
Abstract
Introduction
Young-onset colorectal cancer (YOCR) is increasing. This study aimed to determine the difference between advanced YOCR and non-YOCR patient outcomes.
Methods
We retrospectively included patients with recurrent/metastatic colorectal cancer treated with palliative systemic therapy between 2016 and 2018. Diagnosis at < 50 years was defined as YOCR. Targeted sequencing was used to assess the mutational status.
Results
Among the 969 patients included, 210 (21.7%) were YOCR. The median progression-free survival with first-line chemotherapy (PFS1) was 9.7 vs 9.4 months (P = .755), and the median overall survival (OS) was 25.9 vs 22.3 months (P = .581) in the YOCR and the non-YOCR group, respectively. However, the youngest patients diagnosed at < 30 years showed poorer survival outcomes (median PFS1, 3.9 months; median OS, 8.6 months) compared with other age groups. PFS1 did not differ between YOCR and non-YOCR by choice of treatment regimen. Among the 340 patients with targeted sequencing results, YOCR had fewer APC mutations (61% vs 80%), but had similar KRAS (53% vs 48%), NRAS (7% vs 3%), and BRAF class I mutations (4% vs 6%). The median tumor mutational burden (TMB) was 10.9 vs 12.5 mut/Mb in YOCR and non-YOCR patients, respectively (P = .064). TMB increased with age in tumors with high microsatellite instability (Pearson’s R = .69, P = .028), but not in microsatellite-stable tumors (R = .02, P = .658).
Conclusions
Survival outcomes with palliative systemic therapy were similar between recurrent/metastatic YOCR and non-YOCR with an age cut-off of 50 years. However, patients diagnosed at < 30 years of age showed poorer outcomes compared with other age groups.
Keywords
Introduction
Although the median age of diagnosis of colorectal cancer is approximately in the mid-sixties and more than 88% of new colorectal cases in the USA are > 50 years old at the time of diagnosis, 1 recent trends in the incidence of colorectal cancer are noticeably different between age groups. Between 2011 and 2016, colorectal cancer incidence decreased by 3.3%/year in patients aged ≥ 65 years, whereas it increased by 2.2%/year in patients aged < 50 years, and the increase in the incidence was more prominent in patients aged < 40 years.2,3 These alarming trends in the increase of young-onset colorectal cancer (YOCR) are observed across continents, including East Asia, Europe, and Australia,4,5 and expected to continue to rise in the next 2 decades. 6
However, the difference in the clinicogenomic features and outcomes of YOCR and non-YOCR patients is yet to be determined. Previous studies suggested some features that may differentiate YOCR from non-YOCR, including advanced stage at presentation, left-sidedness, or poor differentiation.7,8 The reasons for these differences are not fully understood. As for the survival outcomes for YOCR, previous studies used heterogeneous age definitions for YOCR, often included heterogeneous patients with different disease stages, and produced contradictory results on the survival outcomes.9-11 Moreover, the effectiveness of specific chemotherapy regimens for YOCR patients was rarely described. Considering that YOCR patients constitute only 13%–15% of colorectal cancer clinical trial participants,12,13 the results of many clinical trials in colorectal cancer might not sufficiently reflect the outcome of YOCR patients. Therefore, further research is needed to determine if age-tailored treatment strategies are necessary in advanced-stage YOCR patients.
This study aimed to identify distinct clinical and genomic features of the YOCR patients and to analyze the impact of age and treatment regimen on the outcomes of YOCR patients, specifically patients with recurrent/metastatic disease treated with palliative systemic therapy.
Methods
Patients
Patients with recurrent or metastatic colorectal cancer patients who were treated with palliative systemic therapy between January 2016 and December 2018 in the Asan Medical Center, a tertiary referral center in Seoul, Republic of Korea, were retrospectively identified and included in this study. All individual patient data were de-identified. This study was approved by the Institutional Review Board (IRB) of the Asan Medical Center and conducted in accordance with the principles of the Declaration of Helsinki. The IRB waived the requirement for informed consent for this retrospective study.
Assessments, Bioinformatics Analysis, and Statistical Analysis
In this study, colorectal cancer diagnosed at < 50 years of age was defined as YOCR and the others were defined as non-YOCR. Progression-free survival (PFS) was defined as the time from the start of palliative systemic therapy to the time of disease progression or death of any cause, whichever occurred first. PFS1 and PFS2 indicate PFS with the palliative first-line and second-line treatment, respectively. Overall survival (OS) was defined as the time from the start of first-line palliative chemotherapy to the time of death of any cause. For targeted exome sequencing, an in-house panel of the Asan Medical Center (OncoPanel AMC, versions 3 and 414,15) was used from previously collected, formalin-fixed, paraffin-embedded tissue specimens.
Baseline characteristics were analyzed and compared using descriptive methods. Survival outcomes were estimated using the Kaplan–Meier method and compared using a log-rank test. The association between age at diagnosis and survival outcomes was assessed using the Cox proportional hazards model and restricted cubic splines curves with age treated as a continuous variable. The correlation between the age of diagnosis and the tumor mutational burden (TMB) was assessed using the Pearson’s R correlation coefficient. All tests were two-sided, and P values < .05 were considered statistically significant. Statistical analyses were performed using R version 4.0.1 (R Foundation for Statistical Computing, Vienna, Austria). The reporting of this study conforms to STROBE guidelines. 16
Results
Patients
Baseline Characteristics.
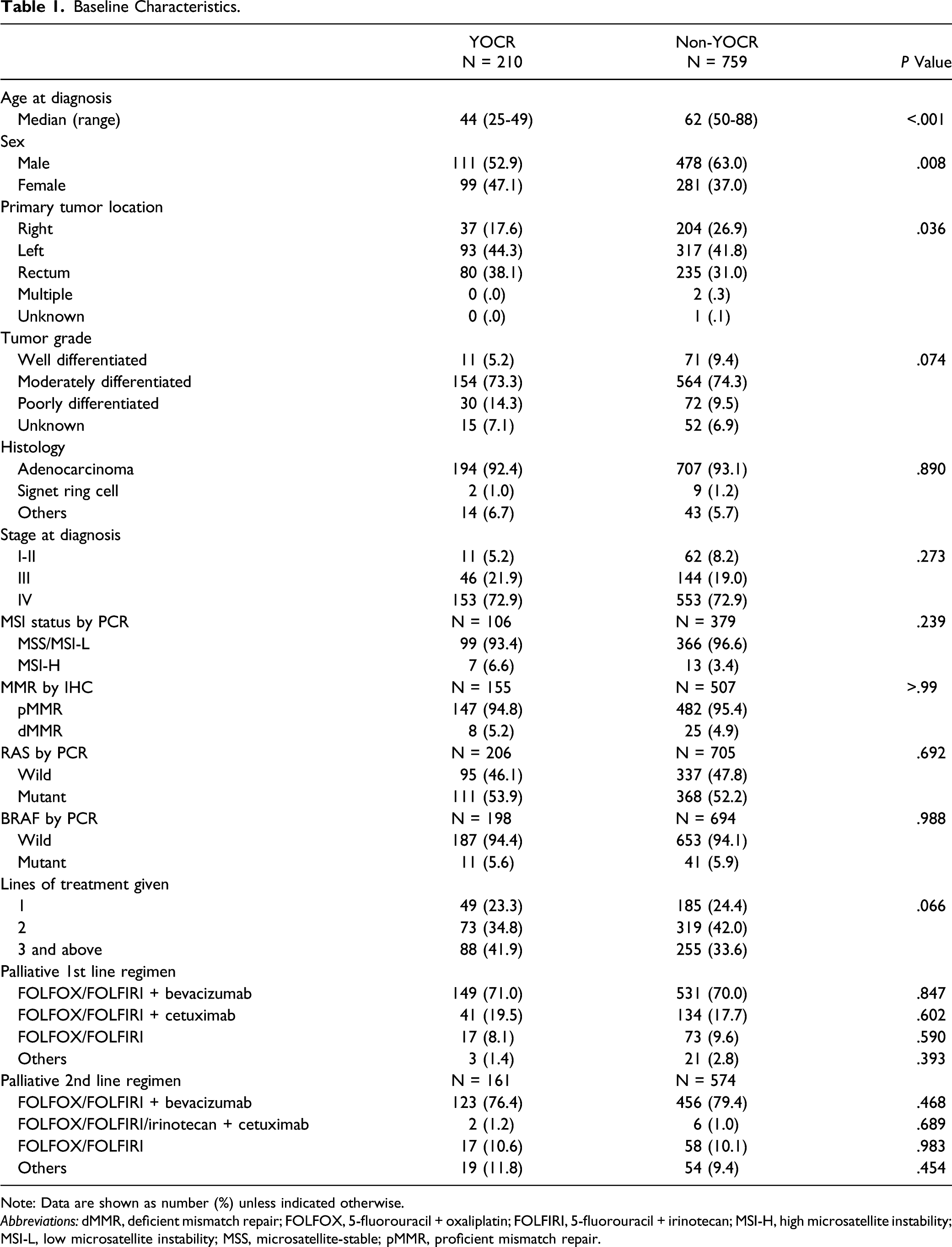
Note: Data are shown as number (%) unless indicated otherwise.
Abbreviations: dMMR, deficient mismatch repair; FOLFOX, 5-fluorouracil + oxaliplatin; FOLFIRI, 5-fluorouracil + irinotecan; MSI-H, high microsatellite instability; MSI-L, low microsatellite instability; MSS, microsatellite-stable; pMMR, proficient mismatch repair.
Treatment patterns were similar between groups. All patients received chemotherapy with palliative intent, with 190 patients (90.4%) in the YOCR group and 665 patients (87.6%) in the non-YOCR group treated with FOLFOX (5-fluorouracil/oxaliplatin) or FOLFIRI (5-fluorouracil/irinotecan) regimen with targeted agents as first-line treatment. As for targeted agents in the first-line treatment, bevacizumab was administered to 151 patients (71.9%) in the YOCR group and 534 patients (70.4%) in the non-YOCR group. Cetuximab was administered to 41 (19.5%) patients in the YOCR group and 136 patients (17.9%) in the non-YOCR group.
The number of patients who achieved complete surgical resection after initially-palliative-intent chemotherapy was 4 (1.9%) in the YOCR group and 9 (1.2%) in the non-YOCR group.
Survival Outcomes
The median follow-up duration was 41.9 months (95% confidence interval [CI], 39.1-44.6). During follow-up, median lines of chemotherapy given were 2 (range: 1-6) in the YOCR group and 2 (range: 1-7) in the non-YOCR group. Median PFS with first-line chemotherapy (PFS1) was 9.7 months (95% CI, 8.7-10.9) in the YOCR group vs 9.4 months (95% CI, 8.9-9.9) in the non-YOCR group (P = .755) (Figure 1A). Median PFS with second-line chemotherapy (PFS2) was 5.9 months (95% CI, 5.3-7.0) in the YOCR group vs 5.9 months (95% CI, 5.4-6.3) in the non-YOCR group (P = .844) (Figure 1B). Median OS was 25.9 months (95% CI, 24.1-28.3) in the YOCR group vs 22.3 months (95% CI, 20.9-23.8) in the non-YOCR group (P = .581) (Figure 1C). Progression-free survival with first-line chemotherapy and OS also did not differ between YOCR and non-YOCR patients in all subgroups stratified by RAS or BRAF mutation status (Supplementary Figure S1). Survival outcomes in the entire study population. (A) Progression-free survival (PFS) with first-line treatment, (B) PFS with second-line treatment, and (C) overall survival. Abbreviations: CI, confidence interval; YOCR, young-onset colorectal cancer.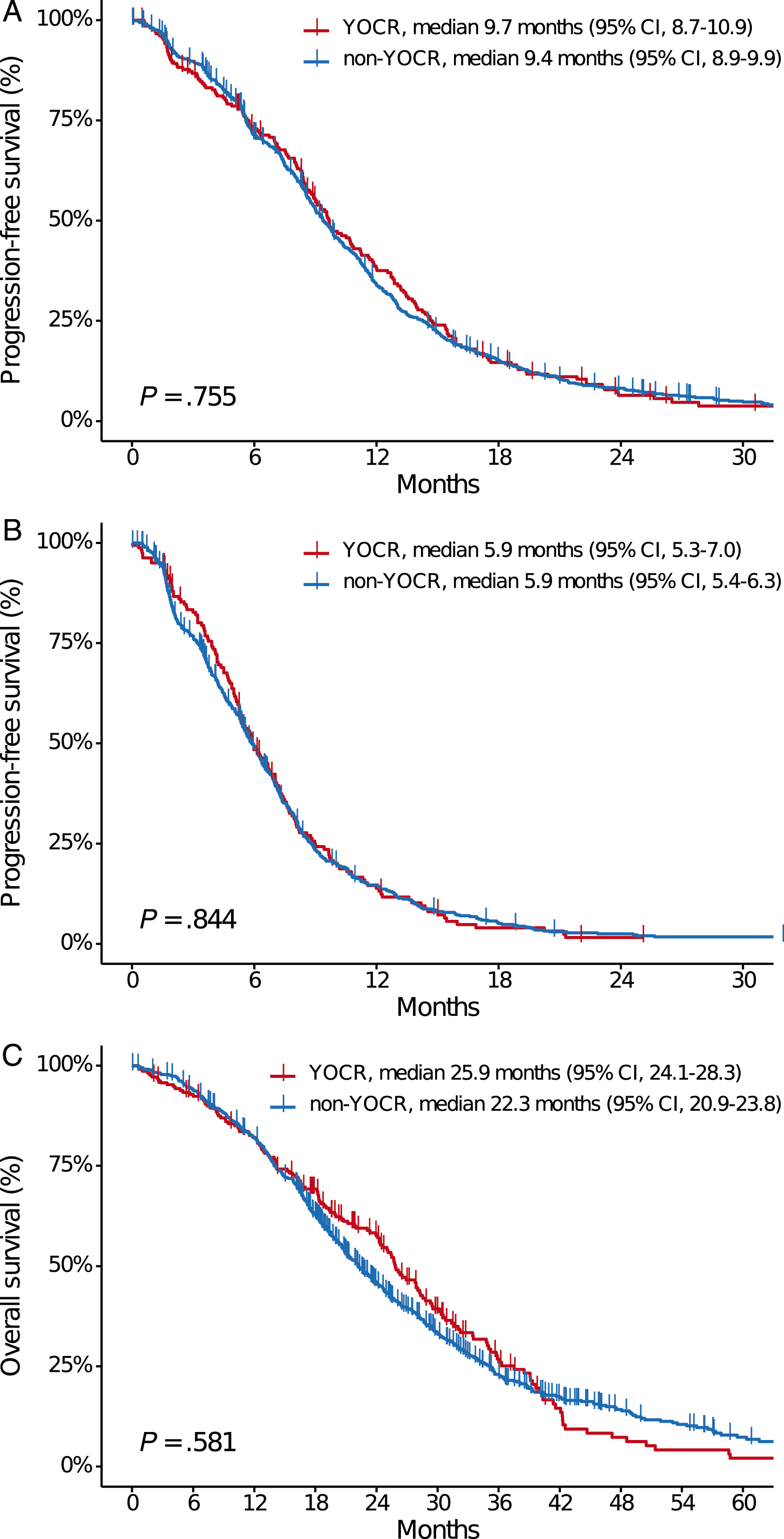
Survival Outcomes by Treatment
We compared PFS1 of YOCR and non-YOCR groups according to the first-line treatment regimen and MSI status. In left-sided tumors including rectal cancers, the median PFS1 with bevacizumab-chemotherapy combinations was 10.5 months (95% CI, 9.3-12.0) in the YOCR group (N = 119) vs 9.5 months (95% CI, 8.8-10.0) in the non-YOCR group (N = 375) (P = .131). In cetuximab-chemotherapy combination-treated left-sided tumors, the median PFS1 was 13.4 months (95% CI, 8.4-15.4) in the YOCR group (N = 37) vs 12.0 months (95% CI, 10.8-13.0) (N = 117) in the non-YOCR group (P = .714) (Figure 2A). In right-sided tumors, the median PFS1 with bevacizumab-chemotherapy combinations was 8.4 months (95% CI, 5.8-9.6) in the YOCR group (N = 32) vs 8.8 months (95% CI, 8.0-9.8) in the non-YOCR group (N = 156) (P = .368). The median PFS1 with cetuximab-chemotherapy combinations was 4.6 months (95% CI, 1.6–not estimated [NE]) in the YOCR group (N = 4) vs 10.7 months (95% CI, 7.3-13.2) in the non-YOCR group (N = 19) (P = .069) (Figure 2B). Progression-free survival with first-line treatment by regimen. (A) With bevacizumab- or cetuximab-containing regimens in left sided tumor and (B) in right sided tumor, (C) with irinotecan- or oxaliplatin-based regimens, and (D) by microsatellite instability status. AbbreviationsBev, bevacizumab; Cet, cetuximab; CI, confidence interval; YOCR, young-onset colorectal cancer, Irino, irinotecan; MSS, microsatellite-stable; MSI-H, high microsatellite instability; Oxali, oxaliplatin. Note: P values refer to log-rank tests and unadjusted for pairwise comparisons.
Progression-free survival with first-line chemotherapy did not significantly differ between the YOCR and non-YOCR groups in patients treated with first-line oxaliplatin- or irinotecan-based regimens (in oxaliplatin-treated patients, median 8.8 months [95% CI, 7.6-9.7] in the YOCR group [N = 92] vs 8.9 months [95% CI, 8.3-9.6] in the non-YOCR group [N = 369], P = .954; in irinotecan-treated patients, median 10.8 months [95% CI, 9.6-12.6] in the YOCR group [N = 118] vs 10.5 months [95% CI, 9.4-11.3] in the non-YOCR group [N = 372], P = .933) (Figure 2C).
Among patients with microsatellite-stable (MSS) disease confirmed by polymerase chain reaction-based analysis, the median PFS1 was 9.6 months (95% CI, 8.7-11.6) in the YOCR group (N = 99) vs 10.2 months (95% CI, 9.0-11.1) in the non-YOCR group (N = 366) (P = .586). Patients with MSI-H tumors had a median PFS1 of 3.8 months (95% CI, 1.7–NE) in the YOCR group (N = 7) and 5.9 months (95% CI, 2.2-8.5) in the non-YOCR group (N = 13) (P = .702).
Survival Outcomes by Detailed Age Group
Additionally, we analyzed survival outcomes according to more detailed age groups where patients diagnosed at age < 50 years were divided by age deciles (< 30 years [N = 10, 1.0%], 30-39 years [N = 48, 5.0%], 40-49 [N = 152, 15.7%], and ≥ 50 years [N = 759, 78.3%]). Patients who were diagnosed at < 30 years of age showed a shorter PFS1 and OS (median PFS, 3.9 months [95% CI, .6-8.1]; median OS, 8.6 months [95% CI, .6-16.1]) compared with other age groups (Figure 3A–B). Kaplan-Meier estimate of (A) progression-free survival with first-line treatment (PFS1) and (B) overall survival (OS) in detailed groups by age at diagnosis, and unadjusted hazard ratio for (C) PFS1 and (D) OS by age at diagnosis as a continuous variable. AbbreviationsCI, confidence interval.
In a univariable Cox regression analysis for PFS1 and OS according to age as a continuous variable, age showed a borderline statistical significance for nonlinear association (P = .093 for PFS1, P = .096 for OS), with hazard ratios increasing at the extremes of age (Figure 3C–D).
Genomic Analysis by Targeted Sequencing
Summarization of Targeted Gene Sequencing Results.

Abbreviation: YOCR, young-onset colorectal cancer.
Tumor Mutational Burden
Tumor mutational burden was calculated from targeted gene sequencing results
14
in the aforementioned 340 patients. Among those, 10 patients (2.9%) were MSI-H, and 330 patients (97.1%) were MSS by targeted sequencing. In MSS tumors, the median TMB was 10.9 mut/Mb [range, 4.7-28.1] vs 12.5 mut/Mb [range, 1.6-167.2] in YOCR (N = 72) and non-YOCR (N = 258) patients, respectively (P = .064). In MSI-H tumors, the median TMB was 78.1 mut/Mb [range, 29.7-106.3] and 137.5 mut/Mb [range, 87.5-178.1 in YOCR (N = 5) and non-YOCR (N = 5) patients, respectively (P = .032) (Figure 4A–B). In the MSS group, TMB was not correlated with age at diagnosis (R = .02 by Pearson’s correlation, P = .658), whereas in the MSI-H group, TMB increased as the age at diagnosis increased (R = .69, P = .028) (Figure 4C). Tumor mutational burden in patients with (A) microsatellite-stable tumors, (B) high microsatellite instability, and (C) Pearson correlation between age and tumor mutational burden. AbbreviationsYOCR, young-onset colorectal cancer; MSI, microsatellite instability.
Discussion
Currently, the need for age-tailored therapy in patients with advanced colorectal cancer has not been clearly established. Based on a large clinical and genomic dataset on the recurrent/metastatic diseases treated with palliative systemic therapy, this study showed that the survival outcomes of YOCR patients were not inferior to those of non-YOCR patients. However, the youngest subgroup of YOCR patients diagnosed at < 30 years of age demonstrated shorter survival outcomes compared with other age groups. The YOCR group showed several distinct features, including fewer APC mutations and Wnt pathway alterations in terms of genomic alterations by targeted sequencing, Also, in patients with MSI-H tumors, TMB increased with age, whereas in MSS patients, it did not.
The treatment regimens used in this study cohort were mostly 5-fluorouracil-based doublet with irinotecan or oxaliplatin combined with targeted agents (> 87% of the patients), and only 1 patient in the non-YOCR group received triplet chemotherapy containing both irinotecan and oxaliplatin. Overall, all the survival outcomes measured including PFS1, PFS2, and OS did not differ between the YOCR and non-YOCR patients. Moreover, we looked into the survival outcomes by treatment regimens and observed no significant differences in PFS1 by the choice of chemotherapy agents or targeted agents in both age groups. Although it has been reported that YOCR patients tend to receive more aggressive treatment including triplet chemotherapy, 17 evidence is lacking on the survival benefit of such approach. Our findings suggest that survival outcomes of YOCR did not differ from those of non-YOCR who underwent similar systemic treatment.
One of the important issues in YOCR is what cutoff value for age should be used for the definition of YOCR. Currently, different definitions of YOCR are used among studies, most commonly around screening ages (40-50 years). 18 We performed additional survival analyses by age deciles among the YOCR patients to determine if prognoses differ in certain age groups before the screening age. As a result, patients diagnosed at < 30 years of age showed significantly poorer survival outcomes compared with other age groups. The poor prognoses of these “very young-onset” colorectal cancers have been suggested in prior studies.8,19-21 In the univariable Cox proportional hazards model with age treated as a continuous variable, patients of extreme ages showed tendencies toward increased hazard ratios for PFS1 and OS with marginal significance for nonlinear associations, consistent with a previous report. 13 Given that our dataset included only a limited number of patients diagnosed at < 30 years of age, further studies are required to confirm the poor prognoses of very YOCR patients and establish the adequate age cutoff for “young-onset” colorectal cancers.
We observed that YOCR patients had significantly fewer APC mutations than non-YOCR patients, which is in line with the results of previous studies.7,22,23 The lower incidence of the Wnt pathway mutation in the YOCR group is also consistent with the low incidence of the APC mutation. However, despite the repeatedly described poor prognosis in APC wild-type colorectal cancer,24,25 the difference in the frequency of APC mutation between age groups did not result in different survival outcomes in this study. Overall, both groups showed high frequency of TP53 mutation (> 84%) which possibly attributed to the advanced disease status of our cohort.26,27
Some previous studies reported a higher incidence of MSI-H tumors in YOCR patients. 7 In this study, the proportion of MSI-H tumors was numerically higher in the YOCR group (6.6% vs 3.4% among patients with available results) without statistical significance. Regarding TMB, it did not differ between age groups in MSS tumors (10.9 mut/Mb in the YOCR group vs 12.5 mut/Mb in the non-YOCR group) without significant linear correlations by age. In contrast, the median TMB patients with MSI-H tumors were lower in the YOCR group (78.1 mut/Mb vs 137.5 mut/Mb). Also, the MSI-H group showed higher TMB with increasing age. In the recent Keynote-177 study, first-line pembrolizumab showed improved PFS in MSI-H/dMMR advanced colorectal cancer. 28 Whether TMB could serve as a predictive marker for treatment response and survival outcomes of MSI-H patients treated with immune checkpoint inhibitors is currently unknown; however, retrospective studies have suggested the relationship between improved response rates and survival outcomes to immune checkpoint inhibitors and high TMB values.29,30 Taken together with our findings that showed a correlation between age and TMB in MSI-H patients, it is worthy of further investigation if clinical outcomes differ by age in patients treated with immune checkpoint inhibitors for advanced colorectal cancer.
One of the limitations of this study is its single-centered and retrospective nature, and the relatively smaller number of patients in the YOCR group compared with the non-YOCR group, which might attribute the lack of statistical significance in the differences of clinical features between groups. However, the strength of our study lies in the homogeneity of patient population in terms of disease status and treatment as well as the large sample size including targeted sequencing results retrieved from real-world practice. Moreover, our data included detailed information on treatment, which we used for survival outcome analysis by regimens and patient characteristics with long-term follow-up duration. The authors believe that this study provides useful information on the palliative treatment choice of YOCR in daily practice where data on the survival outcomes by specific treatment regimens is limited.
Conclusion
Survival outcomes did not differ between recurrent/metastatic YOCR and non-YOCR patients treated with palliative systemic therapy with an age cut-off of 50 years. However, the outcome of patients aged < 30 years was poorer, with the limitation of a small patient number, and warrants further investigation.
Supplemental Material
Supplemental Material - Clinicogenomic Characteristics and Treatment of Young-Onset Colorectal Cancer Patients Treated With Palliative Therapy in Real-World Practice
Supplemetary Material for Clinicogenomic Characteristics and Treatment of Young-Onset Colorectal Cancer Patients Treated With Palliative Therapy in Real-World Practice by Hyehyun Jeong, Eunjung Lee, Deokhoon Kim, Jihun Kim, Sun Young Kim, Yong Sang Hong, Tae Won Kim1, and Jeong Eun Kim in Cancer Control
Supplemental Material
Supplemental Material - Clinicogenomic Characteristics and Treatment of Young-Onset Colorectal Cancer Patients Treated With Palliative Therapy in Real-World Practice
Supplemetary Material for Clinicogenomic Characteristics and Treatment of Young-Onset Colorectal Cancer Patients Treated With Palliative Therapy in Real-World Practice by Hyehyun Jeong, Eunjung Lee, Deokhoon Kim, Jihun Kim, Sun Young Kim, Yong Sang Hong, Tae Won Kim1, and Jeong Eun Kim in Cancer Control
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (2020IP0040) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea, and by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HI18C2383).
Ethics Statement
This study was approved by the Institutional Review Board (IRB) of the Asan Medical Center and conducted in accordance with the principles of the Declaration of Helsinki. The IRB waived the requirement for informed consent for this retrospective study (#2021-0425, approved on 22-Mar-2021).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.