
Abstract
Objective
In this article on adenoid cystic carcinoma (ACC) of salivary gland, we intend to summarize the causes of misdiagnosis and oversight of ACC hoping to improve cytological diagnostic accuracy, clinical management and patient treatment.
Methods
The study retrospectively reviewed 32 patients with ACC of salivary gland, registered at the Affiliated Hospital of Southwest Medical University from July 2014 to June 2021. These cases were diagnosed by FNA and surgical excision biopsy. All cytopathological results were retrospectively categorized according to Milan system for reporting salivary gland cytopathology (MSRSGC). The accuracy of FNA was verified by surgical excision biopsy.
Results
Of these 32 patients, 16 (50.0%) cases were male, and 16 (50.0%) were female. Their age ranged from 21 to 79 years, with an average age of 50.32 years. The highest incidence (15/32, 46.9%) of ACC was observed in patients between 41 and 50 years of age. 10 cases (31.3%) occurred in the parotid gland, 9 cases (28.1%) in the submandibular gland, 9 cases (28.1%) in the sublingual gland, 3 cases (9.4%) in the palate, and 1 case (3.1%) in the lip. Among the 32 cases of ACC, 23 cases (71.9%) were classified to VI, 4 cases (12.5%) to IVa, and 5 cases (15.6%) to II by MSRSGC. A comparison of the FNA results with biopsy showed that the accuracy of FNA in ACC of salivary gland is 71.9%. Being able to identify the cytomorphological features is the key factor for accurate diagnosis of ACC of the salivary gland.
Conclusion
Our results confirm that FNA is an important initial screening in the diagnosis of ACC of salivary gland. Increased study of the cytomorphology of ACC is beneficial for more accurate diagnosis of ACC, to reduce misdiagnosis and oversight.
Introduction
Adenoid cystic carcinoma (ACC) is a malignant tumor that accounts for less than 10% of salivary gland tumors.1,2 It is the most common malignant neoplasm of the minor salivary glands.3-5 The characteristics of ACC include slow growth, early perineural invasion, frequent distant metastasis, and potential local recurrence.6,7 Once metastatic ACC is present, case series of salivary gland ACC suggest that the median survival is about 3 years. Although it was shown that complete surgical resection and additional radiotherapy improve long-term survival, the prognosis of ACC remains poor.8,9 Therefore, early and accurate diagnosis of ACC of the salivary gland is crucial.
Fine needle aspiration (FNA) cytology is a widely accepted, simple, economic, rapid, safe and relatively non-traumatic procedure that can provide a rapid initial diagnosis. The advantage of FNA is that it can be performed in an outpatient setting with low risk of complications. A potential disadvantage of FNA is the possibility of varying results in the distinction of malignant and benign disease and variable rates of non-diagnostic and indeterminate cytology.10-12 The sensitivity and specificity of FNA in differentiating neoplastic and non-neoplastic lesions were 79-100% and 71-100%, regarding the differentiation of benign and malignant tumors were 82% and 95%, respectively.13,14
FNA has become a commonly performed and clinically very useful diagnostic tool in the initial evaluation of masses of the major salivary gland. Therefore, this study retrospectively analyzed and summarized 32 cases of ACC of the salivary gland in order to discuss the causes of misdiagnosis and oversight of ACC in cytology FNA. All cases were diagnosed by FNA and confirmed by surgical resection biopsy from July 2014 to June 2021 in the Affiliated Hospital of Southwest Medical University.
Materials and Methods
Patients
The cytological results of 32 patients with salivary gland mass who underwent FNA in the Affiliated Hospital of Southwest Medical University from July 2014 to June 2021 were collected. In these 7 years, 58,487 patients were punctured and the rate of ACC of the salivary gland was 0.05%. The gender and age of all patients were retrospectively analyzed, and biopsy pathology and postoperative pathological results were compared with the primary cytological results. This study protocol was reviewed and approved by the guidelines of the Institutional Ethics Committee of the Affiliated Hospital of Southwest Medical University (approval no.2022223), Luzhou, China. All patients provided written informed consent prior to enrollment in the study.
Fine Needle Aspiration Biopsy Diagnosis
After obtaining the written informed consents of the patients, FNA operations were conducted for each subject after palpation. FNA procedures were performed by cytopathologists using a 23-gauge needle attached to a 10 ml plastic syringe (Becton Dickinson, S.A., Spain) with more than 10 needle insertions, and hematoxylin and eosin (H&E) staining. The cytological diagnosis was made by 2 experienced and board certified cytologists (WSH and LY). The results were evaluated according to the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC), published in 2018. 15
The FNA-based diagnosis was compared to the results of surgical excision biopsy. If FNA wrongly showed a benign tumor instead of an ACC, it was counted as misdiagnosed. If the FNA wrongly showed a benign tumor instead of an ACC, but the patient still received early standardized treatment, it was recorded as oversight.
Statistical Analyses
All statistical analyses were performed to calculate the diagnostic accuracy of the FNA method compared to histopathological assessment for salivary gland mass. Surgical biopsy specimens served as controls. Enumeration data were expressed as percentage. All data analyses were performed using SPSS 16.0 software (SPSS, Inc., Chicago, IL,USA).
Results
Patients’ Characteristics
Characteristics of 32 Patients with ACC.

Cytopathological Diagnosis of Adenoid Cystic Carcinoma
Cytomorphological features of ACC from FNA smears: Neoplastic ductal cells were distributed in three-dimensional clusters, solid sheets or single scattered. Cells are relatively small, uniform in shape, similar to basal cells, round, oval, and sparse in cytoplasm. Cellular atypia were not evident, only small nucleoli were visible. The nuclear staining is deep, the nuclear chromatin is coarse or slightly coarse, and the distribution is uneven; the nucleus is slightly enlarged, and the size is different; the shape of the nucleus is irregular to varying degrees (usually mild), and mitotic figures are rare (Figure 1). The hyaline membrane globules are transparent, cylindrical or barrel-shaped and surrounded by palisade-like tumor cells. This kind of spherical transparent substance is caused by myoepithelial cells secreting proteoglycan, which is the unique structure of this tumor and has diagnostic significance. Cytological FNA aspirates consist mainly of 2 components: epithelial cells and hyaline membrane globules. The 3 major growth patterns of salivary gland ACC are tubular, cribriform and solid. Classic adenoid cystic carcinoma. Basal-like tumor cells in a cribriform arrangement. A-C Cytopathology, D Histopathology (H&E). Magnification is indicated by scale bar.
Results of Salivary Gland Mass Based on Smears
Of these 32 patients, in 23 cases a malignant tumor was diagnosed (VI), in 4 cases a benign tumor (IVa), and in 5 cases a benign lesions (II) by cytology.
Accuracy of FNA by MSRSGC
Among these 32 cases the results of FNA cytology were compared to histopathological diagnosis, which revealed 23 (71.9%) correctly diagnosed cases, 4 (12.5%) misdiagnosed cases and 5 (15.6%) overseen cases.
Discussion
ACC is a highly malignant but usually slow growing solid salivary gland tumor. Although the cytological features of ACC are well described in literature,16-26 the exact correlation between the primary cytological reports and the final histological diagnosis is about 63% to 71% respectively. The causes of misdiagnosis and oversight in FNAs of ACC of the salivary gland have not been evaluated in detail. Our research shows that the accuracy rate of ACC diagnosis of salivary gland is 71.9%, which is basically consistent with the results reported earlier. 27 We have carefully analyzed the causes of misdiagnosis and oversight of ACC based on our research results. 4 cases (12.5%) were misdiagnosed from the cell morphology and arrangement as benign tumors (IVa), 2 cases were further misdiagnosed as pleomorphic adenomas (PA), and 2 cases were misdiagnosed as basal cell adenomas (BCA). 5 cases of small masses of the salivary gland were overlooked as benign lesions.
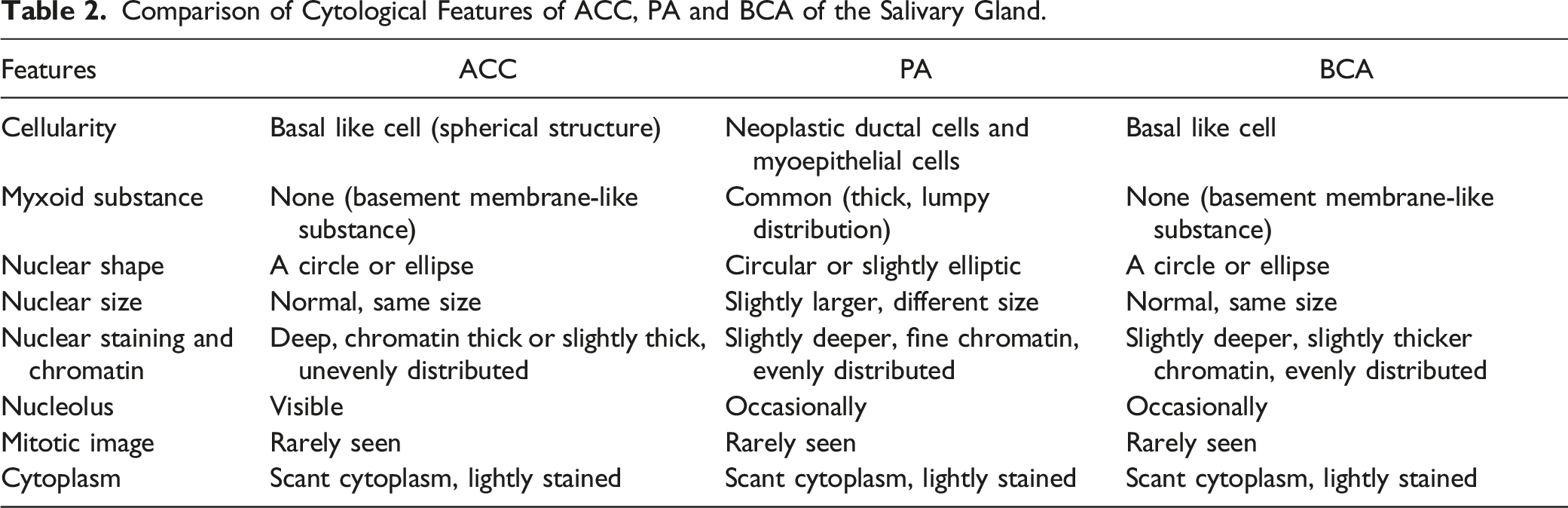
The first case was a 46-year-old male with a mass in the left parotid region. The size of the mass was 3.0 cm, medium in texture and relatively well defined. The patient had no typical clinical manifestations like pain. The collective staff of the department observed the FNA smear again under the microscope. The smear showed strongly demarcated, rounded clusters of basaloid epithelial cells with uniform, round or oval nuclei and scant cytoplasm, and some of the cells were arranged around globules of homogeneous, acellular material (Figure 2, (A)-(D)). The misdiagnosis of this case was due to the cytopathologist’s inexperience in diagnosing ACC at that time. Case 2 was a 53-year-old female with a swelling behind her ear that had recently increased in size. Imaging showed a 3.8 cm parotid mass. The patient complained of swelling of the mass. Cytologically, the glandular epithelial cells were crowded, the chromatin was unremarkable, and prominent nucleoli were missing, a few cells like spindle myoepithelial cells were seen in the background of the smear. In addition, the salivary gland is the most common site for PA, so ACC was misdiagnosed as PA. The cytological characteristics of PA are that the glandular epithelial cells are aggregated in down-like or filamentous mucus, and the myoepithelial cells are arranged in bundles or staggered patterns. Both aspirates with discordant results, where the specific relationship between epithelial cells and extracellular matrix was not recognized in the specimens, were misdiagnosed as PA. Comparison of cytological features of ACC and PA of the salivary gland is shown in Table 2. Misdiagnosis of adenoid cystic carcinoma as pleomorphic adenoma. A-C Cytopathology, more epithelial cells and myxoid material first associated with pleomorphic adenoma. D Histopathology (H&E). Magnification is indicated by scale bar. Comparison of Cytological Features of ACC, PA and BCA of the Salivary Gland.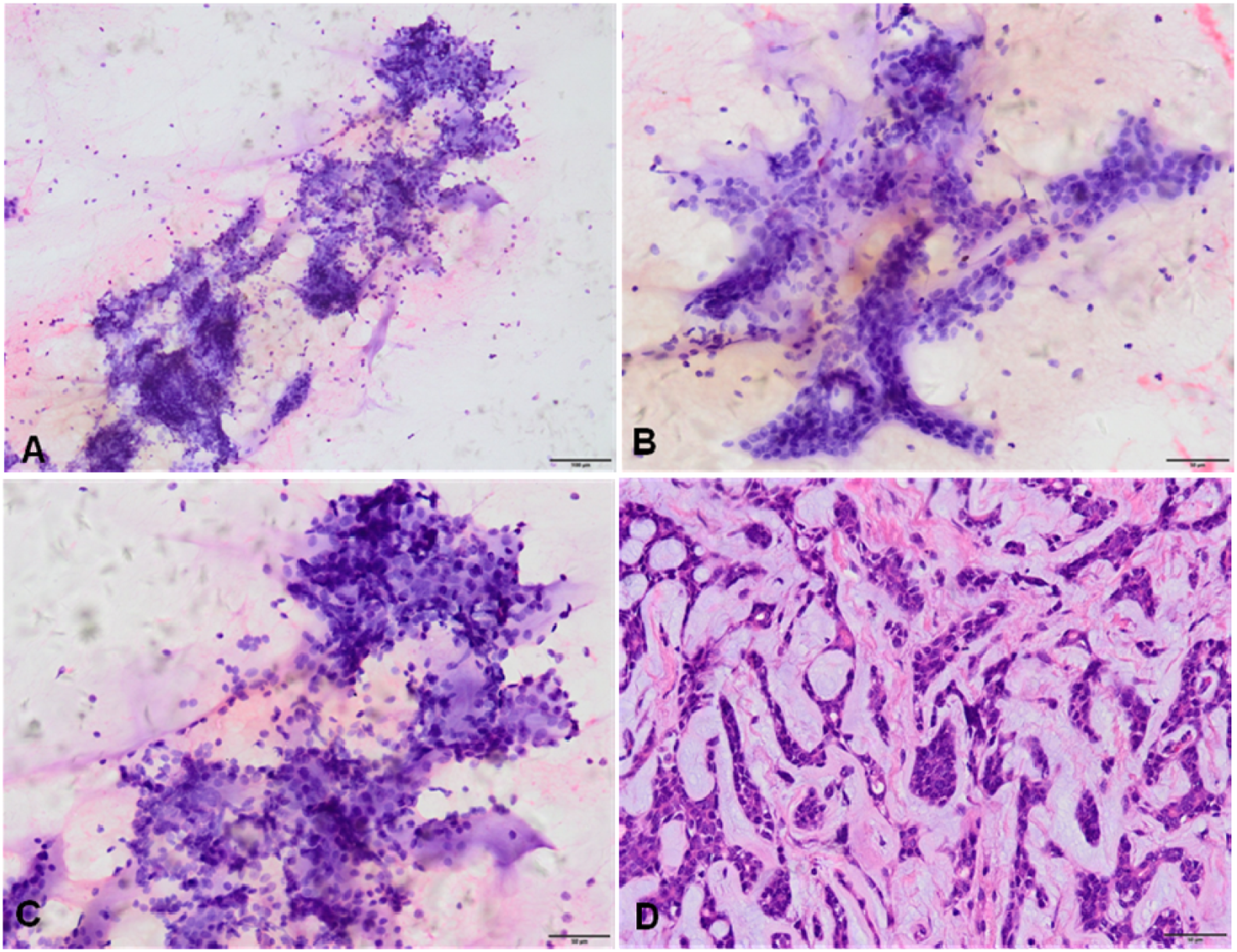
Although there are some distinct cytomorphological features which help in discriminating the 2, still both can be confused with each other and therefore misdiagnosed. It is not easy for cytologists to clearly distinguish the 2 entities especially with atypical cell arrangement or due to inexperience.28-30 Fortunately, the ancillary techniques like immunohistochemistry (IHC) and molecular studies improve the distinction between ACC and PA. A p63+/p40-immunophenotype that can help distinguish it from ACC and PA. 31 Strong nuclear staining for MYB is valuable for cytological diagnosis of ACC,32,33 thus these patients may be amenable to Imatinib therapy. Fusion of MYB-NFIB and MYBL1-NFIB are altered in ACC, alteration of PLAG1 and HMGA2 in PA. 34 β-Catenin plays an important role in the pathogenesis of PAs and ACCs in salivary glands. 35
Two cases of ACC were misdiagnosed as BCA by FNA. The first case was a 42-year-old woman with a 3.0 cm mass in the right parotid gland. The second patient was also female and had a 1.3 cm mass in the left submandibular gland. Both patients were presented due to self-palpation of masses without other discomfort. The cellular smear consisted mainly of small homogeneous basal-like cells, arranged in a flat or beam shape. Scattered lymphocytes and glandular epithelial cells were seen in the background (Figure 3, (A)-(D)). Histopathological assessment of biopsy and resection specimens confirmed a solid ACC. It is often difficult to differentiate ACC and BCA, using only cytological diagnostics. Table 2 shows a comparison of cytological features of ACC and BCA of the salivary gland. The nuclei of BCA cells stained light or slightly dark, with regular shape, uniform size, no atypia, smaller and more slender than those of ACC, no nucleoli or inconspicuous small nucleoli, and the cytoplasm of tumor cells was more abundant and translucent than that of ACC. Hyaline membrane globules are rare. Misdiagnosis of adenoid cystic carcinoma as basal cell adenoma. A-C Cytopathology, homogeneous basal-like tumor cells arranged in a flat or beam shape. D Histopathology (H&E). Magnification is indicated by scale bar.
Cytological results of 32 Patients with Salivary Gland Mass.

Conclusion
Determining the nature of salivary gland masses is of great importance. Accurate diagnosis of ACC allows patients to receive timely treatment. FNA is a quick method that usually, but not always, helps to find a definitive diagnosis. The MSRSGC facilitates clearer communication between cytologists and treating clinicians and enhances inter-institutional communication. The study showed that the accuracy of FNA in diagnosing ACC of salivary gland was 71.9%. The results confirm that FNA is an important initial screening method for ACC, but cytologists should be aware of the possibility of misdiagnosing ACC as PA and BCA, as well as the possibility of small ACC masses being overlooked. Strengthening the study of ACC cytomorphology is helpful to make a more accurate diagnosis, IHC and molecular studies can be carried out when necessary.
Footnotes
Author Contributions
HCG and LMZ made major contributions to the data analysis and manuscript writing. WSH collected the data and participated in writing the manuscript. LY participated in collecting data. ZHL collected data and figures. JH participated in writing and revising the manuscript. All authors discussed, carefully read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the joint project of department of technology of Luzhou, Southwest Medical University (2017LZXNYD-T04).
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
This study was approved by the Medical Ethics Committee of Southwest Medical University (approval no.2022223), Luzhou, China. 32 patients’ written informed consents were obtained before FNA.