
Abstract
Introduction
The COVID-19 pandemic has disrupted many aspects of clinical practice in oncology, particularly regarding early cancer diagnosis, sparking public health concerns that possible delays could increase the proportion of patients diagnosed at advanced stages. In 2009, a cancer fast-track program (CFP) was implemented at the Clinico-Malvarrosa Health Department in Valencia, Spain with the aim of shortening waiting times between suspected cancer symptoms, diagnosis and therapy initiation.
Objectives
The study aimed to explore the effects of the COVID-19 pandemic on our cancer diagnosis fast-track program.
Methods
The program workflow (patients included and time periods) was analysed from the beginning of the state of alarm on March 16th, 2020 until March 15th, 2021. Data was compared with data from the same period of time from the year before (2019).
Results
During the pandemic year, 975 suspected cancer cases were submitted to the CFP. The number of submissions only decreased during times of highest COVID-19 incidence and stricter lockdown, and overall, referrals were slightly higher than in the previous 2 years. Cancer diagnosis was confirmed in 197 (24.1%) cases, among which 33% were urological, 23% breast, 16% gastrointestinal and 9% lung cancer. The median time from referral to specialist appointment was 13 days and diagnosis was reached at a median of 18 days. In confirmed cancer cases, treatment was started at around 30 days from time of diagnosis. In total, 61% of cancer disease was detected at early stage, 20% at locally advanced stage, and 19% at advanced stage, displaying time frames and case proportions similar to pre-pandemic years.
Conclusions
Our program has been able to maintain normal flow and efficacy despite the challenges of the current pandemic, and has proven a reliable tool to help primary care physicians referring suspected cancer patients.
Highlights
Our Cancer Fast Track program (CFP) easily connects general practitioners and hospital specialists. Our CFP shortens waiting times in patients with suspected cancer, enhancing quality of care. Our CFP has maintained normal flow and efficacy despite the challenges of the current pandemic.
Introduction
Cancer continues to be among the main causes of morbidity and mortality in the world. 1 Recognition of cancer warning symptoms may prompt physicians to refer patients to specialists in order to achieve early diagnosis. Maintaining the correct timing for diagnosis and treatment is crucial and requires an adequate integration of all available resources.2,3 In Europe, patients with warning symptoms of cancer often consult their primary care (PC) physicians 4 as the first step to distinguish suspected symptoms of malignancy from those not suggestive of cancer. To provide a coordinated, efficient and affordable solution to this issue and to improve communication between primary and specialized medicine, a cancer fast-track programme (CFP) was launched in our healthcare area (Clinico-Malvarrosa Health Department) in 2009. This programme was designed to promote cooperation between PC and different hospital specialists and thus shorten waiting times between recognition of cancer-related symptoms to diagnosis and initiation of appropriate therapy. 5 Data published over the 10 years of this program show that patients consulting their general practitioners (GPs) with suspected cancer are evaluated by the corresponding specialist in less than 15 days, with a median of 3 days to histopathological diagnosis and 34 days to treatment initiation from their first appointment at the GP. 6
The coronavirus disease 2019 (COVID-19) pandemic was first documented in Spain on January 31th, 2020. On March 14th, the Spanish Government decreed a nationwide state of emergency and approved the population lockdown. On March 28th, all non-essential face-to-face work activities were avoided for 15 days. In Spain, up to six waves have been declared to date and it has been estimated more than 100 000 deaths due to the COVID-19 pandemic (www.lamoncloa.gob.es). In PC centres, patients were attended by phone during the pandemic, and only emergency cases were evaluated by face-to-face visits. In hospitals, face-to-face appointments to outpatient clinics were restricted to patients with suspected oncological conditions to avoid delayed diagnoses; the remaining consultations were carried out by phone. Therefore, CFP could be the perfect tool for maintaining optimal diagnosis flow.
The present study was carried out to evaluate any pandemic-related changes occurring between March 16th, 2020 to March 15th, 2021 in the number of referrals sent from PC to the CFP, waiting times for hospital specialist assessment or time to cancer diagnosis.
Materials and Methods
The program was launched in June 2009 in the Clinical-Malvarrosa Health Department of Valencia (CMH), an area covering 33 primary care centres serving a population of around 345 026. 7 The main objective of the CFP was to reduce waiting times between patient consultation with suspected neoplasia and assessment by the corresponding specialist. To speed up cancer diagnosis and treatment initiation in this setting, suspected cancer guidelines were initially developed for GP use for referring patients with suspected breast, colorectal, cervical, lung, bladder or otorhinolaryngological cancer. In order to assess lymph nodes and constitutional syndrome, additional areas were incorporated into the program. The initial goal of the CFP was that all patients included in this workflow had to be assessed by a specialist in less than 15 days.
We performed an observational, ecological descriptive study. We assessed how the CFP was performed during the worst year of the COVID-19 pandemic (March 2020 to March 2021) and compared with data from previous year (from march 2019 to march 2020). We also assessed if patients with suspicious cancer symptoms that were included in the CFP were evaluated by corresponding specialists within 15 days. We also investigated if PC phone appointments had led to an increase in CFP patient referrals with less well-founded oncological symptoms suspicion. Data was collected for this purpose from all patients referred by GPs with suspected cancer from March 2019 to March 2021. The variables studied were: referral date, first specialist evaluation date, diagnosis date, type of cancer diagnosed, treatment initiation date and tumour stage at diagnosis. This study was approved by the clinical research and ethics committee of University of Valencia, Spain (approval number 2020/312) with waiver of the informed consent.
All data were registered in a Microsoft Access database to facilitate subsequent evaluation and comparison between the 2 study years. Statistical analysis was performed using R software, including chi-square and Wilcoxon tests.
Results
We compared data between the year before the COVID-19 outbreak, from March 16th, 2019 to March 15th, 2020 (year 1) and the first pandemic year, from March 16th 2020 to March 15th, 2021 (year 2).
A total of 895 and 975 patients with suspected cancer were referred through the CFP by their GP during years 1 and 2, respectively.
During year 2, 66 referrals (6.8%) failed to meet acceptance criteria, compared with 34 (3.8%) during the previous year (P < .05). A similar percentage of referrals were lost to follow-up across the 2 cohorts: 86 (10%) in year 1 and 90 (9.9%) in year 2.
During year 2, 198 patients (24.1% of all specialist-studied referrals) were diagnosed with cancer, compared to 176 patients (22.7%) during year 1 (P = .53). Figure 1 shows all referrals sent to each speciality during years 1 and 2. Consort diagram showing all referrals to different specialist units during year 1 and 2. Year 1: From March 16th, 2019 to March 15th, 2020. Year 2: From March 16th, 2020 to March 15th, 2021.
Among all referral types, urogenital carcinoma was the most frequently diagnosed cancer during both the pandemic (65 patients, 32.8%) and pre-pandemic year (28.4%) (P = .42). During the COVID-19 year, 6 patients were diagnosed at advanced stage (all prostate cancer), vs 7 patients (4 prostate, 2 bladder and 1 renal cancer) during year 1 (P = .6).
Breast cancer (BC) was confirmed in 45 patients (22.7%) during year 2, a similar ratio to the year before (25.5%) (P = .6). In total, 27 patients (60%) had localized BC, 15 (33.3%) had locally advanced disease and 3 advanced disease, showing similar figures to the pre-pandemic year. During the COVID-19 pandemic outbreak year, 25 patients (55.5%) diagnosed in our department fell outside the mammography screening target age group (45-69 years), the same proportion of patients as the preceding year.
Gastrointestinal tumours were found in 31 patients (15.6%) during year 2, with 21 (67.7%) cases of colorectal carcinoma (CRC): 11 (52.3%) were localized and 4 (19%) advanced carcinoma. During year 1, 39 patients (22.1%) were diagnosed with gastrointestinal tumours (27 colorectal), a nonsignificant higher rate than in the COVID-19 year (P = .18). During year 2, 17 patients (80%) were diagnosed outside the CRC screening programme age range (50-69 years), whereas 60% of all patients were diagnosed outside the screening programme during year 1. Figures S1 and S2 show differences between year 1 and 2 regarding diagnosis in ages included in early cancer detection programs (breast and colorectal cancer). There are no significant differences between the 2 years in age of diagnosis of breast carcinoma and colorectal cancer, despite the cessation of activity of the Screening Units (P = .97 and P = .65, respectively) [March 16th to June 1st 2020] (Supplementary material annex 1 and 2).
Lung cancer was diagnosed in 12 (9%) and 17 (8.5%) patients in year 2 and 1, respectively. During year 2, 6 patients (35.2%) were diagnosed at a localized stage, whereas 5 (29.4%) had a locally advanced disease and 6 (35.2%) had advanced disease, compared with the 9 patients (75%) diagnosed at an advanced stage in year 1 (P = .39).
Head and neck malignancy was confirmed in 9 cases (4.5%), of which 6 (66.6%) were diagnosed with locally advanced squamous cell carcinoma during the COVID-19 year, compared to 3 patients (1.7) diagnosed during year 1 (P = .21).
Gynaecologic cancer was confirmed in 14 (7%) patients in year 2 and 7 (3.9%) in year 1, of which 85% and 50% were cervical in situ carcinoma, respectively. Haematological malignancies were diagnosed in 10 and 7 patients during year 2 and 1 respectively.
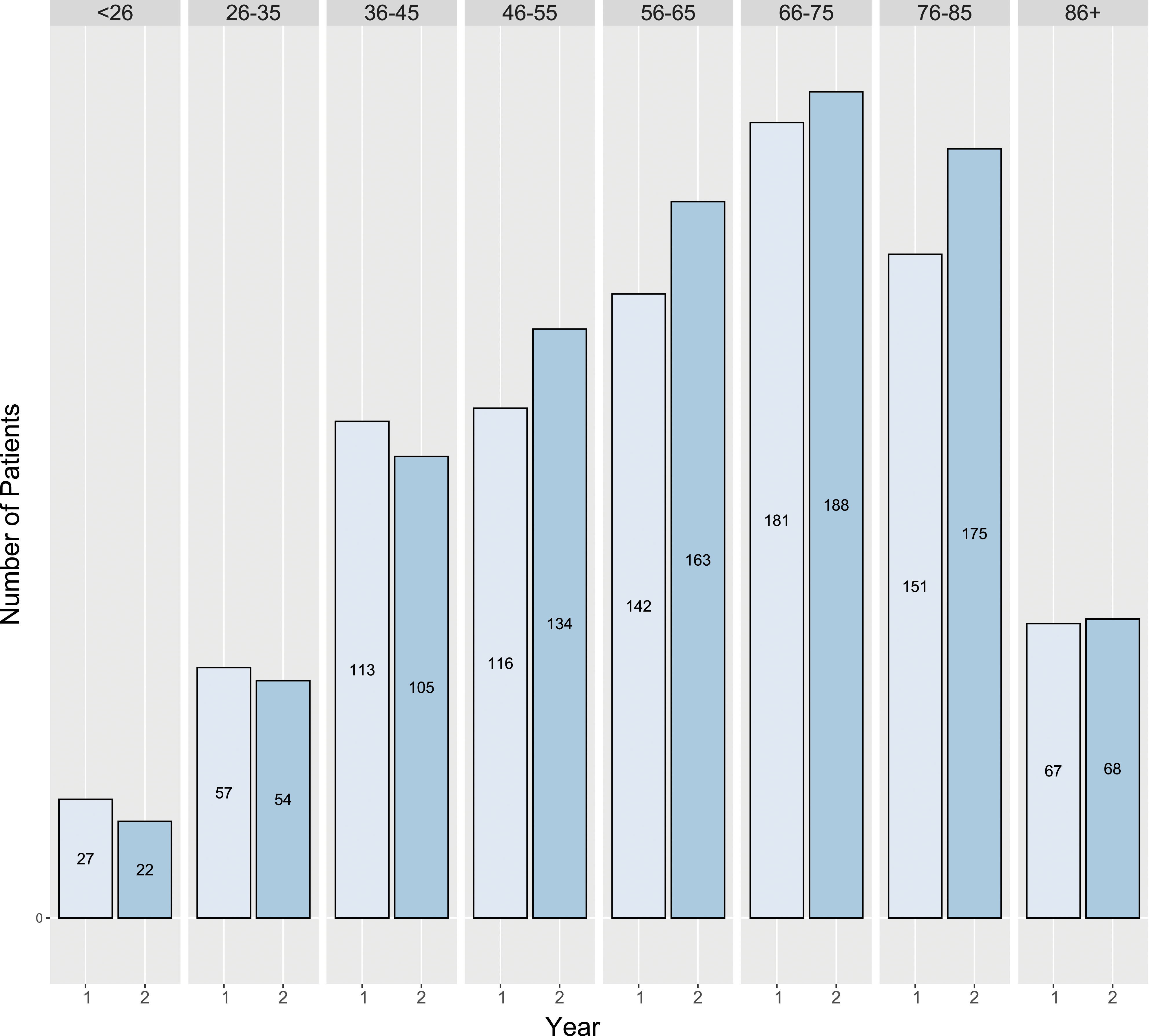
Figure 2 shows all cancer diagnoses during the pandemic and pre-pandemic year. Figure 3 shows the number of suspected cancer patient referrals by month and the difference between the 2 years under study, and Figure 4 shows referrals by age group. Diagnoses by speciality among all studied patients during years 1 and 2. Year 1: From March 16th, 2019 to March 15th, 2020. Year 2: From March 16th, 2020 to March 15th, 2021. The others group includes haematology, dermatology, traumatology and other diagnoses from the above pathologies. CIS: carcinoma in situ; H&N SCC: head and neck squamous cell carcinoma. Referrals by month between year 1 and 2; COVID-19 admissions in our institution between every month during year 2. *: Indicates significant differences between years 1 and 2. Year 1: From March 16th, 2019 to March 15th, 2020. Year 2: From March 16th, 2020 to March 15th, 2021. Referrals by age range across year 1 and 2. There are no statistically significant changes between groups of age. Year 1: From March 16th, 2019 to March 15th, 2020. Year 2: From March 16th, 2020 to March 15th, 2021.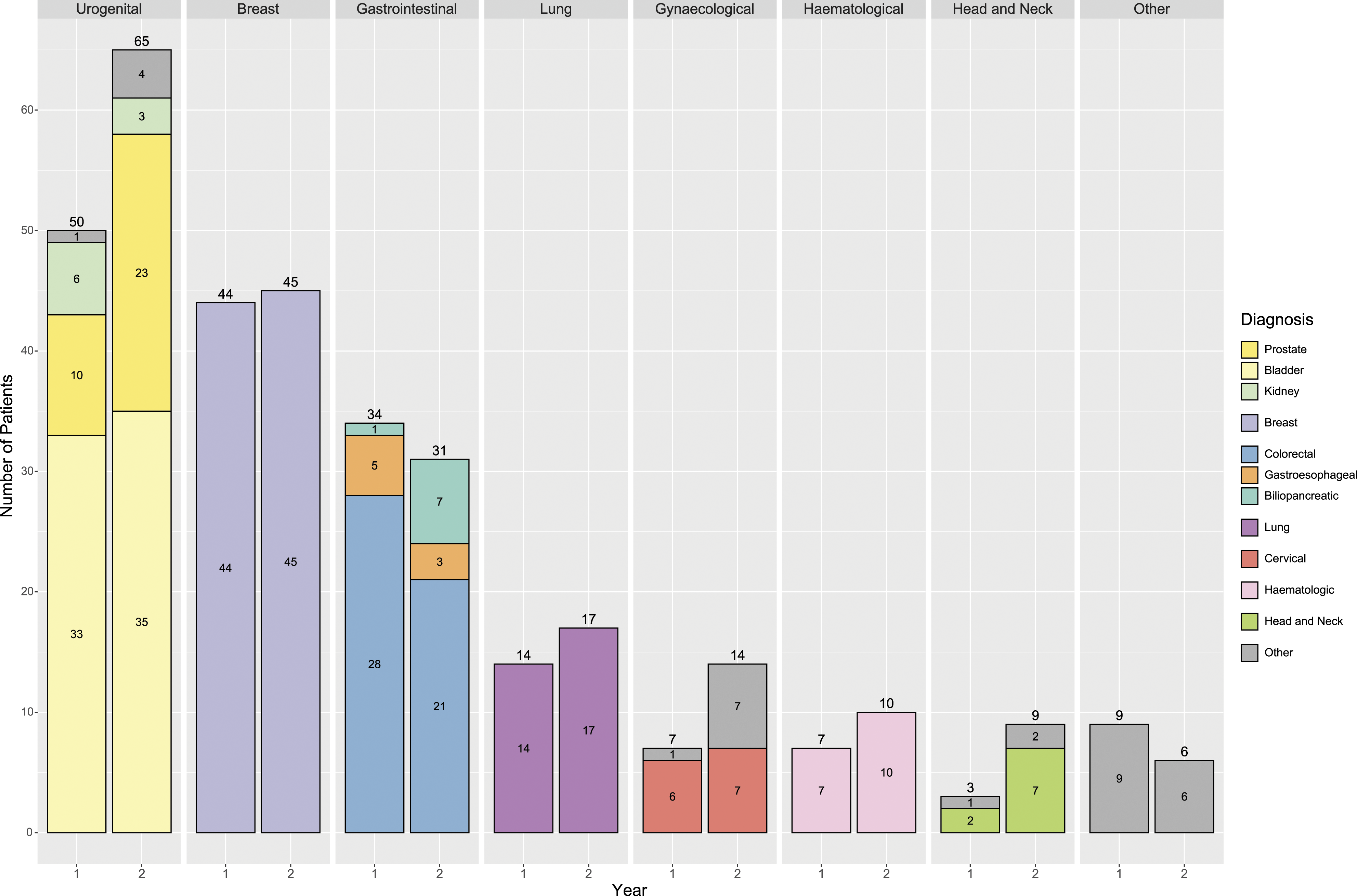

During the COVID-19 year, the median time from submission of referrals to specialist testing was 13 days (8-22 days; quartiles 1 and 3 [q1q3]), a similar interval to the previous year (12 days, 7-24 days, q1q3) (P = .21). Turnaround time from referral to diagnosis was a median of 18 days (10-30 days; q1q3) and 15 days (8-33 days; q1q3) during years 2 and 1 respectively (P = .09). Patients ultimately receiving a cancer diagnosis during year 2 received specialist assessment at a median of 10 days (6-18 days; q1q3), and histopathological diagnosis was made at a median of 17 days (10-28 days; q1q3) from referral. Treatment (surgery or chemotherapy) was started at a median of 30 days (13-51 days; q1q3) from diagnosis. During year 1, patients were assessed by the specialist at a median of 10 days (6-16 days; q1q3) and histopathological diagnosis was achieved at a median of 14 days (9-30 days; q1q3) from submission. Treatment (surgery or systemic treatment) was started at a median of 35 days (16-57 days; q1q3) from diagnosis. Therefore, there are no significant differences between both years (P = .94, P = .39, P = .10 respectively).
In patients in whom cancer diagnosis was ultimately ruled out, the median time from referral to first appointment was similar in years 2 and 1: 14 days (8-25 days; q1q3) and 12 days (7-24 days; q1q3), respectively (P = .2); and rule-out diagnosis was reached at a median of 18 days (11-30.5 days; q1q3) and 15 days (8-33 days; q1q3) from referral during year 2 and 1 respectively (P = .21).
Median Waiting Times From Patient Referral to First Specialist Visit, Diagnosis and Treatment Initiation (Patients Diagnosed With Oncological Disease Only), in Year 1 (From March 16th, 2019 to March 15th, 2020) and Year 2 (from March 16th, 2020 to March 15th, 2021).

The other specialities group includes haematology, dermatology and traumatology.
Discussion
In the Spanish health care system (GPs and specialists), cancer patient access to oncology departments is via different pathways such as screening programmes, emergency presentation and GP referrals. Spanish cancer detection programs are available for the whole Spanish population and include colorectal cancer detection by faecal occult blood test from age 50 and breast cancer detection with mammography from 45 to 50 years old onwards. Patients with suspected cancer symptoms are usually referred by their GPs for specialist consultation, a process taking several weeks before the CFP was created. In CMH in Valencia, a CFP was set up in 2009 aimed at reducing waiting times between patient GP consultation with suspected cancer and assessment by the corresponding specialist, as well as improving GP–specialist communication. During 10 years under the CFP, 4493 patients with suspected cancer were referred from primary care and most were evaluated by the hospital specialist within 15 days. 6 As well as shortening time to cancer diagnosis, the CFP also reduces anxiety in patients with suspected disease and improves quality of care by enhancing primary–specialized care coordination. The objective of this retrospective study was to investigate the impact of the COVID-19 pandemic on cancer diagnostics in general and specialized practices in a region of Valencia (Spain), as well as to determine whether cancer diagnosis was made in early or advanced stages.
The three initial official waves in Spain since the declared state of emergency are the second nights of March-June 2020, October-December 2020 and January-March 2021. Subsequently, there were three more waves of infections, but with less consequences on the functioning of healthcare system. The COVID-19 pandemic is estimated to have caused more than 100 000 deaths in Spain so far, over 51 000 confirmed by Polymerase chain reaction (PCR). The Spanish Government decreed a nationwide state of emergency on March 14th 2020; a population lockdown started after that, restricting free movement to essential activities such as purchase of food and medicine products or travel to and from medical centres or the workplace. On March 28th 2020, all non-essential face-to-face work activity was suspended for 15 days (www.lamoncloa.gob.es). The risk of disease spread within crowded hospitals led the American Society of Clinical Oncology (ASCO) to recommend deferring all clinical appointments that could be postponed without risk to the patient.8,9 To reduce the risk of the health system overload observed in other countries,10,11 the Spanish government and the different autonomous communities took drastic measures from March 2020. These included postponing non-urgent clinical appointments, substituting face-to-face visits for phone appointments in both primary care centres and hospitals, cancelling non-urgent surgeries, increasing intensive care unit capacity and restricting social contact with a national lockdown. 12 The COVID-19 pandemic also affected therapeutic compliance, as fear of COVID-19 infection delayed diagnostic and therapeutic procedures; screening programmes for breast, colorectal and cervical cancers were also suspended. 13 Numerous authors found a reduction in cancer diagnoses of up to 45% in 2020 owing to the above factors. 14 Although effective in reducing the number of new COVID-19 infections, 15 these measures may also have had a detrimental knock-on effect on diagnosis of other medical pathologies such as cardiac, 16 neurological, 17 and oncological disease.18-24 Multiple studies have shown that cancer incidence decreased during the state of emergency in several countries, especially in cancers reliant on screening, due to closure of screening units.9,14,25-33 Early diagnosis is crucial to achieve curative treatment in cancer, so delays in cancer diagnosis due to the COVID-19 pandemic could trigger a rise in disease-related mortality. 34
We also compared referral and diagnosis numbers by month during the past year, as the incidence of COVID-19 varied across the different pandemic waves. Our hospital has 582 beds available, and the months showing the highest number of hospital admissions due to COVID-19 disease were March 2020 (n = 193 admitted), October–December 2020 (average of 300 monthly admissions) and January 2021, with 804 patients requiring hospital admission. No effects on CFP performance or quality were observed, as reflected in the accompanying figures and Table 1. As shown in Figure 3, far fewer referrals were made during April and May 2020 than in the year before, coinciding with the first wave and lockdown (72 vs 32 referrals in April 2019 and 2020, respectively; 97 vs 67 in May 2019 and 2020, respectively). Interestingly, during June, July and August 2020 the number of cancer referrals and diagnoses increased considerably compared to 2019 (54, 53 and 16 diagnosed cases for year 1; 70, 69 and 47 for year 2), possibly offsetting the paucity of referrals during the previous months. The number of patients allocated to the CFP fell again at the beginning of the second wave (91 vs 44 in years 1 and 2, respectively), but recovered during November, December and January, even increasing during the third wave (February 2021), the largest and most complicated wave in our department. Nevertheless, the percentage of positive cases during this time period remained almost identical (21.7% vs 22.9% for year 1 and 2, respectively). During the year under study, non-urgent surgeries and scheduled appointments were suspended in our health department, but patients referred via the CFP continued to be assessed, diagnosed and if necessary treated for oncological disease. A key finding was that lung neoplasms were detected in earlier stages, inviting hypotheses as to the role of the COVID-19 pandemic in diagnosis of this cancer. One possible explanation is that patients in this collective attributed respiratory symptoms including persistent cough to COVID-19, and consulted their GP more promptly than populations in previous years. Notwithstanding with these findings, differences were not statistically significant. For GPs, the COVID-19 pandemic has brought changes in medical practice, ushering in the first steps towards digital care such as increased use of telephone consultations and fewer face-to-face appointments. The findings of the study and in particular the proportion of cancer diagnoses (24%) demonstrate that clinical intuition has not been lost. Patients with well-known warning symptoms such as breast lump or rectal bleeding are also likely to continue to seek primary care. With COVID-19 at the forefront, however, patients might overlook vague cancer symptoms such as fatigue or weight loss, while conversely, respiratory symptoms possibly attributed to COVID-19 could prompt them towards earlier consultation.
This study shows that although PC has often been obscured by the COVID-19 pandemic, symptoms suggestive of cancer are still present and alert doctors to use the CFP. Likewise, we have shown that despite the serious situation in hospitals, care for suspected cancer patients is still a priority and cancer diagnosis and treatment have not been delayed across the past year. The CFP was maintained during the COVID-19 pandemic thanks to the extensive efforts of PC and hospital specialists. Our program has certain limitations which must be considered, such as the fact that our referral guidelines are not standardized but rather based on clinical practice and medical literature. Nonetheless, the CFP has remained a useful diagnostic tool for patients with suspected cancer in the face of the adverse health situation caused by SARS-CoV-2 coronavirus. The indirect conclusions of our findings are that telephone contact has been correctly used in PC, since emergencies were attended in person, and telephone consultations deemed urgent were also dealt with face-to-face. Longitudinally in PC and GP knowledge of patients has enabled an efficient use of telephone contact to arrange second face-to-face appointments to confirm suspicions and thus make timely referrals to the CFP. The CFP has continued to function as a form of rapid contact between different care levels for patients with suspected cancer, and both diagnostic and therapeutic in-hospital care has been maintained, with similar waiting times despite the COVID-19 pandemic. This study also has several important implications and strengths: firstly, we found that patients benefitted from the close relationship between PC and hospital specialists maintained by the CFP, notwithstanding the COVID-19-related health crisis; and secondly, ours is one of the few studies which showed a reduction in diagnostic waiting times for patients with suspected cancer during the COVID-19 pandemic.
Conclusion
The COVID-19 pandemic has forced doctors to make changes to patient care protocols, and many delayed diagnoses of serious diseases have occurred during this period.
Our program has proven a reliable tool for GPs referring patients with suspected cancer, helping to maintain a normal, efficient workflow despite the current pandemic.
Supplemental Material
Supplemental Material - Impact of the COVID-19 Pandemic on a Cancer Fast-Track Programme
Supplemental Material for Impact of the COVID-19 Pandemic on a Cancer Fast-Track Programme by M. T. Martínez, S. Moragon, B. Ortega-Morillo, J. Montón-Bueno, S. Simon, S. Roselló, A. Insa1, A. Viala, J. Navarro, A. Sanmartín, C. Fluixá, A. Julve, D. Soriano, E. Buch, A. Peña, J. Franco, J. Martínez-Jabaloyas, J. Marco, M. J. Forner, A. Cano, A. Silvestre, A Teruel, B. Bermejo, A. Cervantes, and I. Chirivella Gonzalez in Cancer Control
Footnotes
Acknowledgments
We would like to thank all patients and GPs.
Author Contributions
AC, IC, JN, and AS conceived the study and created CF. IC and MM supervised the study, coordinate, and design all aspects of the work. BO, SS, JM, and SM contributed data collection and computational analysis. IC, MM, AJ, EB, AP, JF, JM, MF, AT, AS, AV, AC, AI, BB, DS, and SR contributed clinical patient data. MM, IC, and AC wrote the manuscript. All authors reviewed, read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by the clinical research and ethics committee of University of Valencia, Spain (approval number 2020/312) with waiver of the informed consent.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.