the process by which the curricula were developed. Our previous research in this population
15
found that most of the woman were in the preparation and action stages of change making the Trans Theoretical Model, which focuses on moving participants through the stages, less relevant. Thus, Social Cognitive Theory was selected as the theory-based model (Figure 1). Modified social cognitive theory for Mi Vida Saludable. This figure illustrates the relationship between the proposed motivating determinants and facilitating determinants that result in behavior change as theorized in this intervention. Note: This model is based on Bandura 2004.
20

Step 4: Indicate Objectives
In Step 4, general objectives are specified for each determinant in the theory-based model. General educational objectives are created based on the desired outcome of each determinant. Educational objectives guide the development of the educational plans and activities to support the intended audience in achieving the behavior change goal.
Table 2 outlines the general educational objectives for each determinant in the theory-based model of the Mi Vida Saludable program. These objectives guide the development of content and intervention materials. Educational objectives (“objectives” for short) are learner-based and begin with “Participants will be able to…” followed by an action verb (bolded below). For outcome expectations: negative (perceived threat), the objective was to
Step 5: Generate Plans
The purpose of this step is to create ready-to-use educational plans for group sessions. It starts with the development of a planning matrix that lists each theory-based determinant, along with its attendant behavior change strategies 16 (also called behavior change techniques 24 or methods 30 ), specific educational objectives, and short descriptions of activities sequenced according to educational design principles. 59 This structure ensures that the educational plans systematically create purposeful, and likely more effective, activities that are sequenced according to their theoretical structures for effective delivery. Each educational plan follows 4 sequential phases, denoted as “The Four Es”: first Excite audiences to understand why the behavior change goal is important, then Explain the benefits of the behavior change goal and how to overcome potential barriers, then Expand by practicing and planning how to take action, and finally Exit by creating a clear action goal or plan to achieve the behavior change goal.
The Mi Vida Saludable program created educational plans for the group education component that incorporated interactive group education and hand-on skills building activities adapted from ¡Cocinar Para Su Salud! and for the newly created e-Health education component.
The first task was to create a planning matrix listing each theory-based determinant (from Step 3) along with a behavior change strategy for that determinant. Next, a specific educational objective was written for each determinant. Next, for each component (group education and e-Health) the activities to address the determinant are briefly described. The plans for the group education and e-Health components are described in more detail below.
For the group education component, the activities for each determinant are sequenced according to educational design principles. This structure ensures that the educational plans are sequenced for effective delivery, and follows “The Four E’s” described above. These activities are hands-on cooking, experiential physical activity, discussions about creating action plans for the behavior change goal, and 2 field trips to a local grocery store and farmers’ market.
For the e-Health component, the activities for each determinant included a series of text messages that contained links to newsletters and the bilingual Cook for Your Life website. The text messages were sequenced to address the theory-based motivating and facilitating determinants for each behavior change goal in the same order used in the group education component. The text messages were sent out according to a planned schedule over 11 months. Articles in the newsletters addressed the behavioral determinants, and the Cook for Your Life website provided informational support also addressing the theory-based determinants.
Group Education
Planning Matrix of Session 1 of Mi Vida Saludable Group Education Component.

The first 2 sessions focus on motivating participants to understand and engage in the 4 behavior change goals, while the second 2 sessions focus on facilitating and helping participants engage in adopting the new dietary and physical activity behaviors. All sessions address both motivating and facilitating action determinants, with the first 2 sessions emphasizing motivating determinants and the final 2 sessions emphasizing facilitating action determinants.
Each session begins with an introduction and review of outcome expectations associated with the target behaviors. For sessions 2 through 4, action goals made by each participant at the end of the previous session are discussed to encourage support and revision of action goals as appropriate. Each group session includes both nutrition and physical activity education content, experiential skill building of physical activity behaviors, and culinary and nutrition skill building. Each session emphasizes a different type of physical activity to discuss and experience how more activity can easily be included throughout the day. The culinary and nutrition segments focus on different behavior change goals. The first session emphasizes motivational determinants for decreasing fat and added sugar, the second increasing fruit and vegetable intake, and the third and fourth sessions focus on facilitating determinants for all 3 diet behavior change goals. Sessions 1 and 2 teach main concepts in the classroom. Sessions 3 and 4 include tours of a local affordable grocery store and a farmers’ market. The last segment of each session involves culinary education, where women cook culturally relevant recipes. After cooking, the women eat a meal together to facilitate support and confidence in skills. Sessions conclude with women brainstorming ways to troubleshoot barriers to completing the target behaviors. Women complete action goal-setting worksheets for each target behavior.
e-Health
Examples of Text Messages That Address the Theory-Based Determinants of Behavior Change.

Results from text message-based lifestyle interventions have shown that best practice is to provide more text messages at the beginning of the intervention then decrease the text message frequency. 60 Thus, the number of text messages slowly decreases from 5 to 2 messages a week over the 11-month period. Text and email messages are bidirectional, allowing study staff to respond to participants.
The text message content parallels the group education content. Half of the text messages focus on diet (ie, increasing fruit and vegetable intake, and decreasing fat and added sugar intake) and half focus on physical activity (ie, increasing minutes of weekly physical activity). Once a month, text messages prompt women to set action goals, half related to diet and half related to physical activity. The women to respond to a goal setting question (eg, “Make a goal: How often do you think you can choose a low-fat meat such as 90-95% lean ground meat or chicken without the skin this week? Text back your response: 1 = 1 time per week, 2 = 2 to 3 times per week, 3 = almost every day, 4 = every day.”) 1 week after these action goal-setting messages are sent, another message asks for feedback (eg, “Remember, last week we asked you to set a goal to eat less fat from meat or chicken this past week? How many times did you do it? Text back your response. 1 = 1 time this week, 2 = 2 to 3 times this week, 3 = almost every day, 4 = every day.”) This interactive approach encourages engagement and self-monitoring, which can lead to more sustained behavior change. 61
E-newsletters are delivered via links embedded in text and email and are stored on a secure location on the bilingual Cook for Your Life website only accessible to study participants (www.cookforyourlife.org). (At the initiation of the research period, Cook for Your Life was a non-profit organization that provides nutrition education and cooking classes to cancer survivors in New York City; it has since closed and the Cook for Your Life website in now run out of the Fred Hutchinson Cancer Center.) Half of the newsletters’ content target diet and half target physical activity, with colorful and topical content aligning with the topic of the week and the behavior change being targeted. Each newsletter begins with a welcoming introduction from a member of the study staff and includes motivating and facilitating nutrition or physical activity information. In addition to newsletters, other links sent via text messages include links to Cook for Your Life recipes, dance videos from the local non-profit Moving for Life™ (movingforlife.org), and New York City government sponsored events promoting physical activity.
Pilot study of program before final curriculum completion
The group education program followed by a shortened version of the e-Health program was piloted with a small sample of breast cancer survivors (n = 19) for user testing and to receive participant feedback on the intervention. Changes to the materials were made based upon feedback received. After the pilot study was completed, a formative evaluation of the intervention was conducted. On a scale of 1 to 5 where 5 indicates greatest satisfaction, participants were very satisfied with both group education and eHealth portions of the intervention (range of mean responses was 4.8 – 5.0 for group education and 4.0 – 4.8 for e-Health). Major changes to the group education component included the addition of evidence-based information on common questions about fad diets. Logistical changes focused on field trip transportation to and from the grocery store and farmers’ market, and when and where meal and snack preparation should take place for each session.
Translation
Of note, this intervention was designed to be conducted in both Spanish and English, which meant that all materials needed to be available in both languages. A bilingual, multi-cultural, and multi-disciplinary team was assembled, including one certified translator, to translate the written patient-facing materials (print and digital) and curriculum into Spanish and to review the translation for accuracy. Multiple sessions were used to refine and edit the translations to make sure that meaning was not lost in the translation process. As it was known in advance that the majority of the intended population would be Spanish-speaking, the in-person sessions were designed to be delivered by the health educators in Spanish with simultaneous live translation in English offered to participants who preferred to listen/participant in English. Participants opting for delivery in English listened with headsets while the onsite certified live translator provided translations. This arrangement allowed for participants and staff to request any translation clarifications as needed.
Step 6: Nail Down Evaluation Plan for the Education Program
This final step is to create the evaluation plan. Designing the evaluation plan at the same time as the intervention ensures appropriate methods are used to measure changes in the behavioral determinants and changes in the specific behavior change goal(s). Measuring changes in both determinants and behaviors can help elucidate mechanisms of behavior change and provide guidance on designing future interventions.
For Mi Vida Saludable, an evaluation plan was created to test the effectiveness in a 2x2 factorial-designed randomized controlled trial (RCT). Data are collected on the primary diet and physical activity outcomes at baseline, 6-, and 12-months. Dietary intake is assessed using 2 to 3 24-hour recall assessments using the multiple pass approach using the Nutrition Data System for Research (NDSR) developed by the Nutrition Coordinating Center at the University of Minnesota. Physical activity is assessed using the a 7-day physical activity recall (7DPAR). 62 A questionnaire to measure changes in Social Cognitive Theory behavioral determinants was developed and validated (Koch et al, manuscript in submission). The evaluation results will identify the most important determinants of diet and physical activity change for this population, which will have implications for future research and practice.
Discussion
The Mi Vida Saludable intervention consists of a four-session, 1-month nutrition and physical activity group education component and an 11-month e-Health component focused on improving diet and physical activity in Hispanic/Latina breast cancer survivors. Both components were created using the 6-step DESIGN Procedure. The Social Cognitive Theory based intervention targets 4 key behaviors: (1) increase daily fruit and vegetable intake, (2) decrease percentage of daily calories from dietary fat, (3) decrease percentage of daily calories from added sugar, and (4) increase daily minutes of moderate to vigorous physical activity. While DESIGN has previously been used in other settings, 63 this is the first study that we are aware of to develop and test a theory-based educational program with similar content for both in-person group education and e-Health formats and for both diet and physical activity. This is also one of the first studies to use, and describe in detail, a systematic curriculum development process to develop such a program for a racial/ethnic minority population with a specific health concern.
The systematic DESIGN approach to curriculum development is unique in that while several other systematic procedures provide frameworks for translating behavioral theory into practice,29,64 they not to provide specific practical guidance on the next necessary step of how exactly to create educational behavior change activities and sequence them appropriately for individual sessions or for indirect venues such as electronic media. DESIGN fills this need by using effective instructional design theory from the field of education, accompanied by communication principles, to structure and sequence activities into actual ready-to-deliver educational plans. The novel DESIGN planning matrix shown in Table 3 in particular helps with this process. It provides a clear delineation of how determinants of behavior change derived from a clearly stated theory drive the development of activities through the selection of appropriate behavior change strategies (or techniques or methods), and the writing of specific educational objectives. The matrix also shows how given sessions are sequenced according to education principles. 59 This study shows that DESIGN can be used for planning sessions addressing both diet and physical activity behaviors.
e-Health approaches to intervention have become widely used. They are generally based on tailoring content to individuals based on psychosocial, psychographic, and related variables.60,65 This study adds to the literature on the use of e-Health by showing how to use a systematic design procedure to facilitate the creation of e-Health text messages and e-newsletters based on a theory-based model and education principles to be delivered as a structured program addressing both dietary and physical activity behaviors. In addition, the schedule of delivery of text messages used educational theory principles, in particular sequencing the motivational messages early in the intervention and facilitating messages later in the intervention.59,66 E-Health approaches may be particularly beneficial as they have the potential to overcome the problem of time constraints and scheduling conflicts and may be more scalable than in-person interventions. 39 The only e-Health nutrition and physical activity intervention for Latina breast cancer survivors identified to date was based on a smartphone app used by participants over a 6-week period along with 3 telecoaching calls based on motivational interviewing.67,68 The content of the app was primarily straightforward instruction on managing symptoms, medications, emotions, family, and friends. The study described here shows that the DESIGN procedure can be used to develop theory-based education through both remote e-Health and in-person group sessions.
There are potential benefits to use of the DESIGN Procedure. The literature has shown that behavioral interventions are more effective if they are behaviorally-focused, theory-based, and directly address the determinants in the theory.16,26 Further, as diet and physical activity behaviors are complex, DESIGN allows program developers to create a theory-based model specific to a certain behavior for the audience. In addition, DESIGN calls for creating evaluation methods that specifically measure changes in behaviors and psychosocial theory determinants targeted by the intervention. The Mi Vida Saludable curriculum within each session and over the 4 sessions moves from motivating behavior change to facilitating decisions on new nutrition and physical activity behaviors. A distinction of the Mi Vida Saludable program is the cultural integration of the local Latina breast cancer survivor population from conception to execution of the intervention, following behavior change theory, both via in-person group education and e-Health communication.
Translating theory-based determinants into educational objectives, and then identifying evidence-based behavior change strategies and activities, allows researchers to develop similar programs across demographic groups and across various behavior change goals, and to compare outcomes consistently across populations.16,66 The methods by which behavior change curricula for cancer survivor populations are developed have rarely been described in detail, which prevents researchers from systematically building upon prior work. Culturally based and adapted programs are important for effectiveness and recommendations have been made for features to consider in developing such programs.25,35,69,70 The description of a systematic procedure to provide guidance for developing culturally-tailored or culturally specific educational programs for racial/ethnic minority populations has not been found, and there are limited education resources for Hispanic/Latina groups.
This description of the development of Mi Vida Saludable makes several contributions. First, Mi Vida Saludable provides guidance for developing future behavior change interventions with cancer survivors. Second, Mi Vida Saludable provides an example of an intervention that is culturally sensitive to ensure Hispanic/Latina women feel connected in terms of language and community, which has been shown as a strong desire among this group. 71 Third, Mi Vida Saludable demonstrates how to develop complementary interventions using different mediums (ie, electronic and classroom based that address the same behavior change goals and theory-based determinants). In particular, the use of theory-based determinants of behavior change to guide the development of e-Health content and sequencing can inform future technology-delivered intervention programs targeting lifestyle behaviors among Latina breast cancer survivors. Practitioners designing brief interventions can use an abbreviated version of the DESIGN Procedure. 16
Despite these strengths and contributions, there are potential limitations to this approach. To maximize generalizability, the intervention was designed for any Latina breast cancer survivor with non-metastatic disease post-diagnosis and post-treatment. If women are more likely to make changes based on stage at diagnosis or time since diagnosis, this intervention was not designed to address this. In addition, at the time this intervention was developed, there was little data upon which to base the frequency and content of the text messaging intervention 60 ; one of our goals was to use the methods and data generated from this research to help fill this gap.
When behavioral interventions are developed without describing their developmental process, replication and identification of effective strategies to address theory-based determinants are difficult. With a clear description using a systematic process, researchers and practitioners are able to conserve resources and move the field of behavior change forward more quickly and effectively. Further research can enhance the utility of the DESIGN procedure by investigating which components of the DESIGN Procedure are the most effective.
Conclusion
This detailed description of the development of MiVS shows how the systematic DESIGN Procedure can provide practical guidance for developing a behaviorally-focused, theory-based, and culturally sensitive program that addresses both dietary and physical activity behaviors. DESIGN creates a ready-to-deliver program by integrating nutrition and exercise science to determine the behaviors to address and content to include, psychology to select the theory-based model and determinants, educational theory to sequence activities, and communication theory for effective implementation. The DESIGN Procedure can be used to develop a program with similar behavior change goals, theory-based determinants, and content for both in-person group education and e-Health formats, thus permitting wide dissemination of a program. This procedure provides guidance for developing future behavior change interventions with persons who have survived cancer.
Supplemental Material
Supplemental Material - Developing a Diet and Physical Activity Intervention for Hispanic/Latina Breast Cancer Survivors
Supplemental Material for Developing a Diet and Physical Activity Intervention for Hispanic/Latina Breast Cancer Survivors by Isobel Contento, Rachel Paul, Amanda M. Marin-Chollom, Ann Ogden Gaffney, Heewon Gray, Anne M. Haase, Dawn L. Hershman, Pamela Koch, Heather Greenlee in Cancer Control
Abbreviations
ACS American Cancer Society
AICR American Institute for Cancer Research
DESIGN Decide behaviors, Explore determinants, Select theory-based model, Indicate objectives, Generate plans, and Nail down evaluation; NCI, National Cancer Institute
NDSR Nutrition Data System for Research
PRECEDE Predisposing, Reinforcing, and Enabling Constructs in Educational Diagnosis and Evaluation
PROCEED Policy, Regulatory, and Organizational Constructs in Educational and Environmental Development
RCT Randomized controlled trial
RE-AIM Reach, Effectiveness, and Maintenance, and Adoption, Implementation, and Maintenance
7DPAR Seven-day physical activity recall
Footnotes
Acknowledgments
We thank Martha Eddy, PhD of Moving For Life for her contributions to the physical activity component of the in-person group dance class. We thank Cynthia Thomson, PhD, RD, Tracy Crane, PhD, and Hagen Frank at the University of Arizona for their contributions in developing the platform to deliver the electronic communication program. We also thank Gramercy Global for developing and managing the ![]() website. We thank Fitbit for providing Fitbit Zips to study participants.
website. We thank Fitbit for providing Fitbit Zips to study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the National Institutes of Health National Cancer Institute (R01CA186080), National Center for Advancing Translational Sciences (UL1TR000040 and UL1TR001873), and Herbert Irving Comprehensive Cancer Center (HICCC) Avon pilot study funding.
Ethical Approval
Ethical approval to report this case was obtained from the Columbia University Institutional Review Board (Protocol ID AAAP0461).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Columbia University Institutional Review Board (Protocol ID AAAP0461) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.