
Abstract
Background
Lebanon has an increasing cancer burden. Sufficient knowledge of cancer risk factors and early cancer symptoms can help lower cancer burden by facilitating primary prevention and early diagnosis. This study (i) assessed Lebanese adults’ knowledge and beliefs of cancer risk factors and early cancer symptoms, (ii) analyzed whether knowledge was correlated with personal behavior, and (iii) assessed the presence of barriers that keep knowledge from turning into healthcare seeking behavior.
Methods
We performed a cross-sectional survey in the Lebanese adult population, consisting of a questionnaire administered during face-to-face interviews on a community-based non-probability sample (n = 726) that was frequency matched to national government estimates on age, level of education and gender.
Results
Recognition was high for carcinogens and protective factors (75%), but low for neutral factors (22%) which were often seen as carcinogenic. A quarter of participants (27.8%) could not name any early warning signs. For some risk factors, high knowledge scores were correlated with low-risk behavior, but this was not the case for cigarette smoking. The most frequent barriers for not seeking timely care were financial (57.0%) fear of finding illness (53.7%), and having other things to worry about (42.4%).
Conclusion
This study revealed important knowledge gaps which are likely to hamper primary prevention and early diagnosis. However, we also showed that high knowledge of risk was not always correlated with low-risk behavior. This, together with the barriers we found that kept people from seeking timely health care, emphasizes that efforts to lower cancer burden should not only focus on increasing knowledge.
Keywords
Background
Lebanon has the highest cancer incidence rates in the Eastern Mediterranean Region and is in the top quartile of cancer incidence worldwide. 1 The most common cancers among Lebanese males are prostate cancer (17.7%), followed by lung cancer (15.4%), colorectal cancer (9.6%), and bladder cancer (8.0%). The most common cancers among Lebanese females are breast cancer (33.7%), lung cancer (8.7%), colorectal cancer (6.0%), and thyroid cancer (5.2%). These top 4 locations account for more than half of all cancers (50.7% for males, 53.6% for females). 2 Although cancer burden is projected to increase over the next years, primary prevention, screening, and early diagnosis can help lower cancer burden. 3
Primary Prevention
A third (33%) of all cancers in adults in the Eastern Mediterranean Region can be avoided because avoidable carcinogenic factors in our lifestyle are the driving force behind them (such as tobacco, alcohol, and low physical activity).4-7 Eliminating these carcinogenic factors (primary prevention) is therefore an effective tool to lower cancer burden. This requires that the population has sufficient knowledge of these cancer risk factors, while barriers that keep this knowledge from turning into action are simultaneously minimized. 8 Research that assessed knowledge and beliefs of cancer risk factors in Lebanon is scarce. Although some local and national organizations had initiatives to increase knowledge, but exposure to lifestyle risk factors is increasing rather than decreasing.2,6,9 Previous studies found that only 34% of Lebanese adults were aware of the cancer risks of human papillomavirus (HPV), 10 36.5% are aware that physical inactivity is a risk factor for colorectal cancer, 11 alcohol is identified as a risk factor for colorectal cancer by 52.8% of Lebanese adults, 11 51.4% of Lebanese adults are aware that being overweight is a risk factor for cancer, 12 and only 30.1% know tobacco is the biggest risk factor for bladder cancer. 13
Screening and Early Diagnosis
Screening (diagnosing illness before symptoms are present) and early diagnosis (diagnosing illness at the first sign of symptoms) also have the potential to lower cancer burden. World Health Organization (WHO) recommends that countries use early diagnosis for all cancers. 4 In order for a population to use screening and early diagnosis, knowledge of cancer, the possibility of screening, and early cancer symptoms should be optimized. At the same time, barriers to care that could keep this knowledge from turning into action need to be minimized (financial, logistical, or psychosocial barriers that keep someone from seeing a doctor).8,14,15
Research that investigated barriers to cancer screening in Lebanon found that 63.6% of the Lebanese citizens were aware of the screening program for breast cancer and 40.8% was aware screening for cervical cancer is possible. 15 Those results were in line with the weighted national prevalence of “ever-use” of the Pap smear for screening purposes, which was estimated at 35%. 16
Aim
This study aimed to (i) assess Lebanese adults’ knowledge and beliefs of cancer risk factors and early cancer symptoms; (ii) analyze whether knowledge of the risk posed by cigarettes, waterpipe, alcohol, and lack of physical exercise is correlated with personal behavior on those factors; and (iii) assess the presence of barriers that keep knowledge of early cancer symptoms from turning action (seeking health care for early diagnosis).
Materials and Methods
We performed a cross-sectional survey in the general adult population in 2019. The survey consisted of a questionnaire that was administered by investigators during face-to-face interviews. A non-probability sample (n = 726) was frequency matched to national government estimates on age, level of education, and gender. The study was approved by the ethical committee of the University Hospital of Brussels.
Setting and Participants
Sampling took place in the Beirut and Mount-Lebanon, 2 governorates that together host half of the Lebanese population. Sampling stations included places with varying socio-economic characteristics such as gyms, medium size malls, community-based pharmacies, churches, mosques, tea houses, and public markets. Recruitment took place after obtaining permission and support from municipal authorities and people in charge of the sampling location, on any day of the week and at different times of the day. During recruitment, an interviewer would approach people in the sampling station and provide information about the study (see section on ethical considerations). Inclusion criteria were having the Lebanese nationality and being adult (defined as ≥20 years old to allow distribution comparison between sample and government data). Exclusion criteria were severe hearing or speaking difficulties. All refusals were registered. No financial incentives were provided.
Instrument
The questionnaire was based on two existing validated English language measures of cancer awareness (the UK Cancer Awareness Measure and the US Health Information National Trends Survey).17,18 We performed forward and backward translation to Modern Standard Arabic and made some adaptations to include culturally specific elements such as use of waterpipe, which has been shown to be carcinogenic. 19 The resulting questionnaire was pretested by performing in-depth interviews with 5 persons, after which appropriate clarifications were made. 20
The questionnaire included questions on knowledge and beliefs of cancer risk factors, personal behavior regarding risk factors, knowledge and beliefs of early cancer symptoms, barriers to seeking timely care, and sociodemographic characteristics (age, gender, employment, marital status, highest education).
Knowledge and beliefs of cancer risk factor was first evaluated in an open-ended recall question (what do you think are the biggest risk factors for developing cancer?). Next, we presented a recognition question with 24 factors for which we asked, “Do you think any of these can influence someone’s risk of developing cancer?” Among these 24 factors were 14 that the International Agency for Research on Cancer classified as carcinogenic, 7 that are classified as having no influence on cancer risk, and 3 that lower cancer risk (see Table 4). 21
There were 8 answering options: I do not know; neither increases nor decreases, increases risk strongly/moderately/somewhat, decreases risk strongly/moderately/somewhat. All 3 “increase” options were counted as correct answers for the 14 carcinogens, the option “neither increases nor decreases” was counted as correct for the 7 factors that do not influence risk (we refer to these as neutral factors), the 3 “decrease” answer were counted as correct for the 3 protective factors.
Knowledge and beliefs of early cancer symptoms were evaluated in an open-ended recall question (Please name early warning signs of cancer, as many as you can think of). The authors from the UK Cancer Awareness Measure have previously categorized these signs into 2 groups: key cancer symptoms (lump, bleeding, changing bowel habits) and vague cancer symptoms (cough, weight loss, tiredness, loss of appetite), and we used the same categorization.
Lifestyle behavior questions were close-ended questions that enquired about the amount of daily exercise, consumption of waterpipe, cigarettes, and alcohol.
Barriers to seeking timely care were assessed in close-ended questions in which we presented 10 statements and asked, “Would any of the following keep you from seeking medical care?” (5-point Likert scale answers).
Sample Size
Epi-info was used to calculate the required sample size, using the following equation

Statistical Analysis
Data were analyzed using Stata version 13 (StataCorp, USA). Answers to the open-ended questions on cancer risk factors and early cancer symptoms were categorized, and the proportion of each category was calculated against the total number of participants. For the 24 closed-ended risk factor recognition questions, the proportion of people that recognized a factor correctly was calculated against the total number of participants for each factor. The chi-square test was used to compare this proportion between men and women with significance set at P < .05. The arithmetic mean of the 24 factors was also calculated for the 14 carcinogens as a group, for the 7 neutral factors as a group, and for the 3 protective factors as a group.
Per lifestyle behavior (alcohol, physical exercise, waterpipe, and cigarettes), an ordered logistic regression was run in which the answers to the lifestyle behavior question were used for the dependent variable, and the answers to the risk perception question were used as independent variable, together with gender and age (two demographic variables which have previously been shown to be correlated to behavior). Significance was set at P < .05. In case a significant correlation was found, we tested the proportional odds assumption through a likelihood ratio test with the user-written command called omodel with significance set at P < .05. 22
For the 10 closed-ended recognition questions regarding barriers that keep adults from seeking timely care the answers “I agree completely” and “I agree somewhat” were grouped together, and the proportion of this sum was calculated against the total number of participants. The chi-square test was used to compare this proportion between men and women with significance set at P < .05.
Ethical Considerations
Informed consent was sought from every participant by explaining the objectives of the study, that participation was voluntary, that anonymity of the participants was guaranteed and that withdrawal at any point was possible. The study was approved by the ethical committee of the University Hospital of Brussels with reference number CAL-3.1.
Results
Characteristics of Participants
Distribution of socio-demographic characteristics among participants and the general population.
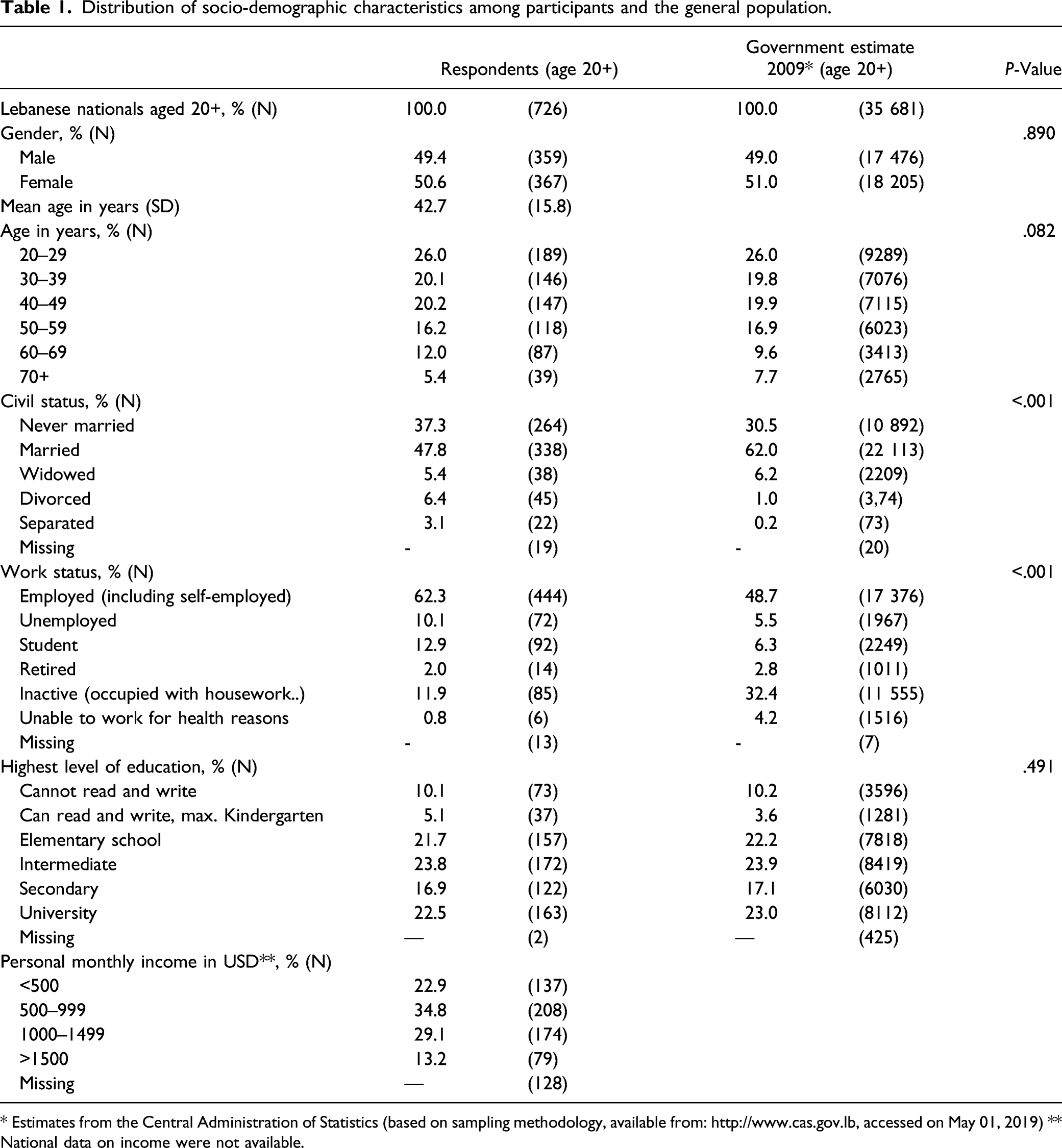
* Estimates from the Central Administration of Statistics (based on sampling methodology, available from: http://www.cas.gov.lb, accessed on May 01, 2019) ** National data on income were not available.
Knowledge and Beliefs of Cancer Risk Factors
Factors Lebanese adults recall as the most important causes of cancer (Lebanon, 2019).

Correct recognition of the role of lifestyle factors and aging in cancer risk (Lebanese adults, Lebanon, 2019).
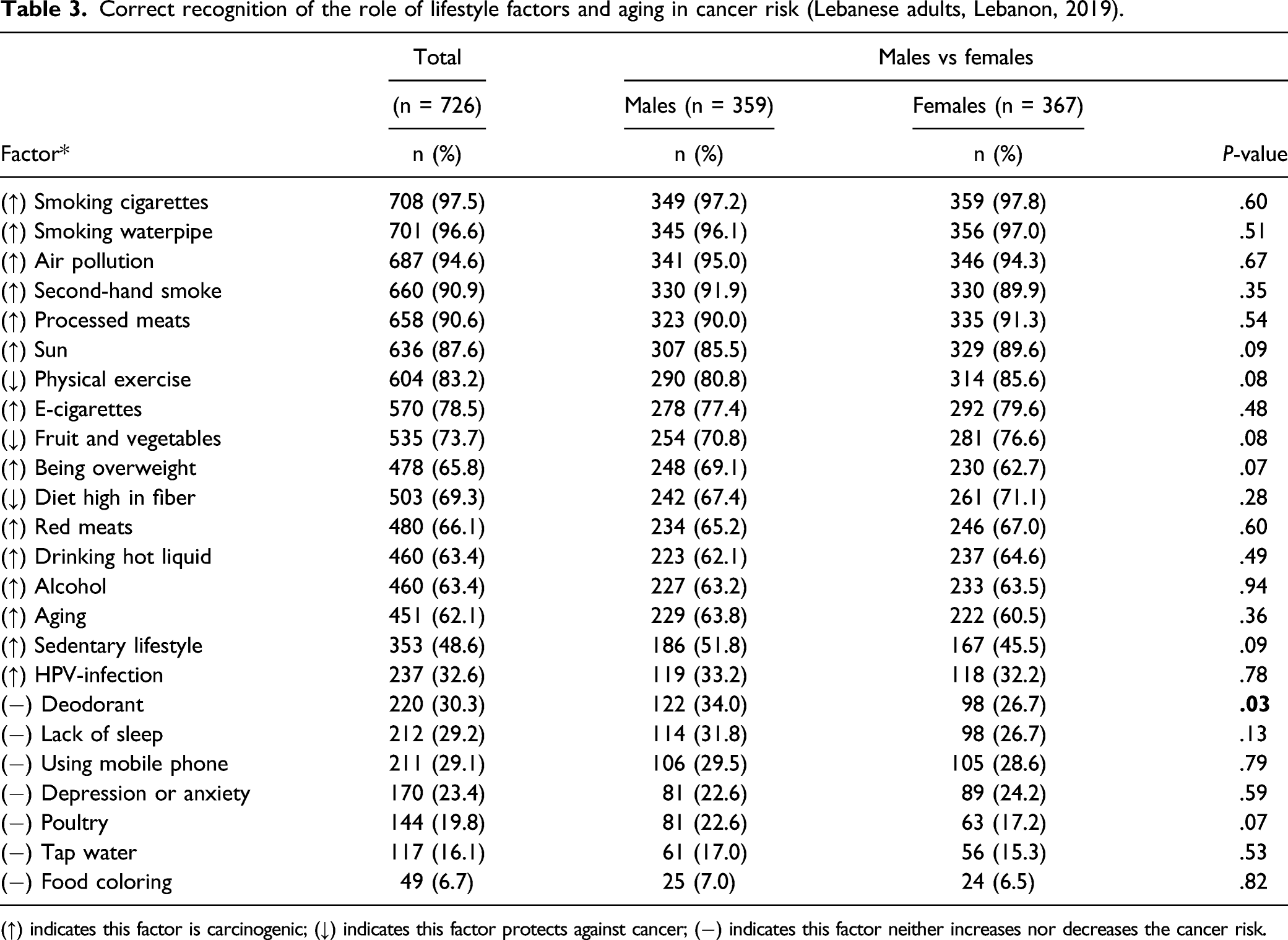
(↑) indicates this factor is carcinogenic; (↓) indicates this factor protects against cancer; (−) indicates this factor neither increases nor decreases the cancer risk.
The only factor for which results differed significantly between men and women was deodorant. While 73.3% of women incorrectly attributed carcinogenic properties to deodorant, men did so less often (69.7%, P = .03).
Correlation Between Risk Factor Knowledge and Personal Behavior
Correlation between knowledge and behavior. (Lebanese adults, Lebanon, 2019).

Knowledge and Beliefs of Early Cancer Symptoms
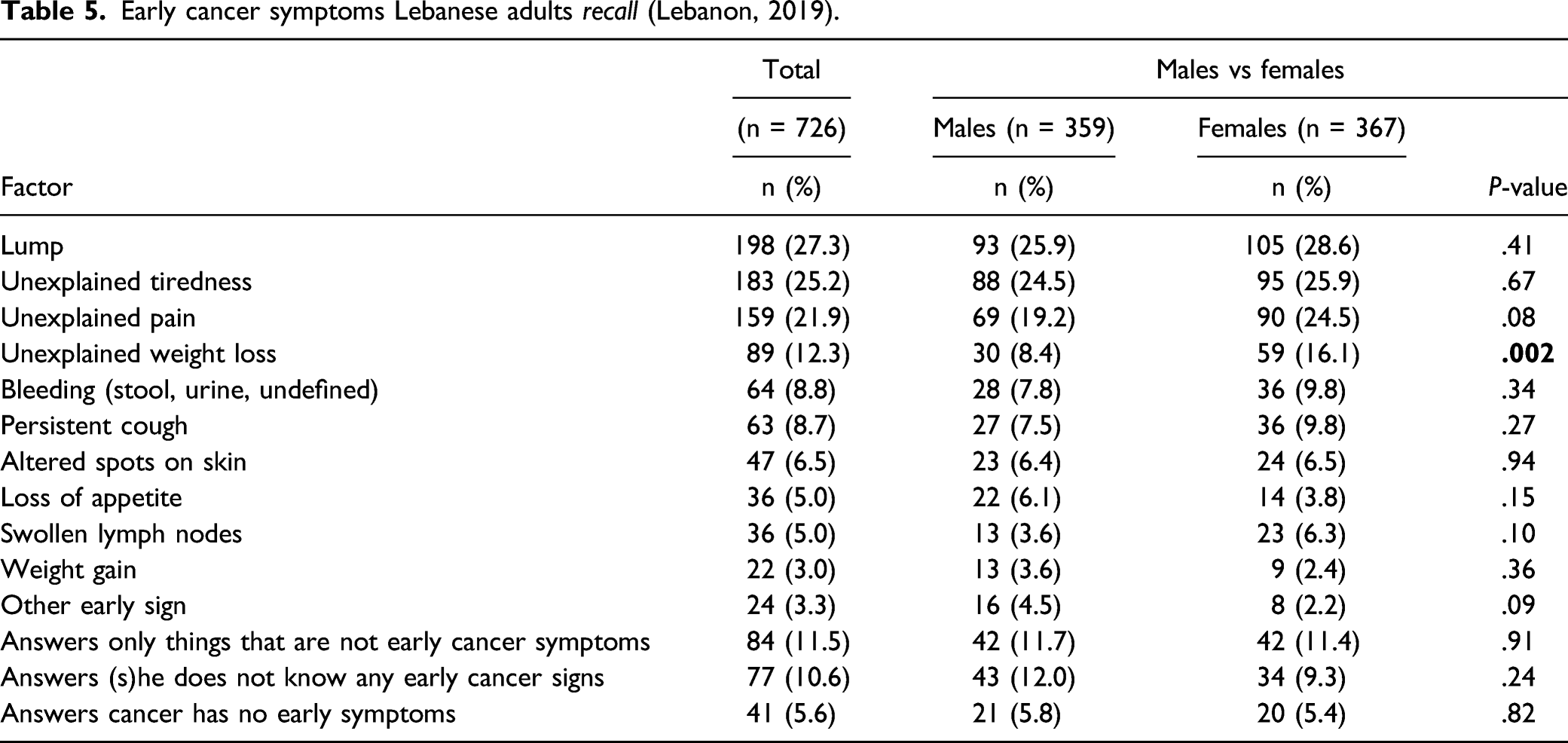
Early cancer symptoms Lebanese adults recall (Lebanon, 2019).
Barriers That Keep Knowledge of Early Cancer Symptoms From Turning Into Action
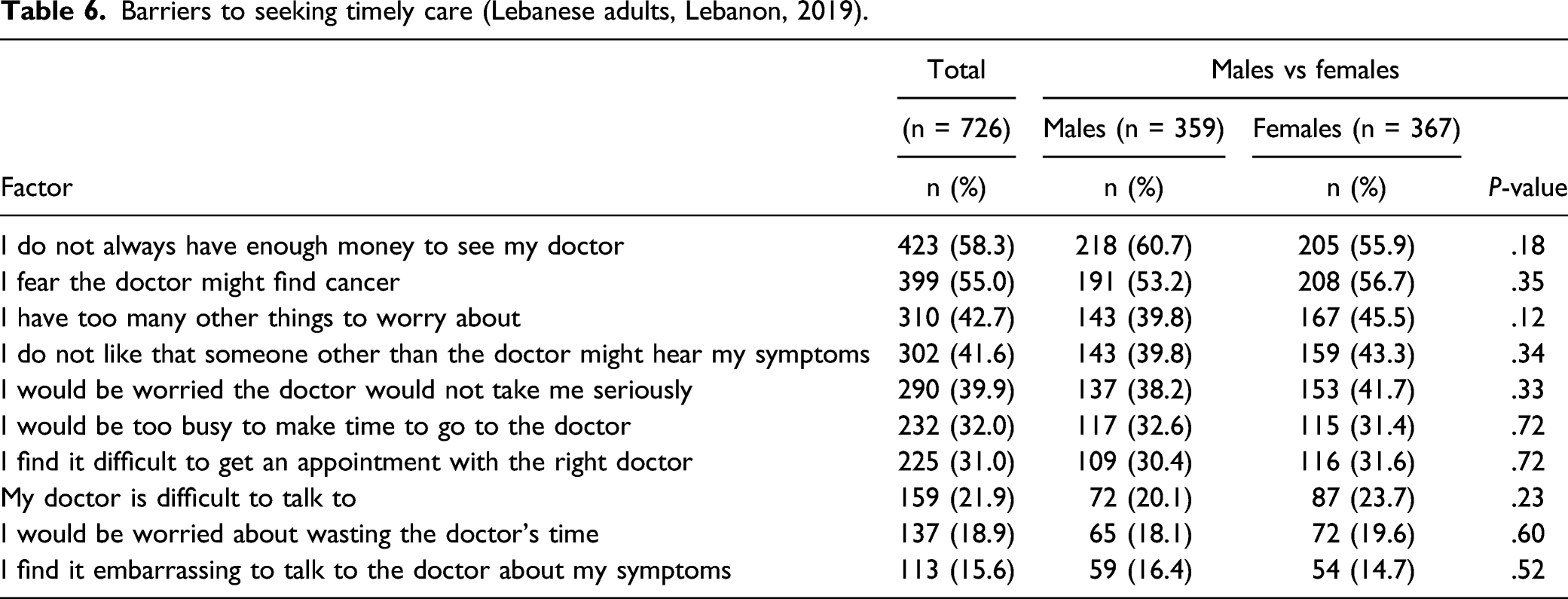
Barriers to seeking timely care (Lebanese adults, Lebanon, 2019).
Discussion
Knowledge of Cancer Risk Factors and Correlation Between Knowledge and Behavior
Overall, it is comforting that smoking was identified as the prime lifestyle carcinogen in both recall and recognition questions and that many other carcinogens were also correctly recognized. Cigarettes and waterpipe were recognized as carcinogenic by over 95% of participants and were the most mentioned factor on recall, which is comparable to results in the UK. 23 The exceptions to high knowledge of carcinogens (less than 50% classified them as carcinogenic) were HPV (32.6%) and physical inactivity (48.6%). Previous research in Lebanon also found tobacco to be far more known as a carcinogen than other factors such as lack of exercise and being overweight. 24
The striking lack of knowledge about HPV confirms earlier research that found only 24.8%–34% of adults were aware of the cancer risks of HPV.10,15 We only investigated knowledge of HPV itself, but future research should also look into knowledge of the HPV vaccine since HPV vaccination is an important aspect of primary prevention for HPV-related cancers and knowledge of this vaccine has previous been shown to be low. 24
The lack of knowledge about the risk of a sedentary lifestyle (48.6%) confirms earlier research that found that only 36.5% of adults see it as a risk factor for colorectal cancer. 11
Alcohol and aging (respectively recognized as a carcinogen by 63.4% and 62.1%) were the other least known carcinogenic risks. This confirms previous research that found 52.8% of Lebanese identified alcohol as a risk factor for colorectal cancer and 25.4% see advanced age as a risk factor for cancer. 11
More worryingly, factors that do not influence cancer risk were incorrectly recognized as carcinogenic by a large percentage of people (food coloring: 93.7%; tap water: 83.9%; depression and anxiety: 76.6%). Similarly, non-carcinogenic factors were also mentioned as important causes of cancer in the recall question: depression and stress (7.6%) and a variety of foods (6.8%). Attributing a carcinogenic effect to a non-carcinogenic factor has been observed in other countries as well. 25 Social media may be at least partly responsible for spreading such cancer myths and can therefore also be used to counter the myths. 25
Higher knowledge of risk was moderately correlated with beneficial behavior for waterpipe, alcohol and physical activity, suggesting that a well-designed knowledge campaign could be effective to reduce exposure. Such a correlation was not detected for cigarette smoking, which confirms previous research that also found a large gap between knowledge and behavior.26-28
Knowledge and Beliefs of Early Cancer Symptoms and Barriers That Keep Such Knowledge From Turning Into Action
Recall of key early warning signs was low in our study especially when compared to results of the UK. Our results are very similar to previous research on recall of early warning signs in Lebanon and can also be compared to recall results from the Gaza strip: (i) a lump was the most recalled symptom (27.3% in our study, 23.5% in previous Lebanese research, 59% in the UK, and 39.7% in the Gaza strip), followed by (ii) unexplained bleeding (8.8% in our study, 4.4% in previous Lebanese research, 35% in the UK, and 6.5% in the Gaza strip), and (iii) altered spots on skin (6.5% in our study, 2.2% in previous Lebanese research, and 18% in the UK).15,23,29
Vague symptoms were also less known then in the UK, but very comparable to previous Lebanese research: (i) unexplained pain (21.9% in our study, 22.9% in previous Lebanese research, 34% in the UK, and 18.7% in the Gaza strip), (ii) persistent cough (8.7% in our study, 4.1% in previous Lebanese research, 24% in the UK, and 2.2% in the Gaza strip), and (iii) weight loss (12.3% in our study, 9.4% in previous Lebanese research, 26% in the UK, and 19.7% in the Gaza strip). Interestingly, there were two vague warning signs that were more known in our study than in the UK: loss of appetite (12.3% in our study vs 7% in the UK) and tiredness (25.2% in our study vs 16.0% in the UK).15,23,29
The most often mentioned barrier to consulting a physician were of a financial nature (58.3%), fear of finding illness (55.0) and having many other things to worry about (42.7%). This confirms previous Lebanese research (respectively, 67.7%, 34.2%, and 28.2%). 15
Possible Aspects of Future Strategies to Promote Primary Prevention and Early Diagnosis
Well-timed and evidence-led campaigns will be useful to raise knowledge about cancer risks, cancer myths, and cancer early warning signs, which will benefit any efforts to promote primary prevention and early diagnosis. Information material of the International Agency for Research on Cancer (www.euro.who.int, European Code against Cancer) and Cancer Research UK (https://www.cancerresearchuk.org/about-cancer/cancer-symptoms) could, for instance, be translated to the Lebanese dialect.
However, such campaigns need to be embedded in behavior change programs that also address other barriers to change. This is exemplified by our findings of a gap between knowledge and behavior and the existence of non-knowledge based barriers. Inspiration for such a multifaceted approach can be found in “Europe’s Beating Cancer Plan” or from previous research and include, for instance, (i) increasing taxes on tobacco, alcohol, and high-calorie foods; (ii) decreasing taxes on healthy choices such fruits and vegetables, bikes, and gyms; (iii) smoking bans; (iv) reducing young people’s exposure to online marketing and advertising of unhealthy food products such as alcohol and high-calorie food or drinks; (v) mandatory labeling of alcoholic beverages for ingredients, nutrient content, and health warnings; (vi) encouraging schools to eliminate sales of high-calorie drinks and snacks and instead promote the sales of fruits and vegetables on their premises; and (vii) working with celebrities through social media to deal with low knowledge levels.30-32
Another important tool to lower cancer burden is screening (screening means to diagnose cancer before symptoms are present, as opposed to early diagnosis which means diagnosis is made when the first symptoms appear). Awareness campaigns have in the past succeeded in increasing breast cancer screening uptake, suggesting that future strategies to lower cancer burden should include raising awareness for cancer screening. 33 At the moment, national screening programs in Lebanon are limited to breast cancer. Although assessing the level of knowledge of participants regarding screening was out of scope of the current study, previous research revealed significant knowledge gaps regarding screening and that knowledge about breast cancer screening was among higher than for other types of screening. 24
Strengths and Limitations
Our study had some major strengths. We based our questionnaire on a validated measure of cancer knowledge and beliefs, managed to reach the lower socio-economical groups, had less than 15% of refusals to participate, and had very few missing data (except for the variable personal income). Our population-based sample was also frequency matched to important demographic variables. Although this method is inferior to a random sampling design, it is more likely to give representative results compared to a non-random sampling method that neither checks nor adjusts for population distribution. However, our study also has limitations. Recall and recognition are different methods of measuring cancer knowledge and beliefs; recall is thought to underestimate knowledge and beliefs, while recognition is thought to overestimate it. 34 Of the eight Lebanese governorates, our sample strategy included only two (mainly urban). Therefore, it cannot be guaranteed that our results are generalizable to Lebanon as a whole, although our sample was matched to national data on socio-economic variables. It would also have been interesting to also address the level of knowledge of participants regarding screening for cancer. Although this was out of scope of the current study, we recommend pursuing this topic in future research since screening is an important tool in lowering cancer burden.
Conclusion
This study revealed important knowledge gaps which are likely to hamper primary prevention and early diagnosis. Well-timed and evidence-led campaigns are needed to raise knowledge about cancer risks, cancer myths, and cancer early warning signs. However, we also provided two reasons why future information campaigns need to be embedded in behavior change programs that also address other barriers to change: (i) high knowledge of risk was not always correlated with low-risk behavior and (ii) we found barriers which keep people from seeking timely health care but which have nothing to do with a lack of knowledge.
Footnotes
Acknowledgments
The authors would like to thank Jon Shelton, Briony Hudson, Brigitta Boonen, and Sacha Hatem for their valuable contributions.
Authors’ contributions
Georges Hatem, Diana Ghanem, Ibrahim AlZaim, Eliane Kellen, and Mathijs Goossens contributed to the design of this study, the analysis of its data and the writing of the article. All authors reviewed the final version of the submitted article and approved it for publication. Georges Hatem, Diana Ghanem, and Ibrahim AlZaim oversaw data collection. Georges Hatem prepared the tables together with Mathijs Goossens.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethical committee of the University Hospital of Brussels with reference number CAL-3.1. All procedures performed involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was sought from every participant by explaining the objectives of the study that participation was voluntary, that anonymity of the participants was guaranteed, and that withdrawal at any point was possible.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.