
Abstract
Objectives
The objective of this study was to assess the impact of the COVID-19 pandemic, after 2 years, on mammographic screening in Brazil evaluating BIRADS® results, breast cancer diagnosis rates, and breast cancer stage.
Study Design
This was an ecological observational study based on retrospective data from Brazil’s mammographic screening program from 2015 to 2023.
Methods
Data were obtained from the national screening database DATASUS – SISCAN (Cancer System Information) and retrieved in March 2024. Inclusion criteria comprised completeness of mammogram data (incomplete records were excluded), female participants aged 50 to 69 years, and mammograms exclusively performed for screening purposes. The study analyzed the number of mammograms conducted during the specified period, focusing on BIRADS® test results.
Results
Out of 23,851,371 mammograms performed between 2015 and 2023, 15,000,628 were included for analysis. A significant reduction of 39.6% in mammograms was observed in 2020 compared to 2019, followed by a 12.6% decrease in 2021. Notably, a substantial rise in BIRADS categories 4 and 5 examinations was seen post-pandemic. Breast cancer staging analysis revealed a shift towards more advanced stages (III and IV) diagnosed post-pandemic, suggesting potential delays in detection and diagnosis.
Conclusions
In conclusion, the study highlighted significant discrepancies in mammographic screenings and breast cancer diagnosis rates over 9 years. The pandemic reflected significant influence on the timing and stage at diagnosis, suggesting potential delays in detection and diagnosis that resulted in later identification of more advanced disease stages.
Keywords
Introduction
On March 11, 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) a pandemic. 1 Globally, the management of COVID-19 necessitated the shutdown or suspension of many non-essential medical services, sparking concerns about the utilization of healthcare services.2,3 Studies have documented a significant decline in breast cancer screening, with some reporting reductions of up to 99% during the initial wave of the pandemic from March to June 2020.4-7 Subsequently, as COVID-19 transmission decreased, screening mammography gradually resumed.
However, the long-term repercussions of the temporary suspension of screening mammography remain unclear. While some studies have indicated a recovery in screening mammography volumes during the early phases of reopening post-shutdown in 20207-10 and in May to July 2021, others have observed a sustained overall decrease in screening mammography throughout 2020. 11
We have previously reported on the impact of the COVID-19 pandemic on breast cancer screening in Brazil. 12 Among the target population of women aged 50-69 years, mammography attendance decreased by 39.2% in public healthcare (SUS) facilities when comparing 2019 to 2020, and by 13.3% in 2021 compared to 2020. 12
A systematic review revealed significant reductions in breast screening volume and diagnosed breast cancers during the peak of the pandemic, with a comparatively smaller reduction following the peak. Changes in the proportions of detection mode and stage at diagnosis were noted, with higher proportions of cases diagnosed through symptomatic presentations and a greater proportion of relatively more advanced stages at diagnosis during the pandemic. 13
Since the onset of the COVID-19 pandemic, an increasing number of reports have highlighted its impact on cancer care. As of March 2024, PubMed lists 2113 articles with keywords “Covid” and ”breast cancer.” Most studies have found a negative association between lockdown restrictions and breast cancer care, including challenges in accessing healthcare, 14 increased prescription of preoperative endocrine therapy, 15 and even delayed surgery beyond 12 weeks.16,17
The Brazilian national guidelines for early breast cancer detection, established in 2004 by the Brazilian National Cancer Institute (INCA), were updated in 2015 and currently recommend that all women aged 50-69 years undergo mammography screening every 2 years. 18 Early detection plays a crucial role in reducing mortality and the intensity of required treatment. Delays in the diagnosis and treatment of breast cancer due to the pandemic are anticipated to necessitate more aggressive and mutilating treatment approaches, potentially leading to increased mortality. 3
The aim of this study is to assess the impact of the COVID-19 pandemic, 2 years after its onset, on mammographic screening in Brazil. We will evaluate a 9-year span from 2015 to 2023, analyzing BIRADS® results, breast cancer diagnosis rates, and breast cancer stage to gain insight into the pandemic’s impact on breast cancer screening and diagnosis in Brazil.
Methods
Study Design
This was an ecological observational study based on retrospective data from Brazil’s mammographic screening program from 2015 to 2023, conform to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 19
Data Sources
This ecologic observational study utilized retrospective data from the Brazilian Ministry of Health’s mammography screening program. The National Breast Cancer Screening Bank (DATASUS/SISMAMA/Information System on Breast Cancer) served as the primary data source. SISMAMA is a public department aimed at providing the Brazilian health system with essential information for planning, operating, and controlling health actions. It records requests for breast cyto/histopathological exams, mammography, results of all requested exams, and monitoring of altered exams, thus facilitating monitoring and evaluation. The data are publicly available for download and analysis. Notably, in Brazil, mammography performance is entirely opportunistic, with women in the recommended age range (50-69 years) encouraged to seek public service and undergo physical examination and mammography every 2 years. Therefore, campaigns are essential for reaching the target population. Data were downloaded in March 2024, with 2023 being the last complete year reported in the database.
Inclusion and Exclusion Criteria
Key inclusion criteria included the availability of complete reports on the number of mammograms for the study period (missing data were excluded), age filtering (50 to 69 years old), and selection of only mammograms performed for screening purposes. The study evaluated the number of mammograms performed in the specified period, considering BIRADS® test results.
Statistical Analysis
Data were analyzed as follows: (a) absolute number of mammograms performed per year (2015-2023); (b) comparison of mammograms for pre-pandemic (2019), pandemic (2020 and 2021), and post-pandemic (2022 and 2023) periods; (c) mammograms per year according to risk factors (family history and previous breast cancer diagnosis); (d) breast cancer stage; (e) screening rate.
A chi-square test for independence was employed for each BIRADS category and staging to compare observed case numbers against expected distributions from aggregated data. Expected frequencies were calculated by averaging each stage’s proportions across all years, assuming negligible annual variations under the null hypothesis. P-values were calculated to determine the statistical significance of discrepancies between observed and expected frequencies, with a conventional alpha level set at .05 for significance. Particularly in the post-pandemic period, P-values were significantly lower than .0001, indicating marked changes in staging patterns. To project the number of mammograms from 2020 to 2023, based on historical data from 2015 to 2019, a linear projection method was utilized. Using the linear regression equation derived from pre-pandemic data, predictions for the expected number of mammograms in 2020 to 2023 were made, assuming that the trend established between 2015 and 2019 would continue in the absence of the pandemic.
Ethics
This study used publicly available, anonymized data from the Brazilian Ministry of Health’s National Breast Cancer Screening Database (DATASUS/SISMAMA). According to the Brazilian Resolution CNS 510/2016, Article 1, Section VII, ethical approval is not required for research that utilizes publicly accessible data, as long as the information remains anonymized. Furthermore, this is in line with international guidelines, such as the Declaration of Helsinki and the US Common Rule (45 CFR 46.104(d)(4)), which exempt the need for ethical review for studies utilizing publicly accessible anonymized data. Based on these principles, no ethical approval was required for the current study.
Results
Between 2015 and 2023, 23,851,371 mammograms were performed across all age groups, with 542,889 (2.3%) classified as diagnostic and 23,308,482 (97.7%) as screening examinations. Out of the screening mammograms, 8,307,854 (34.8%) were conducted outside the Ministry of Health’s recommended age range of 50-69 years. Per the study’s criteria, 15,000,628 (62.9%) mammograms were included for analysis (Supplement Fig 1).
Mammographic Screening Performed in Brazilian Women, Aged 50 to 69 Years.

Legend: Difference in the pandemic period was compared to 2019, and pos-pandemic was compared to 2019. Source: DATASUS – SISCAN, accessed on 01/04/2024.
Figure 1 shows the graph of examinations performed from 2015 to 2023, as well as the projection of examinations for 2020 and 2023 if there was an increase in the number of mammograms performed following the proportions of the years before the pandemic. Comparison of examinations carried out in the period 2015-2023 and the projection of examinations if the pandemic did not occur. Source. DATASUS – SISCAN accessed on 01/04/2024.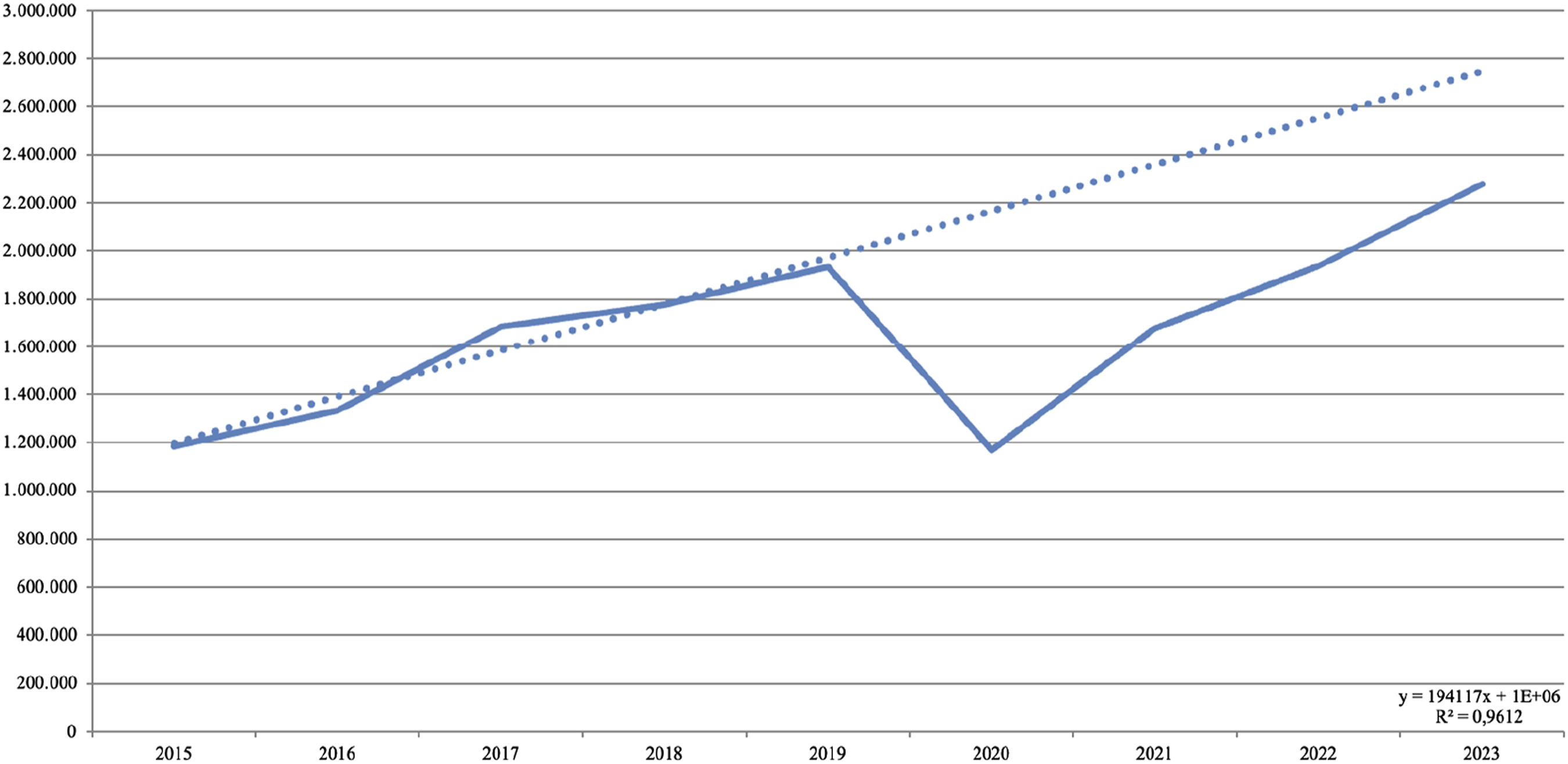
Comparative Results of Mammograms Over Pre-Pandemic, Pandemic and Pos-Pandemic Biannual Years.

Source. DATASUS –SISCAN accessed on 01/04/2024.
Distribution of Clinical Staging in the Pre-Pandemic, Pandemic and Post-Pandemic Periods.

Source. DATASUS –SISCAN accessed on 01/04/2024.
Comparative Analysis of the Change in Staging Between the Pre-Pandemic Period With Pandemic and the Pandemic Period With Post-Pandemic.

Source. DATASUS –SISCAN accessed on 01/04/2024.
Discussion
In this ecologic observational cross-sectional study, we compared breast cancer (BC) screening across 3 distinct periods: pre-pandemic, pandemic, and post-pandemic. Our analysis revealed a notable decline in the proportion of women up-to-date with screening during the pandemic, with a subsequent increase post-pandemic that did not fully recover to pre-pandemic levels. Notably, there was an increase in suspicious mammograms (BIRADS categories 4 and 5) and advanced clinical stage BC diagnoses post-pandemic.
The pandemic era saw a significant reduction of 39.6% in breast screening mammograms performed in 2020, followed by a 13.3% reduction in 2021. While there was a modest increase of .2% in 2022 and a notable 17.9% increase in 2023, these findings fell short of the estimated number of 2,750,000 exams by 2023.
Similar trends in reduced healthcare demand during the pandemic have been reported by other authors, including declines in emergency services utilization.20,21 Naidich et al reported that the greatest decline in imaging volume during the pandemic was observed among outpatient imaging examinations (88%), affecting all modalities, but the decline was highly pronounced in mammogram examinations (94% less than that in 2019). 21
The reductions in breast screening volume and number of diagnosed breast cancers found in our study were also noted in other systematic reviews of the impact of COVID-19 pandemic related to cancer healthcare. One review identified significant declines in cancer screening or tests and cancer diagnosis rate, and found an increase in advanced cancers, but this study only included 17 publications. 22 One meta-analysis with relatively smaller number of papers (13 publications) reported incidence rate ratios of .10-.63 for cancer screening institutions. 13 Another review also identified a remarkable frequency (up to 79%) of delays and disruptions in all cancer care attributed to the pandemic. 3
In keeping with the reduction in screening volume, there was a decrease in the proportion of screen-detected cancers and a relative increase in cases diagnosed clinically through symptomatic presentations. This aligns with a systematic review 11 that have demonstrated over proportions of early-stage and higher proportions of relatively more advanced cases were reported in the pandemic compared to the pre-pandemic period. Concomitantly, greater proportions of cancers with nodal and distant metastases were found. Even though the stage distributions might raise concerns about potentially worse long-term outcomes, these results should be interpreted with the caveat that these are the percentage of cases from the diagnosed breast cancers, and do not reflect population rates. Moreover, the association between diagnosis delay and long-term findings has not been well-established by recent metanalyses. 11
We must consider delays in breast examinations in terms of not only how to return to the normal number of examinations but also how to mitigate the effects of delayed diagnoses.
This study has limitations related to observational studies such as risk for imprecisions in the registries and the inferences surrounding our findings. For example, we were not able to assess in the database the number of women who should be screened (potential candidates).
This suggests the pandemic’s potential influence on cancer detection and diagnosis, leading to the identification of more advanced stages thereafter.
Despite its contributions, our study has limitations inherent to observational designs, including potential inaccuracies in registries and inference limitations. Additionally, missing data due to loss to follow-up may bias results, particularly if related to the outcome. Furthermore, the inability to assess the number of potential screening candidates in the database is a notable limitation.
Conclusion
In summary, our analysis of Brazil’s national screening database revealed significant discrepancies in mammographic screenings and breast cancer diagnosis rates across 9 years. Notably, during the pandemic, there was a substantial decline in mammogram screenings, followed by a resurgence afterwards. Post-pandemic data indicated an increase in the detection of BIRADS categories 4 and 5, which significantly diverged from expected patterns. Additionally, breast cancer staging analysis showed a predominance of early stage diagnoses pre-pandemic, with a shift towards more advanced stages (III and IV) diagnosed afterwards. This shift reflects the pandemic’s significant influence on the timing and stage at diagnosis, suggesting potential delays in detection and diagnosis that resulted in later identification of more advanced disease stages.
Supplemental Material
Supplemental Material - Two Years Post-COVID-19: An Ecologic Study Evaluating the Impact on Brazil’s Mammographic Screening Program
Supplemental Material for Two Years Post-COVID-19: An Ecologic Study Evaluating the Impact on Brazil’s Mammographic Screening Program by Marcelo Antonini, André Mattar, Denise Joffily Pereira da Costa Pinheiro, Marina Diógenes Teixeira, Andressa Gonçalves Amorim, Odair Ferraro, Francisco Pimentel Cavalcante, Felipe Zerwes, Marcelo Madeira, Eduardo de Camargo Millen, Antônio Luiz Frasson, Reginaldo Guedes Coelho Lopes, Fabrício Palermo Brenelli, Renata Montarroyos Leite, Luiz Henrique Gebrim, and Ruffo Freitas-Junior in Journal of Cancer Control.
Footnotes
Acknowledgments
We would like to thank all patients who participated in the study.
Author Contributions
Marcelo Antonini: Conceptualization, Methodology, writing – original draft. Andre Mattar: Conceptualization, writing – review & editing. Denise Joffily Pereira da Costa Pinheiro: Writing – review & editing. Marina Diógenes Teixeira, Writing – review & editing. Andressa Gonçalves Amorim: Writing – review & editing. Odair Ferraro: Supervision, Writing – review & editing. Francisco Pimentel Cavalcante: Writing – review & editing. Felipe Zerwes: Writing – review & editing. Marcelo Madeira: Writing – review & editing. Eduardo de Camargo Millen: Writing – review & editing. Antonio Luiz Frasson: Writing – review & editing. Reginaldo Guedes Coelho Lopes: Supervision, writing – review & editing. Fabrício Palermo Brenelli: writing – review & editing. Renata Montarroyos Leite: writing – review & editing. Luiz Henrique Gebrim, Luiz Henrique Gebrim: Supervision: Writing – review & editing. Ruffo Freitas-Junior: Writing – review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.