
Abstract
Human epidermal growth factor receptor 2–positive breast cancer (HER2+BC) is a common malignancy that is prone to recurrence and metastasis in the early stages, resulting in a poor prognosis for patients. Many studies have suggested that targeted therapy promotes clinical outcomes in HER2+BC. With the introduction of trastuzumab in 1998, the prognosis of patients with early HER2+BC has improved significantly. However, owing to obstinate drug resistance and adverse events, the addition of new agents in standardized treatment has become a research hotspot. These promising agents include antibodies, antibody-drug conjugates, tyrosine kinase inhibitors, and anti-HER2 combined therapies. This article provides a brief description of the biology of BC and the expression of HER2, with the aim to provide an overview of the therapeutic landscape of HER2+BC by reviewing research results and introducing the latest evidence to provide a reference for clinical treatment.
Keywords
Introduction
Breast cancer remains the primary disease burden in women worldwide.
1
Breast cancer can be divided into several subtypes, with different subtypes leading to different therapeutic sensitivities and prognoses.
2
HER2 is overexpressed in 15%–20% of all breast cancers plays an indispensable role in the progression of breast cancer.
3
As a result, HER2 is regarded as an effective target for the genomic therapy of various tumors.
4
By forming homodimers or heterodimers, HER2 can drive tumor growth and activate downstream signaling pathways, which promote cell proliferation, survival, and angiogenesis.
5
HER2-targeted therapy has been authorized by the Food and Drug Administration (FDA) because it greatly improves the prognosis of HER2-positive breast cancer (HER2+BC). Chemotherapy plus 1 year of adjuvant HER2-targeted therapy is the standard regimen for HER2+BC. Trastuzumab is the most typical HER2-targeted agent, and the use of trastuzumab in 1998 inspired patients with HER2+BC. For metastatic breast cancer (MBC) with HER2 overexpression, trastuzumab enhances the clinical benefits of chemotherapy.
6
Moreover, the addition of trastuzumab has been shown to halve the recurrence rate in patients with HER2+BC.
7
Although the treatment is valid, some obstinate drug resistance and AEs associated with trastuzumab affect the quality of life of patients during the course of treatment. Therefore, several targeted agents have been explored and approved in recent decades (Figure 1). Further enhancement of the effect of targeted therapy has become the focus of research into HER2+BC. Therefore, there is an urgent need to develop novel and acceptable targeted agents for patients.
8
Timeline of the findings of HER2 and the development of HER2-positive breast cancer regimens. HER: Human epidermal growth factor receptor, EGF: Epidermal growth factor, EGFR: Epidermal growth factor receptor, TDM-1: Ado-trastuzumab emtansine, BC: Breast cancer, FDA: Food and Drug Administration, DS-8201: Trastuzumab deruxtecan.
This article provides a brief description of the biology of BC and the expression of HER2, with the aim to provide an overview of the therapeutic landscape of HER2+BC by reviewing research results and introducing the latest evidence to provide a reference for clinical treatment.
Breast Cancer Biology and Expression of HER2
Four Molecular Subtypes of Breast Cancer.

Abbreviation: ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor.
HER2 oncogenes are located on chromosome-17
11
and are responsible for encoding transmembrane receptor tyrosine kinases.
12
The HER2 oncogene is a member of the epidermal growth factor receptor (EGFR) family (also known as ErbB), together with HER1, HER3, and HER4 (Figure 2). By forming homodimers (with HER2) or heterodimers (with HER1, HER3, or HER4), tyrosine residues in the cytoplasmic domain undergo autophosphorylation, which activates downstream signaling pathways (mainly the PI3K/AKT/mTOR and Ras/Raf/MEK/MAPK pathways) and causes adverse biological reactions (Figure 3). HER2 amplification is defined as a vital independent adverse prognostic factor,
13
and HER2+BC is more invasive and more likely to relapse and metastasize in the early stage.
14
Liner structures and corresponding ligands of the epidermal growth factor receptor family. EC: Extracellular domain, TM: Transmembrane domain, D: Domain. IC: Intracellular domain, TK: Tyrosine kinase domain, APR: Amphiregulin, NRG: Neuregulin, BTC: Betacellulin, HER: Human epidermal growth factor receptor, EPR: Epiregulin. Biological mechanism of HER2 and summary of targeted therapies for HER2-positive breast cancer. HER: Human epidermal growth factor receptor, ADCs: Antibody-drug conjugates, TKI: Tyrosine kinase inhibitor, CAR: Chimeric antigen receptor, CD3: Cluster of differentiation 3, TCR: T-cell receptor, PD-1: Programmed death-1, PD-L1: Programmed death-ligand 1, TDM-1: Ado-trastuzumab emtansine, DS-8201: Trastuzumab deruxtecan.

Summary of Major Phase III trials in HER2+BC.

Abbreviation: C, group of control; E, group of experiment; NA, not available; NCT, National Clinical Trial; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; T, total numbers; TDM-1, ado-trastuzumab emtansine.
Therapeutic Antibodies
Several novel antibodies have been identified. Compared to trastuzumab, they either have greater specificity to combine with the HER2 receptor, or they can bind to extra epitopes to enhance activity and generate greater immunologic responses.
Pertuzumab
Pertuzumab is a humanized recombinant monoclonal antibody. In addition to preventing the formation of homodimers and triggering antibody-dependent cell-mediated cytotoxicity (ADCC), which is also triggered by trastuzumab, pertuzumab can combine with HER2 in other regions, restrain the heterodimer (HER2/HER3), and block downstream signaling pathways (Figure 3).16,17
Pertuzumab was first found to be useful in MBC with a combination of trastuzumab and docetaxel in the CLEOPATRA study. The study showed that the regimen extended the median progression-free survival (PFS) to 18.5 months compared to 12.4 months in the placebo group. 18 Later, to determine whether pertuzumab played a role in neoadjuvant therapy of HER2+BC, a phase II trial, NeoSphere, was conducted. 19 The results showed a significantly higher pathologic complete response (pCR) in the treatment group than that in the placebo group (45.8% vs 29.0%; P = .014). It is worth mentioning that the PEONY study, which was conducted in Asians, also confirmed that the application of pertuzumab in neoadjuvant therapy was beneficial in patients with HER2+BC. 20
APHINITY, a phase III clinical trial, showed that pertuzumab could lower the risk of invasive disease-free survival (iDFS) compared to placebo (hazard ratio [HR] = .81; 95% confidence interval [CI], .66–1.00; P = .045). Therefore, pertuzumab has been approved as an adjuvant treatment for HER2+BC. 21 In addition, the regimen (trastuzumab plus pertuzumab and docetaxel) could extend the overall survival (OS) to 56.5 months in patients with HER2+MBC. 22 It is worth noting that this regimen is relatively safe and does not cause additional cardiotoxicity.
According to the latest National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology (Version 2.2022), trastuzumab and pertuzumab combined with chemotherapy are the first-line regimens for neoadjuvant chemotherapy. 23 However, there is no precise evidence to support whether the regimen is useful for patients with tumors <2 cm in diameter and without axillary lymph node metastasis.
Margetuximab
Margetuximab (MGAH22) is a chimeric murine monoclonal antibody. Unlike trastuzumab, MGAH22 is designed with an engineered Fc portion to increase affinity for the activating Fcγ receptor and to decrease affinity for the inhibitory Fcγ receptor, thereby increasing the ADCC response. 24 In a phase I trial, MGAH22 exhibited antitumor activity and no cardiotoxicity in patients treated with anti-HER2 therapy. 25 A crucial phase III trial, SOPHIA, showed that the regimen of MGAH22 plus chemotherapy improved PFS compared to the trastuzumab group (HR = .76; 95% CI, .59–.98, P = .03). 26 As a result, MGAH22 combined with chemotherapy has been approved by the FDA for the treatment of HER2+MBC. Further phase II trials, such as MARGOT and NCT04262804, are currently recruiting volunteers. 27
ZW25
ZW25 is a bispecific antibody; in contrast to trastuzumab, ZW25 can combine two HER2 epitopes simultaneously to increase specificity and improve efficacy (Figure 3). In most HER2-overexpressed cancers, ZW25 shows high activity in vivo and in vitro. 28 In a phase I clinical trial, ZW25 was effective in patients with HER2+BC, with a 33% objective response rate (ORR). 29 Recently, a phase I/II trial (NCT02892123) has been conducted. Part 1 was completed with no dose-limiting toxicity, but two common AEs were reported - diarrhea and infusion-related reaction (all grade 2). In part 2, 13 patients with MBC were included in the study, seven of whom improved and six failed. In part 3, which is ongoing, scientists will assess the safety, tolerance, and efficacy of the combination with specific chemotherapy. 30
MM-111
Unlike the HER2/HER2 homodimer regulated by trastuzumab, MM-111 is a fusion antibody consisting of fully human anti-HER2/HER3 single chains linked by modified human serum albumin. It precisely obstructs the combination of heregulin (HRG) and HER3, and blocks ligand-induced signaling and tumor growth. A series of preliminary studies have evaluated the curative effect of MM-111 in the regimen of patients with HER2-positive solid tumors, such as MM-111 monotherapy (NCT00911898), MM-111 plus trastuzumab and chemotherapy regimen (NCT01304784), and MM-111 plus trastuzumab and lapatinib regimen (NCT01097460). 31
MCLA-128
MCLA-128 is a humanized bispecific antibody that contains two arms (“dock” HER2 arm and “block” HER3 arm) and targets extracellular domains, which prevents the phosphorylation of HER3 and downstream oncogenic signaling. 32 In a phase I trial, large doses of MCLA-128 were administered to ten patients with breast cancer, and the results revealed a considerable clinical benefit rate of 70%. Another phase II trial (NCT03321981) is proceeding. 33
Ertumaxomab
The trifunctional immunoglobulin ertumaxomab is an integrated bispecific antibody. 34 Traditional treatment with trastuzumab only affects the EGFR family; however, ertumaxomab can simultaneously target HER2 and cluster of differentiation 3 (CD3) presented on T cells, and activate Fcgamma receptors of innate effector cells. According to these characteristics, ertumaxomab acts as a bridge between tumor cells and immune cells. ADCC can be enhanced by activating the adjunctive cells. In addition, they can relate immune effector cells and tumor cells in a short time and display powerful antineoplastic activity. 35 A phase I trial confirmed that ertumaxomab resulted in one complete response (CR) case and several partial response (PR) cases. A maximum tolerated dose of 100 μg is recommended, and cytokine release is the most related AE. 36 Phase II trials concerned with ertumaxomab (NCT00522457, NCT00452140) were terminated because of changes in the development plan or focus on other projects. Although there is currently no clear conclusion, ertumaxomab could still be an appropriate adjuvant for anti-HER2 therapy.
Antibody-Drug Conjugates (ADCs)
ADCs transmit different cytotoxic drugs to tumors using mAbs. These drugs not only decrease toxicity in normal tissues, but also have increased targeting ability and efficiency. Ado-trastuzumab emtansine (T-DM1) is a representative drug approved by the FDA for the treatment of HER2+MBC, and is composed of cytotoxic agents such as trastuzumab and emtansine. 37 Because T-DM1 combines with HER2, the conjugate can be transported into tumor cells. Subsequently, emtansine is released, which causes the inhibition of tubulin and finally leads to apoptosis. 38 In addition, T-DM1 can block downstream signaling pathways (Figure 3). 39 Phase I/II trials have demonstrated that the addition of TDM-1 results in an excellent response, with better ORR and PFS. 40 EMILIA was a critical phase III trial, which showed that T-DM1 plus capecitabine significantly lengthened the median PFS and OS (HR = .53; 95% CI, .37-.76; P < .05). Based on these results, T-DM1 gained acceptance and was used as a second-line treatment for HER2+MBC patients. 41
Summary of Novel ADCs Applied in HER2-Positive Breast Cancer.
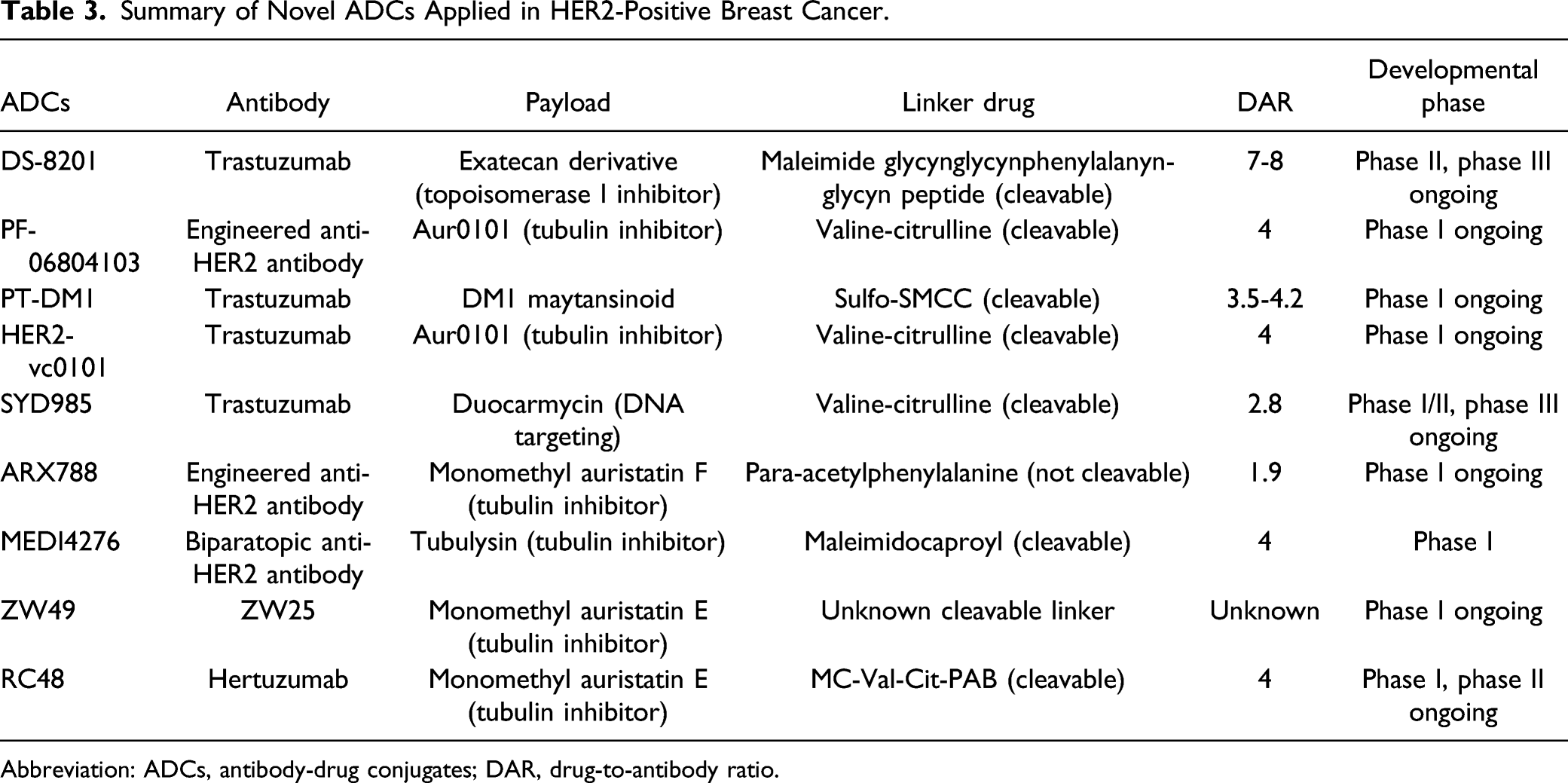
Abbreviation: ADCs, antibody-drug conjugates; DAR, drug-to-antibody ratio.
Tyrosine Kinase Inhibitors (TKIs)
TKIs are suitable candidates for the treatment of various malignancies. They bind to tyrosine kinases competing with adenosine triphosphate (ATP), inhibit phosphorylation of residues, and block downstream signaling pathways, all of which suppress tumor cell proliferation and metastasis (Figure 3). Therefore, TKIs may be beneficial in patients with early HER2+BC. To date, two HER2-targeted TKIs have been approved by the FDA: lapatinib and neratinib, while several novel TKIs are currently undergoing clinical research. 48 While it is difficult for monoclonal antibodies to traverse the blood–brain barrier (BBB), some TKIs can cross easily, which may represent an effective solution for the metastasis of the central nervous system (CNS) in HER2+BC. 42
Lapatinib
The FDA-approved lapatinib is an effective oral TKI. It can reversibly inhibit HER1 and HER2 receptors, block the downstream pathways (mainly PI3K/AKT/mTOR and Ras/Raf/MEK/MAPK pathways), and ultimately inhibit the proliferation and development of tumor cells. 49 According to the FDA, the regimen of lapatinib plus capecitabine is effective in patients with MBC. As lapatinib can cross the CNS, it has the potential to improve the prognosis of CNS MBC. 50 Studies have shown that short-term treatment with lapatinib (1-7 days) induces cell cycle arrest, apoptosis, and autophagy. However, long-term treatment (3-6 months) may result in acquired drug resistance. 51 Unfortunately, its well-known AE, diarrhea, limits its clinic use. 52
Neratinib
Neratinib is an FDA-approved oral TKI, which irreversibly inhibits members of the EGFR family (except HER3). Compared to lapatinib, neratinib is more valid and consistent. 53 By lowering the phosphorylation of each protein kinase domain, it blocks downstream pathways, which eventually decreases both cyclin D1 expression and RB phosphorylation. 54 As neratinib and trastuzumab have different mechanisms, their combination may be promising. 55
A phase II trial, NEFERT-T, showed that the administration of neratinib led to fewer CNS recurrences. The most frequent AE was diarrhea (20%, grade 3-4). 56 A phase III trial named NALA confirmed that a regimen of neratinib plus capecitabine could lower the cumulative incidence of CNS metastasis. 57 Another phase III trial, ExteNET, explored patients with 1-year neratinib treatment followed by 1-year trastuzumab treatment. In the 5-year follow-up study, the neratinib group showed a survival rate of 90.2%, while the placebo group showed a survival rate of 87.7%, confirming its clinical efficacy. In addition, subgroup analysis suggested that the sequential use of neratinib was more beneficial for hormone receptor (HR)-positive patients. 58
Pyrotinib
Pyrotinib was developed exclusively in China and has similar biological mechanisms to neratinib. 59 Phase I trials showed that a single application of pyrotinib was efficient and safe for patients with advanced HER2+BC. 60 A recent randomized phase II trial (NCT02422199) assessed the clinical efficacy of pyrotinib plus capecitabine, and the results showed that the regimen had a higher ORR (79%) and a longer median PFS (18.1 months). Moreover, phase III trials, including PHENIX and PHOEBE, confirmed that pyrotinib plus capecitabine could achieve longer median PFS (11.1 months, 12.5 months). Based on the above conclusions, this regimen has won regional recognition in China. 61
Tucatinib
Tucatinib is a new oral TKI, and in an in vitro model with HER2-overexpressed cells, tucatinib blocked the phosphorylation of HER2 and protein kinase B (PKB). 62 A phase Ib trial showed that the combination of tucatinib and TDM-1 had expectant outcomes in HER2+MBC. 63 Tucatinib is a promising drug because it does not bind to EGFR, which reflects lower toxicity and indicates the possibility of traversing the BBB. HER2CLIMB is a phase III trial that assessed the clinical efficacy of tucatinib plus trastuzumab and capecitabine in patients with HER2+MBC. The results showed that this regimen increased PFS compared to the placebo group (25% vs 0%, HR = .48; P < .01). Hence, the FDA recently authorized this regimen for adjuvant therapy in patients with advanced HER2+MBC. 64 Other phase III trials, such as HER2CLIMB02 and HER2CLIMB04, have attempted to further assess the availability of tucatinib in MBC. 65
Afatinib
Afatinib is a TKI that irreversibly inhibits HER1, HER2, and HER4 receptors. 66 A phase II trial (NCT01325428) assessed the possibility of applying afatinib in patients with inflammation or MBC. 67 A phase III trial, LUX-Breast 1, attempted to add afatinib to the regimen for patients treated with chemotherapy plus trastuzumab. 68 However, the result showed lower OS than the placebo group, and common AEs such as diarrhea and rash were inevitable. Consequently, the potency of afatinib needs to be investigated in further research.
Anti-HER2 Combined Therapies
PI3K/AKT/mTOR Inhibitors
In a previous statement, we learned that the PI3K/AKT/mTOR signaling pathway plays a vital role in HER2+BC. 69 By activating this pathway, cell proliferation, survival, and angiogenesis can be promoted, suggesting that we can attempt to delay the progression of HER2+BC by inhibiting this pathway. 5
Everolimus is a type of mTOR inhibitor. Several trials have confirmed that the application of everolimus is beneficial in patients with HER2+BC. 70 BOLERO-3 is a phase III trial, scientists have found that the combination regimen of everolimus plus trastuzumab and vinorelbine improved the median PFS compared to the placebo group (7.0 months vs 5.78 months). 71
Buparlisib, an oral inhibitor of both PI3K and mTOR, has been hailed as an exciting discovery in the field. NeoPHOEBE, a phase II trial, proved that the regimen of buparlisib plus trastuzumab and paclitaxel resulted in a higher RR (69% vs 33%, P = .053) and apparent decline of Ki67 (75% vs 27%) compared to the placebo group. 72
PD-1/PD-L1 Inhibitors
Programmed death-1(PD-1) and programmed death-ligand 1 (PD-L1) combine to trigger immune escape and are crucial to tumor growth. 73 As a result, PD-1/PD-L1 inhibitors have attracted considerable attention, and existing trials have shown that PD-1/PD-L1 inhibitors are helpful in the treatment of triple-negative breast cancer. Although there are few studies on HER2+BC, molecular mechanisms and in vitro trials have indicated that PD-1/PD-L1 inhibitors have modest clinical efficacy in HER2+BC. 74
Pembrolizumab is a commonly used PD-1 inhibitor, which can reverse trastuzumab resistance by restoring T cells to tumor cells. A phase Ib and II trial, PANACEA, indicated that pembrolizumab plus trastuzumab is safe and effective, with lasting clinical efficacy. 75
Another inhibitor, atezolizumab (ATEZO), can combine with PD-L1 to block the interaction between PD-L1 and B7.1. In a phase II trial, KATE2, the regimen of ATEZO plus T-DM1 acquired longer PFS than the placebo group (8.2 months vs 6.8 months, HR = .82; 95% CI, .55-1.23; P = .33). 76 Phase III trials are ongoing to determine the advantages of ATEZO. HER2-targeted agents have fast action and high safety, while PD-1/PD-L1 inhibitors have slow action and lasting efficacy, and their combination is expected to play a better role in further research.
HER2-Targeted Vaccines
Tumor vaccines have been explored in recent years, and HER2-targeted vaccines are considered a potential treatment for HER2+BC. 77 Based on the characterized peptide, virus, and tumor cells, HER2-targeted vaccines can be designed in various forms which aim at different substance. Prior clinical trials have shown that HER2-targeted vaccines can generate active immunity. 78 Future research should focus on the development of multi-epitope vaccines.
NeuVax, a peptide-based vaccine, has been widely investigated. Stimulation of CD8+ T cells by NeuVax promotes cytolysis and destroys tumor cells. NeuVax is the only HER2-targeted vaccine that has completed a phase III clinical trial (the PRESENT trial); however, the results indicate that the application of NeuVax might result in a high risk of recurrence. 79
AVX901 is a virus-based vaccine, which can jointly express tumor antigen and virus genes, activating helper T cells in vivo to trigger specific cellular and humoral immune responses. Patients will not become sources of infection because of the low toxicity of AVX901. A completed phase I trial (NCT01526473) has certified its feasibility. 80
ETBX-021 is a virus-based vaccine, which contains a modified adenovirus 5 that is inserted into the HER2 gene. A phase I trial (NCT02751528) has evaluated its safety and preclinical indices.
Chimeric Antigen Receptor (CAR) T-Cell Therapy
Chimeric antigen receptor (CAR) T-cell therapy is a novel approach for treating tumors. The mechanism involves editing tumor-specific T cells, which may be more efficient in killing tumor cells. It has been proven beneficial for several solid tumors, including ovarian carcinoma and prostate cancer.81,82 Scientists have attempted to explore whether therapy is helpful for HER2+ tumors. The phase I/II trial CAR-T-HER2 (NCT01935843) investigated the efficacy, feasibility, and activity of CAR T-cell therapy for HER2+ advanced solid tumors. Eleven patients were enrolled, among whom one obtained PR and five achieved stable disease without severe AEs. 83 The safety and persistence of T-cells, as well as the possibility of the application of CAR T-cell therapy in HER2+BC, need to be further verified.
Conclusions and Future Perspectives
Breast cancer is a major disease burden on women worldwide. Breast cancer can be classified into four subtypes based on IHC parameters, with HER2+BC occupying 15%–20% of all cases. The overexpression of HER2 can drive tumor growth and activate downstream signaling pathways, and, as a result, is extremely aggressive and has poor prognosis in terms of recurrence and metastasis. HER2-targeted therapy is a powerful strategy for the treatment of HER2+BC. The emergence of trastuzumab has improved this dilemma; however, some obstinate drug resistance and AEs associated with trastuzumab have hindered its use. Treatment options for patients with HER2+BC have changed dramatically due to the encouraging results of numerous clinical trials. Pertuzumab has shown good benefit, and patients who were considered likely to experience recurrence could benefit from the combination of trastuzumab and pertuzumab. Trastuzumab plus pertuzumab and taxanes remain the first-line regimen for HER2+BC. Other antibodies, such as ZW25, margetuximab, MM-111, MCLA-128, and ertumaxomab, have shown greater specificity in combination with the HER2 receptor or could bind to extra epitopes to enhance activity and generate greater immunologic responses. T-DM1 is an ADC authorized by the FDA as a second-line agent after failure of a standard chemotherapy regimen. The success of TDM-1 has led scientists to concentrate on the production of new HER2-targeted ADCs such as DS-8201, PF-06804103, PT-DM1, and HER2-vc0101. These ADCs differ in affiliative antibodies, linker drugs, or payloads. It is well accepted that ADCs are taking the central stage as second-or third-line regimens for HER2+BC. Adding small-molecule TKIs to the standard chemotherapy regimen, a third-line regimen, significantly improved the prognosis of patients.
DESTINY-Breast03 was the first trial to compare two ADCs in malignancy to change the standard regimen. The linker is specifically split by tumor cells, which triggers the release of membrane-permeable drug molecules. This “bystander effect” is considered to be advantageous given the heterogeneity of HER2 expression in HER2+ tumors. 47 In addition to the remarkable outcome, the safety of DS-8201 is acceptable and the AEs are within controllable ranges, which can be well managed by monitoring. With rapid development, the future of HER2+BC treatment will likely focus heavily on ADCs.
Although the abovementioned agents are of great value, some patients may be insensitive to them or develop resistance. Therefore, it is necessary to develop novel targeted agents. Preclinical and clinical trials of PI3K/AKT/mTOR inhibitors, PD-1/PD-L1 inhibitors, HER2-targeted vaccines, and CAR T-cell therapy have provided possible anti-HER2 combined strategies. However, the AEs and higher treatment costs need to be weighed by both clinicians and patients. To improve the quality of life and maximally reduce drug toxicity, one of the greatest challenges in the future is to discuss the best combined sequence of these agents. The progress of HER2-targeted therapy is challenging, but with deeper research, the regimens for HER2+BC will gradually become more individualized and precise.
Footnotes
Abbreviations
ADCs, antibody-drug conjugates; ADCC, antibody-dependent cell-mediated cytotoxicity; AEs, adverse events; ATEZO, atezolizumab; ATP, adenosine triphosphate; BBB, blood–brain barrier; CAR, chimeric antigen receptors; CD3, Cluster of Differentiation 3; CD8, Cluster of Differentiation 8; CI, confidence interval; CNS, central nervous system; CR, complete response; DS-8201, trastuzumab deruxtecan; EGFR, epidermal growth factor receptor; FDA, food and drug administration; HER1, human epidermal growth factor receptor 1; HER2, human epidermal growth factor receptor 2; HER2+BC, human epidermal growth factor receptor 2–positive breast cancer; HER3, human epidermal growth factor receptor 3; HER4, human epidermal growth factor receptor 4; HR, hazard ratio; HRG, heregulin; iDFS, invasive disease-free survival; IHC, immunohistochemical; MAGH22, margetuximab; MBC, metastatic breast cancer; NCCN, National Comprehensive Cancer Network; ORR, objective response rate; OS, overall survival; pCR, pathologic complete response; PD-1, programmed death-1; PD-L1, programmed death-ligand 1; PFS, progression-free survival; PKB, protein kinase B; PR, partial response; TDM-1, ado-trastuzumab emtansine; TKIs, tyrosine kinase inhibitors
Authors’ contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (81872152, Xiaoming Xie).