
Abstract
Objective
To evaluate the potential impact of tobacco reduction on future cancer incidence in Colombia
Introduction
Colombia has implemented multiple actions that led to reducing smoking prevalence in recent years. However, the numbers of cancer cases and deaths associated with smoking exposure remain high highlighting the importance of maintaining efforts to reduce and keep smoking prevalence low.
Methods
We performed a theoretical modeling exercise, projecting expected changes in the incidence of four cancers between 2016 and 2050 under two simulated scenarios of smoking reduction.
Results
A cumulative decline of 10% in the prevalence of smoking, a percentage in line with current cigarette taxation policies, will decrease cancer incidence in 2050 by 3.2%, .5%, .2% and .2% of lung, liver, cervical and colorectal cancer incidence, respectively. Complete elimination of tobacco consumption will reduce these by 39.1%, 6.1%, 2.2% and 2.3% respectively, by 2050.
Conclusion
These results highlight the importance of continuity and reinforcement of current tobacco control programs, including increasing taxation, to further reduce the prevalence of tobacco smoking and reduce cancer cases and deaths in the coming decades.
Introduction
Worldwide, tobacco use is the major preventable cause of cancer incidence and death. Cancer in Colombia was the second leading cause of death from chronic disease after cardiovascular disease in 2018, with approximately 45,466 [30,496 – 65,692] annual deaths. 1 Smoking is a risk factor for more than 20 different types of cancer; thus tobacco control has been an important global health focus in the last decades. 2
In Colombia, lung, liver, cervical, and colorectal cancers are the four most frequently occurring cancer types associated with tobacco use (relative risks RR>1.15). 3 According to GLOBOCAN 2020 estimates, these four cancers are placed in the top 10 cancers with the highest mortality. 4
The current prevalence of smoking in Colombia is 9.8%. Even though this is one of the lowest rates in the Latin American region, the associated morbidity is still significant.5,6 In recent decades, the Colombian government has implemented policies to prevent, discourage, and reduce smoking. 7 Colombia has implemented multiple actions to reduce the prevalence of smoking, including the adoption of the Framework Convention for Tobacco Control of the World Health Organization (WHO FCTC) and the implementation of a national Ten-Year Plan for Cancer Control 2012-20218,9 with reduction of smoking included as one of the main actions for cancer risk control. There have been various control mechanisms to reduce tobacco consumption, with tax reforms between 1997 and 2016 being the most effective. 7 The continuation of such interventions should significantly reduce cancer cases, including reinforcement of the existing and potentially new national public health programs to reduce tobacco consumption. 10
To evaluate the impact of reducing tobacco consumption on the incidence of tobacco associated cancers, this project carried out a theoretical modeling of the expected changes in the incidence of lung, liver, cervical, and colorectal cancers between 2016 and 2050 under two simulated scenarios of smoking reduction based on current tobacco control policies.
Methodology
Statistical Analysis
A population-based macro-simulation model was developed for Colombia, based on the PREVENT 3.01 model previously used in studies of estimating population attributable risks and attributable fractions.11-15 Briefly, this model uses data on age- and sex-specific incidence rates of included cancers, population projections, and relative risks (RR), or risk functions for the association between risk factors and disease, to estimate the burden of disease in the future, under scenarios of hypothetical changes in the prevalence of exposure to risk factors. Our analyses used the estimated incidence by age and sex of lung, liver, cervical and colorectal cancer in Colombia. We projected the potential impact on the incidence of each of the four cancers for the period 2016-2050 under two hypothetical scenarios modifying the prevalence of tobacco consumption. The following information was included as input for the model:
Age-Specific and Sex-Specific Incidence Rates (ASIR) and Population Projections
We used national age-specific (five-year age groups from 0 to 70 years and over) and sex-specific estimates of lung, liver, cervical and colorectal cancer incidence for Colombia 16 and mortality data at the departmental level, based on data from four high-quality population-based cancer registries (Cali, Bucaramanga metropolitan area, Manizales and Pasto) included in editions X and XI of Cancer Incidence in Five Continents. 17
As a denominator for calculating expected rates and number of expected cases, we used the population distribution from 2016, taken from the Colombian National Statistics Agency (Departamento Administrativo Nacional de Estadística (DANE)). For the population sizes up to 2050, we used the projections prepared by the Economic Commission for Latin America and the Caribbean (CEPAL), which are discriminated by age and gender for each year of the time range established in the model. 18 An important assumption in the modeling exercise was that changes in smoking prevalence were not assumed to impact the population forecasts.
Smoking prevalence
We obtained the most recent and complete information on smoking prevalence from the National Study of Consumption of Psychoactive Substances in Colombia 2013. 5 Current cigarette use (yes/no) during the last month was derived as previously described. 13
Association Measures
Summary of the relative risks (RRs) used in the macrosimulation models for the four cancer types.

Lat and Lag Times
LAT time for smoking and consumption (time of change in prevalence without noticeable change in RR) of 5 years an LAG time (time since end of LAT until full effect in terms of RR of exposure) of 10 years were used for all cancer types. LAG and LAT times were defined by the authors based on those previously estimated in similar model exercises15,23 and supported by case control studies 24
Modeled Scenarios
Two scenarios were included and compared to the reference scenario of no interventions on tobacco: the first one consisted of an ideal model in which the prevalence of tobacco consumption is eliminated, and a second scenario where the prevalence of tobacco consumption is gradually reduced for 10 consecutive years starting from year 2017 and reaching a 10% reduction in prevalence associated with the implementation of policies to increase consumption taxes in 2026.
Human Subject Research
This is a modeling study without involvement of patients or public. The study was reviewed and approved by the Colombian Instituto Nacional de Cancerología E.S.E. (INC) research ethical board (INTOFI079982015).
Results
Modeled smoking prevalence for the baseline scenario (2016) varied between 1.6% and 12.7% among men aged 10 years and older, and between .7% and 7.1% among women in the same age groups (Supplementary Table 1). The highest smoking prevalence in men was 18.3% in the 20-24 age group and in women was 8.0% in the 50-54 age group.
Reduction of Lung Cancer Cases in the Period 2016-2050 After Tobacco Interventions
Expected number of new cancer cases in year 2050 under three modeled scenarios: Baseline (no intervention), 10% reduction in tobacco consumption and complete elimination of tobacco exposure.

Figures 1A and 2 A show that with a cumulative 10% reduction in the prevalence of tobacco consumption, an initial decrease in the number of lung cancer cases in both sexes is accomplished by 2023. In males, the annual rate between 2023 and 2031 would decrease from 12.93 ASIR per 100,000 to 12.69 and 543 cases of lung cancer would be prevented. However, the effects of the intervention are more evident in the following five years (2032-2036) where the annual ASIR would be reduced by an average of 5% (from 11.58 without intervention to 11.00 with a reduction of 10% in tobacco consumption), avoiding 891 new cases of lung cancer in males. For the period 2037-2050, a maximum of preventable cases is achieved with an average of 214 avoided cases every year. The incidence rate would remain relatively stable for women during the first eight-year period (2016-2023). From 2024 until 2038, the average annual ASIR would decrease from 6.80 to 6.04. By 2050 a reduction in the annual rate to 5.36 is achieved, representing 1,758 new lung cancer cases prevented in women over the entire period. Model of the effect in lung cancer ASIR for men and women after variations in tobacco consumption. A. Model of the effect after cumulative 10% reduction in tobacco consumption. B. Model of the effect after elimination of tobacco consumption. Number of avoided cancers in Colombia during the period 2016-2050 after variations in smoking prevalence. A. 10% reduction in tobacco consumption. B. Complete elimination of tobacco consumption.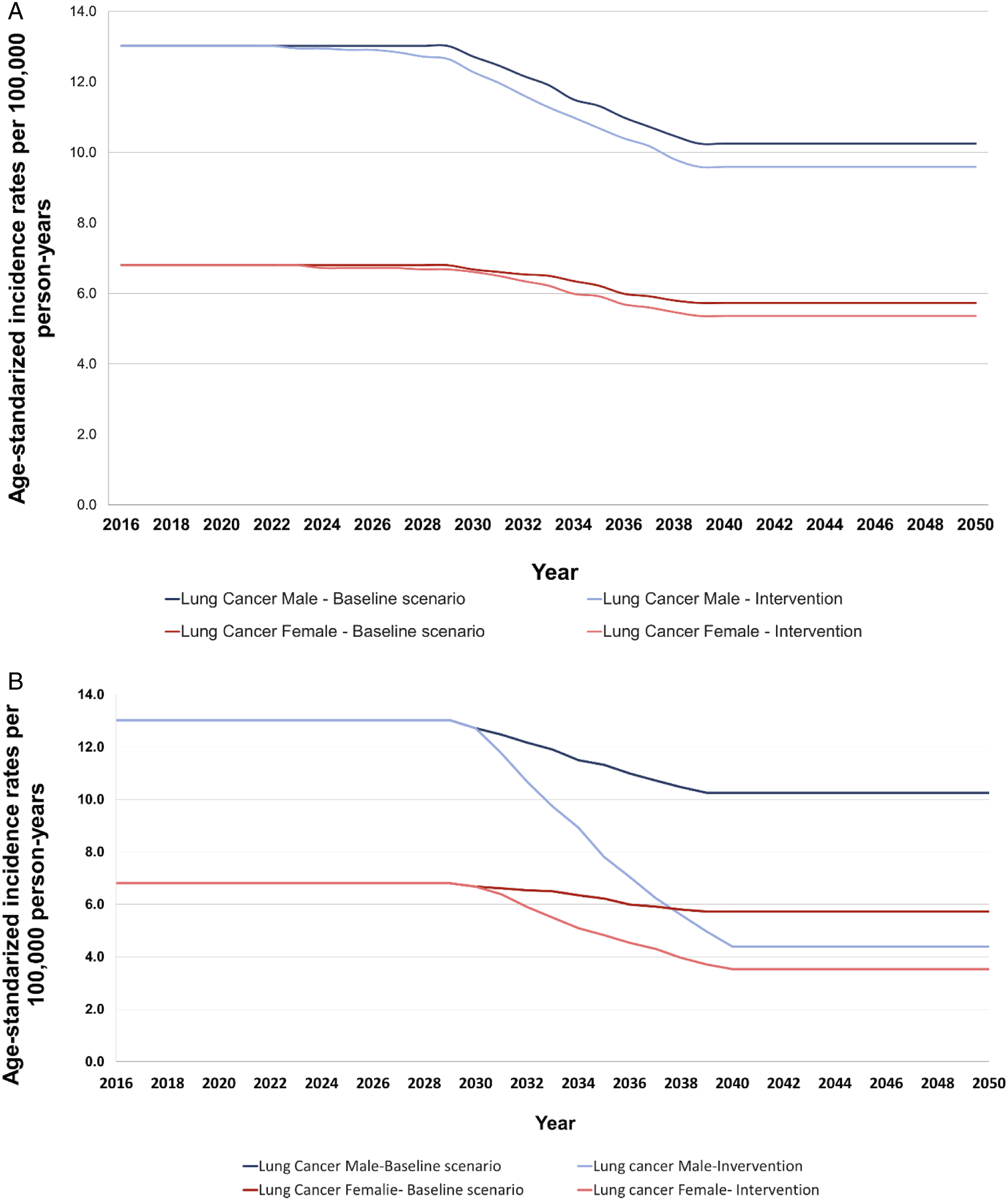

In contrast, the ideal scenario of complete elimination of tobacco consumption from 2016 onward will result in a drastic reduction of the ASIR in men from 11.31 cases per 100,000 to 8.09 (Figures 1 and 2B). Initially, this scenario will prevent 18,749 new cases for 2031-2039 period. The final ten years of the modeled period (2040-2050) will contribute to the annual average prevention of additional 2030 new cases. In women, the reduction in the annual rate of cases becomes evident as of 2031. Between 2031 and 2039, the annual ASIR is projected to drastically reduce from 6.18 to 4.91, preventing 7,850 new cases. An additional 836 new female lung cancer cases per year would be avoided between 2040 and 2050.
Impact of tobacco reduction on cancer cases of the liver, colorectum and cervix
For the period 2016-2050 in Colombia a cumulative 10% reduction in tobacco consumption would prevent a total of 295 cases of liver cancer, 488 cases of colorectal cancer in both sexes and 423 cases of cervical cancer in women, representing a reduction in incident cases .5%, .2% and .2%, respectively (Table 2, Figure 2A). Complete elimination of tobacco consumption would prevent 3,594 cases of liver cancer, 6,104 cases of colorectal cancer, and 5,069 cases of cervical cancer, which would be a reduction of 6.1%, 2.2% and 2.3%, respectively for the period 2016-2050.
Based on a 10% reduction in smoking prevalence the ASIR of liver cancer in both sexes would decrease early (starting in 2022 for women and in 2034 for men) (Supplementary Figure 1). A total decrease of .3% (2.42 vs. 2.39) in the incidence rate for men would be achieved by 2050. In addition, if complete elimination of tobacco consumption were to be achieved the decrease in ASIR of liver cancer in males would start ten years earlier (from 2024).
A 10% reduction in smoking prevalence will not produce significant differences in incidence rates for colorectal cancer cases. During the 2016-2050 period this change would represent an average annual decrease in ASIR of .1% in men and .07% in women (Supplementary Figure 2). However, elimination of smoking consumption would result in reductions in ASIR of 3% for men and in 1.1% for women, with an annual average of 136 preventable cases in men and 74 preventable cases in women in the period 2022-2050.
In cervical cancer the intervention of a 10% reduction in tobacco consumption shows a reduction in the incidence rate starting in the year 2034 with an average annual reduction of the rate of 1.2% and 76 preventable cases per year (Supplementary Figure 3). Complete elimination of tobacco prevalence would lead to a decrease in ASIR as early as 2024, an average annual reduction of 5.9% and an annual average of 187 preventable cases.
Discussion
Our results indicate that the two interventions considered (complete elimination of tobacco consumption and a 10% cumulative reduction in the percentage associated with the implementation of policies to increase consumption taxes) may lead to a reduction in the number of new cases for four cancer types analyzed in the period 2016-2050. The proposed interventions have the greatest impact on reducing lung cancer cases due to the strong documented association between tobacco use and the risk of developing lung cancer (Table 1). 21 The models estimated that in 2016-2050, 39.1% of the expected lung cancer cases in Colombia would be prevented if tobacco consumption is completely eliminated by 2017 and that 3.2% would be prevented if smoking consumption is reduced by 10% between 2017 and 2026. Although there are several other factors that influence the risk of developing lung cancer, including socioeconomic status, family history, occupational exposures (asbestos and silica dust), as well as environmental exposures to kitchen fumes, radon and particulate matter in the air25,26 worldwide, smoking is the attributed cause of 78% and 53% of lung cancer cases in men and women, respectively.26,27 Considering that lung cancer is the second leading cause of cancer mortality in Colombia for both sexes, 4 we confirmed that reducing tobacco prevalence remains an efficient public health intervention to reduce new lung cancer cases and future increases in mortality rates.
Our results also show an overall reduction of cancer incidence in liver, colon and rectum, and cervical cancers in women, although with more modest effects. In the period 2016-2050, 3,594 (6.2%) cases of liver cancer would be prevented if tobacco exposure would no longer exist, confirming that tobacco cessation will prevent liver cancer cases along with elimination of the additional major risk factors such as hepatitis B and C infections, excessive alcohol consumption, obesity, and the presence of diseases such as non-alcoholic steatohepatitis and non-alcoholic fatty liver disease. 28 The positive effect of smoking reduction in liver cancer incidence starts earlier in women than men in both simulated scenarios. This difference is explained by a higher relative risk of tobacco consumption in liver cancer for women, the projected demographic growth in Colombia by sex, and the sex variance in the projected increase in liver cancer incidence by 2050.
For colorectal cancer, we show that tobacco elimination will result in a net reduction of 6,104 (2.2%) of the expected cases by 2050.Colorectal cancer is currently the second most frequently diagnosed cancer in both sexes in Colombia 4 and interventions aim to reduce recognized modifiable risk factors such as obesity and alcohol consumption are fundamental to decrease incidence. A recent study showed that in addition to decreasing tobacco prevalence and exposure to alcohol, interventions aimed to reduce high body mass index (BMI) and increase physical activity may avoid a more substantial number of colorectal cancer cases in Colombia. 13 Modeled results on cervical cancer demonstrate that elimination tobacco consumption will prevent 5,069 (2.3%) new cases. Infection with Human Papilloma Virus (HPV) is the main risk factor for cervical cancer and HPV vaccination remains the primary public health intervention to prevent cervical cancer. 29 Still, evidence has shown that women who quit smoking have a two-fold reduced risk of developing cervical cancer, even after adjusting for HPV. 30 This confirms the additional benefit of smoking cessation preventing cervical cancer.
In Colombia, tobacco consumption prevalence has decreased from 12.9% in 2013 to 9.8% in 2019.5,6 The country continues to comply with the MPOWER measures, a tool designed by the WHO to facilitate the implementation of the convention for Tobacco control (WHO FCTC) in each country. According to the 2021 report on WHO FCTC status, in Colombia the highest level of achievement was assigned to the continuity of bans on tobacco advertising, promotion and sponsorship at cultural and sport events. 31 However, the country still faces significant challenges to implement the WHO FCTC fully. In a 2-year period (2019-2021), Colombia lost its position in the top group of best performance countries to raise tobacco taxes to or above 75% share of total taxes in the retail price of the most widely sold brand of cigarettes. Current tobacco taxation of 73.1% lags behind the 75% taxation rate recommended by WHO mainly due to an increase in cigarette prices above tax increases, leading to a decrease in tax share. 31 In addition, individual cigarettes are still being sold. A national law (Ley 1335) 32 issued in 2009 prohibits the sale of single cigarettes and small packets of cigarettes with enforcement by local health departments and police. However, Colombia’s ongoing internal conflict has forced the police to focus more on public security enforcement, and the number of street vendors who largely sell individual cigarettes remains high. 33
Between 2016 and 2017 the price of a pack of 20 cigarettes increased by 28.2% and by 23.1% for loose cigarettes. 34 As calculated by Gallego and collaborators, this increase would decrease the prevalence of cigarette consumption between 14.6% and 18.1%. 7 Our simulations used a more conservative intervention approach of 10% cumulative decrease in smoking prevalence starting in 2016 and considering no further increments in cigarette prices or taxation. However, considering this more modest reduction in smoking exposure our results showed a decrease of 3.2%, .5%, .2%, and .2% in lung, liver, cervical and colorectal cancer cases, respectively, by 2050. Gallego et al. also calculated the simulated response of smokers to the increase in cigarette prices in Colombia, finding that a 10% increase in the price of cigarettes would lead to a theoretical 66% decrease in the number of tobacco consumers. As Colombians are sensitive to the cost of cigarettes, we consider that prices and shared taxes can be further increased. An additional benefit of reducing of smoking prevalence is the increase in population health and economic paybacks. 35 Overall tobacco-related illnesses represent an annual direct cost to the Colombian health system of more than 4.5 billion Colombian pesos (around 1 billon USD), while the tax collection for the sale of cigarettes that will be used for wellbeing promoting programs barely manages to cover 10% of this expense. 7 Political decisions are needed to continue increasing the prices of tobacco products through taxes and accomplish complete compliance with the MPOWER measures. In the same way, monitoring the use of cigarettes and new tobacco products, such as e-cigarettes, by adolescents should be envisioned since intervention targeting a younger age group can prevent lifelong tobacco use.
Several limitations of this modeling exercise must be acknowledged and the effects of the interventions for smoking reduction modeled should be carefully interpreted. 14 In summary, smoking prevalence data was based on population-based surveys conducted under rigorous study designs but lacked subpopulation and regional differences on smoking consumption. Specific RR estimates of good quality for Colombia are not available but we balance this limitation by using risk estimates from meta-analyses with similar tobacco exposure categories as those available from the National Study of Consumption of Psychoactive Substances in Colombia. 5 Models are a simplified version of reality. Ideally, in this particular study, one would have included the effects of tobacco consumption on life expectancy and population dynamics, including changes in the future population structure. However, the lack of data on the effects of smoking on population dynamics in Colombia, which are already complex because of the strong effects of the armed conflict, would make this exercise even more hypothetical than is currently the case. 13 For instance, an initial study conducted on victims of forced displacement in three major cities showed a prevalence of tobacco smoking during the last year of 14% compared to 12% reported in the general population. 36 Additional data reflecting the direct effects of internal armed conflict in population dynamics and national smoking prevalence stratified by region and age groups would allow better adjusted simulations.
As in any modeling exercise, one must be aware that the projections will never represent the real future cancer burden, as this would depend on other, concomitant processes in the population. However, this exercise has significant strengths useful for understanding the potential magnitude of the effect of population measures aimed to improve public health: we used local age-specific tobacco exposure data as input for modeling and we quantified the relative effects of smoking reduction based on expected decreases on cancer incidence if taxation policies are maintained. We have estimated the number of avoided cancer cases of the lung, liver and colorectal for both sexes and cervix for women in the next 25 years showing the significant population benefit if smoking reduction interventions are continued and reinforced in Colombia.
Conclusion
Although tobacco consumption in Colombia has been gradually reduced over time, it still represents a public health problem due to its causal effect on the development of certain cancers, particularly lung cancer and their associated mortality rate. We showed that both a hypothetical reduction of 10% of smoking prevalence and complete elimination of tobacco exposure over 30 years in Colombia would significantly reduce lung cancer incidence by 2050 and contribute to a modest reduction of liver, cervical and colorectal cancer cases. Current policies and interventions on tobacco control in Colombia have proven to be effective reducing the prevalence of smoking. However, it is necessary to secure and strengthen these programs by increasing the real prices of tobacco products through taxes and by banning advertising, promotion, and sponsorship, which have proven to have a greater impact on reducing tobacco consumption.
Supplemental Material
Supplemental Material - Modelling the Reduction in Cancer Incidence After Variations in the Prevalence of Tobacco Consumption in Colombia in the Period 2016-2050
Supplemental Material for Modelling the Reduction in Cancer Incidence After Variations in the Prevalence of Tobacco Consumption in Colombia in the Period 2016-2050 by Sandra Perdomo, Julián Lopez, Miguel Zamir Torres-Ibargüen, Devi N. Puerto, and Esther de Vries in Cancer Control
Footnotes
Acknowledgments
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy, or views of the International Agency for Research on Cancer/World Health Organization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the Colombian Instituto Nacional de Cancerología E.S.E. (INC) with proper resources in the period 2016-2019 [budgetary code 41030110020 (2016), C190103001-15 (2017-2018). Personnel costs between 2016-2019 were financed by INC without further subsidies. The project was co-financed and co-executed by the Pontificia Universidad Javeriana (Convenio PPTA7602, project medical ethics code 2016/157), and the Universidad El Bosque (Convenio UEB.453-2017), which provided investigator time and resources.
Ethical Approval
The study was reviewed and approved by the Colombian Instituto Nacional de Cancerología E.S.E. (INC) research ethical board (INTOFI079982015).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.