
Abstract
Background
The correlations of epidemiological characteristics and clinical outcomes with different tumor sites in patients with intracranial typical site germinomas (ICTSGs) have not yet been well established. We analyzed ICTSGs using a multicenter database, focusing on its demographic, management patterns, and long-term survival outcomes.
Methods
Patients diagnosed with ICTSGs were selected from the Surveillance, Epidemiology, and End-Results (SEER) database. Demographic information and management patterns of ICTSGs were extracted for data analysis stratified by different tumor sites. Kaplan–Meier curves were used to evaluate the survival outcome stratified by treatment, tumor site and tumor size.
Results
Among the 327 patients enrolled in the study, 16.21% had tumors located in the suprasellar region and 83.79% in the pineal region. The proportion of males was significantly higher among pineal germinomas (94.16 vs 66.04%; P < .001). Smaller tumors (<24 mm) were more common in the suprasellar region (37.74 vs 18.87%; P < .001). A higher percentage of patients with suprasellar germinomas underwent surgery. Radiotherapy (RT) and chemotherapy (CT) was, respectively, administered to 82.97 and 60.61% of patients during the treatment period, with no significant difference between suprasellar and pineal germinomas. CT plus RT was the most common treatment modality for both pituitary (30.19%) and pineal (33.94%) germinomas. Both RT and CT were associated with improved long-term survival. No survival difference was observed between suprasellar and pineal germinomas.
Conclusions
Despite significant differences in epidemiology and management, pineal and suprasellar germinomas had a similar long-term clinical outcome.
Introduction
Intracranial germinomas are rare primary central nervous system (CNS) tumors in western countries that account for 65–75% of all intracranial germ cell tumors (iGCTs).1,2 Germinomas predominantly occurs in male pediatric and young adult patients. The most common region affected by this neoplasm are the midline structures, such as the pineal gland and suprasellar region, which is why they are collectively referred to as intracranial typical site germinomas (ICTSGs). 3 However, the correlations of epidemiological characteristics and clinical outcomes with different tumor locations have not yet been investigated in detail for ICTSGs.
Medical presentations and tumor markers are used to diagnose germ cell tumors in North America and Europe. 3 However, since the majority of intracranial germinomas are non-secretory, the serum tumor marker levels (b-hCG and AFP) may be within the normal range in the early stage. 4 Motor disorders (dyskinesia/ataxia and focal/general weakness), Parinaud syndrome (eye coordination disturbances and pupil dysfunction), neurological manifestations (headache, nausea/vomiting, dizziness/vertigo, and drowsiness), polyuria/polydipsia, and urine/stool incontinence have all been identified as possible symptoms in studies of ICTSGs. 5 However, no characteristic clinical manifestations were observed, and early detection is difficult.
Germinomas are highly sensitive to radiotherapy (RT) and chemotherapy (CT).6,7 However, it is worth noting that all confirmed cases of recurrence were located outside of the irradiated field in patients who received local radiation therapy, while there were no cases of observed recurrence following RT covering the ventricles. 8 Both in terms of reducing the recurrence rate and prolonging survival, craniospinal radiation, whole-ventricle irradiation, or whole-brain RT gradually replaced local radiation therapy and have become the gold standard for treating germinomas.8-11 It became necessary to decrease the radiation dose due to the sequelae of CNS irradiation, such as cognitive impairment and hormonal dysfunction. 12 As a result, platinum-based CT has been adopted by an increasing number of medical centers. Compared to radiation alone, a combination regimen of RT and CT has also been found to provide better clinical outcomes. 13 Nevertheless, there are a variety of treatment methods for integrating RT and CT, and the optimal regimen is still being researched.
ICTSGs outlive germinomas in atypical locales in terms of progression-free survival. 3 However, the differences in epidemiological data and clinical outcomes between ICTSGs affecting different sites are mostly unknown and have previously only been described in a few studies of limited patient populations. Furthermore, previous research has not been able to properly clarify whether there are gaps in the WHO definition of ICTSGs or heterogeneity in outcomes across various treatment centers. In order to improve the clinical management of ICTSGs, we analyzed 327 cases selected from the Surveillance Epidemiology and End-Results (SEER) database, to be further integrated with the epidemiological characteristics and long-term clinical outcomes.
Materials and Methods
Ethics Approval Statement
All patient data in the NCI SEER is anonymized, and the study received a waiver for consent from the ethics committee due to its retrospective nature and guaranteed patient privacy.
A Study Designed to Select Patients
We performed a retrospective analysis of the SEER program governed by the USA National Cancer Institute (NCI, USA). The SEER database collects and publishes data on cancer incidence, treatment, and survival from 18 cancer registries in 13 states (Alaska, California, Connecticut, Georgia, Hawaii, Iowa, Kentucky, Louisiana, Michigan, New Jersey, New Mexico, Vermont, and Washington) that covers around 30% of the US population and could readily represent the population diversity. 14 A SEER Research Data Agreement was essential to obtain the user account, enabling free access to the SEER data. Individual-level data were extracted from the SEER database using NCI SEER*Stat 8.3.9 software published on March 15, 2021. Patients diagnosed after December 31, 2010, were eliminated in order to guarantee sufficient follow-up time. In 1998, the SEER database was updated to include detailed information on surgery for individuals diagnosed with systemic malignancies and patients diagnosed before 1/1/1998 were not included in the study. Thus, the cohort in the current study consisted of patients diagnosed with a germinoma in the suprasellar region or the pineal gland from 1998 to 2010 using the International Classification of Diseases for Oncology, Third Edition (ICD-O-3), histology codes 9064/3 (germinoma), and the ICD-O-3 site codes C75.1 (pituitary) and C75.3 (pineal). Patients had to be excluded due to incomplete dates for survival. Participant follow-up ended December 31, 2016.
Patient Demographics and Treatment History
Patients were further stratified according to the tumor site, yielding a suprasellar and a pineal region group. Demographic variables such as age, race/ethnicity, sex, region of diagnosis, tumor size, survival time (months), and vital status were collected. Age was used as a continuous variable and expressed as the mean ± standard deviation (SD). Treatment information containing surgery, RT, and CT was accessible in the SEER database. The surgical strategies were described in detail and categorized into 5 classifications: gross total resection (GTR), subtotal resection (STR), biopsy, no surgery, and others. Treatment comparison categories included the abovementioned surgical approaches plus RT and CT or not. Descriptive analysis was performed to compare the demographic and treatment characteristics of the suprasellar and pineal groups. We excluded patients who had incomplete information on surgery from the analysis of management. Overall survival was used as the primary endpoint in survival analysis. We performed Kaplan–Meier (K-M) survival analysis (or Kaplan–Meier product-limit estimates) to plot the survival curves.
Statistical Analysis and Analytic Methods
Chi-squared and Fisher’s exact test were used to estimate the differences in demographics and therapies between the suprasellar and pineal groups. We applied the Log-rank test to assess the statistical significance in the survival curves produced by the K-M methodology. 15 Two-tailed P values of less than .05 were considered to indicate statistical significance for comparisons.
Results
Demographic Characteristics of the Enrolled Patients
Demographics of patients with intracranial typical site germinomas.

Follow‐up time (months)* expressed as median (interquartile range, IQR). N-H, non-Hispanic.
Management patterns* of patients with intracranial typical site germinomas.

Available data for management patterns* n =323; RT, Radiotherapy; CT, Chemotherapy; GTR, gross total resection; STR, subtotal resection.

Workflow for the analysis of demographics and management patterns of patients with intracranial typical site germinomas.
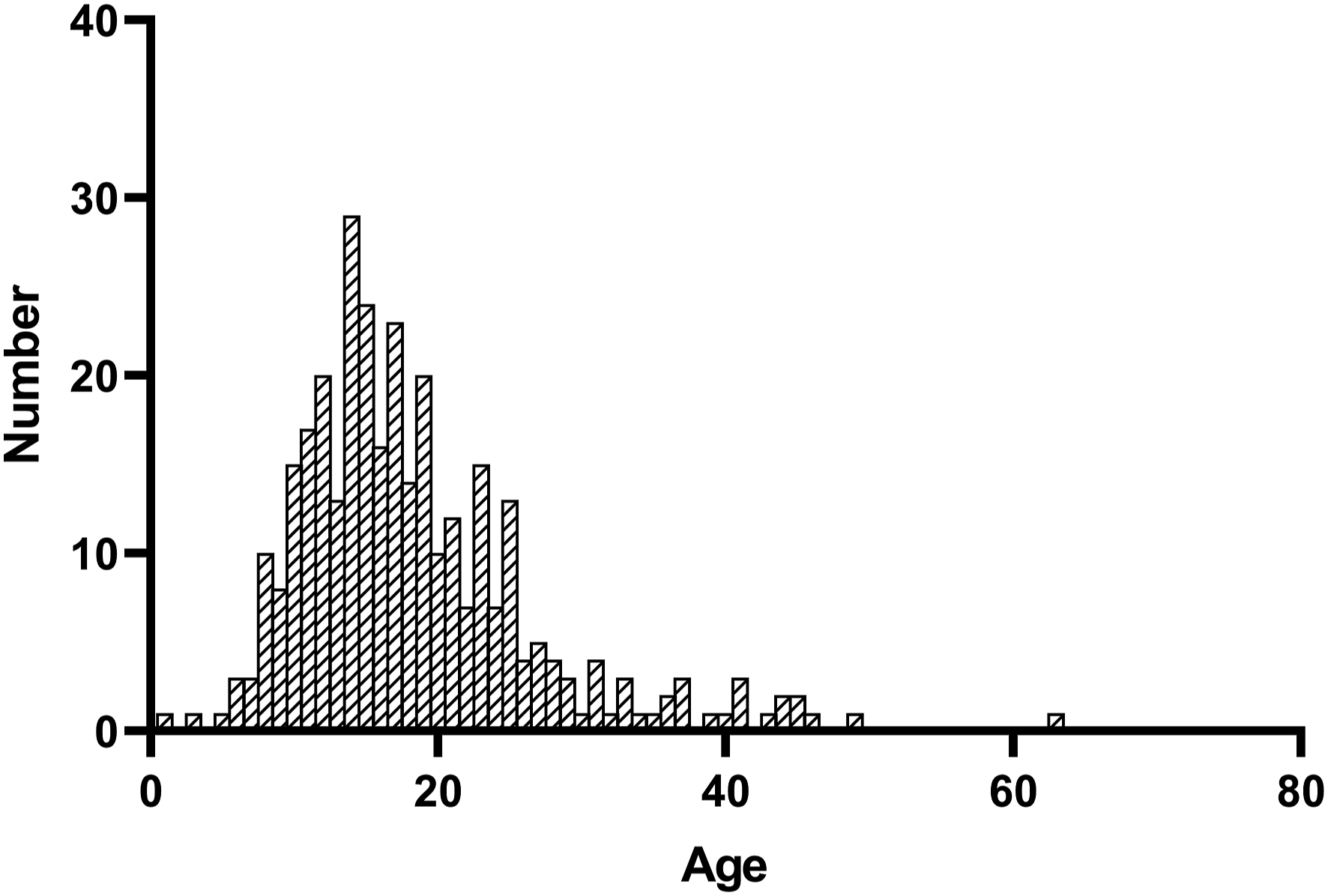
The number of patients with intracranial typical site germinomas.
In terms of race/ethnicity, most patients were non-Hispanic White (53.52%) followed by Hispanic (21.41%), others (containing non-Hispanic Asian or Pacific Islander and non-Hispanic American Indian/Alaska Native, 18.96%), and non-Hispanic Black (6.12%). The United States (US) is divided into 4 geographical census regions in the database, and the Western part accounted for the majority of the patients (69.73%), followed by the Southern region (13.76%), Northeast region (10.09%), and Midwest region (6.42%).
Overall, there were no statistically significant differences between the suprasellar and pineal groups in age, race, geographic location and follow-up time. However, significant differences were found in the gender distribution (P < .001) and tumor size (P < .001) between the suprasellar and the pineal germinomas.
Patient Treatment Characteristics
The treatment data were available for 323 patients. A total of 268 (82.97%) patients received RT as part of therapy, with no statistically significant difference (P = .898) between the suprasellar and pineal groups (82.35 vs 83.10%). CT was performed for 60.61% of all patients as part of therapeutic modality with not statistically significant (P = .151) usage difference in the suprasellar region (70.59%) when compared to the pineal region germinomas (59.92%). 117 (36.22%) patients underwent surgery as part of the treatment. There was a significantly higher rate of surgical treatment (including GTR, STR, and biopsy) in the suprasellar region than in the pineal region (P = .001). Treatment regimens for suprasellar germinomas most commonly included RT + CT (30.19%), RT + STR + CT (15.09%), and RT+GTR+CT (9.43%). For pineal germinomas, most patients underwent RT + CT (33.94%), followed by RT (19.71%) and RT + biopsy + CT (8.76%). We observed 54 (19.71%) and 22 (8.03%) pineal ICTCGs who received RT only and CT only, respectively. This was accompanied by 3 (5.66%) and 2 (3.77%) suprasellar ICTCGs treated with RT only and CT only, respectively.
Overall Survival
Kaplan–Meier curves were plotted to compare the long-term survival among groups stratified by primary tumor site, tumor size, and treatments (Figure 3). There was no difference in survival between suprasellar and pineal germinomas (P = .760). The association of tumor size and overall survival in our cohort did not reach statistical significance. Furthermore, we found that RT (P = .0048) and CT (P = .0053) were significantly associated with increased overall survival. And the effect of radiation treatment, chemotherapy, and tumor location on the outcomes of patients who had surgery with verified tumor pathology was similar to the whole cohort (Supplemental Figure S1). Kaplan–Meier curves showing a significantly improved long-term survival in patients receiving radiotherapy (A) or chemotherapy (B); surgical treatment (C) and tumor site (D) were not associated with patient survival; smaller tumor size (<24 mm) was related to better long-term survival, but the difference did not reach statistical significance (E).
Discussion
The current study aimed to address the scarcity of data on the demographics and management of ICTSGs. At present, there are few extensive cohort studies that offer reliable insights for diagnosing and treating ICTSGs due to the low incidence of the disease. Midline tumors, also known as germinomas, a primary histological subtype of iGCTs, most frequently arise in the pineal and suprasellar regions, but the differences in their respective epidemiologically are not well described.
Our analysis demonstrates that the average onset age of suprasellar germinomas was similar to that of pineal germinomas (17.98 vs 18.39; P = .750). This suggests that the tumor location does not influence the age of onset. However, it is well known that the pathogenesis of germinomas depends on a patient’s age.3,16,17 We observed 1 peak of occurrence of onset at the age of 14–15, and a similar trend was reported by Takami, 18 who compared the difference of epidemiology, tumor location, histology, and prognosis of iGCTs between Mayo Clinic (n = 98) and Japanese consortium cohorts (n = 154) and observed a single peak during adolescence in both places. The “germ cell theory” which states that the faulty location of primordial germ cells occurs with a similar pattern intracranially and extracranially. 19 On the way to the normal destination, primordial germ cells may abnormally migrate during the 3rd–4th week of gestation and inappropriately stay in midline structures, such as the mediastinum sacrococcygeal region and the third ventricle.20,21 The high incidence of adolescent cases of germinomas in this study needs more in-depth research in the future.
Suprasellar germinomas have a male predominance, with no apparent differences in pediatric and adult groups. 22 Similarly, a male predominance was noted in neurohypophyseal and pineal germ cell tumors. The sex distribution was more markedly skewed among patients with tumors in the pineal region, greater than 90% of which were male, compared with approximately 75% of patients in the neurohypophyseal region. 8 However, the sample size (n = 60) of the study was small, which might influence the reliability of the results. Fortunately, the data of our study, which is based on NCI SEER with a larger sample size, consolidate these findings. Based on the “germ cell theory,” we hypothesized that progenitor germ cells appeared with equal frequency at pineal and suprasellar region in both sexes, and affected by physiological/hormonal changes in adolescence, tumorigenesis preferentially occurs in males in the pineal region. Alternatively, the pineal gland may have a unique developmental attraction for the abnormal aggregation of progenitor germ cells in males. Both these scenarios provide plausible explanations for our other finding that a higher proportion of large-sized tumors (>24 mm) occurred in the pineal region while smaller ones were mostly found in the suprasellar region. Although the high ratio of missing values of tumor size in the suprasellar region may affect the reliability of the results, the overall proportion of missing values was acceptable for complete case analysis.
Our findings indicated that the vast majority of the study cohort (82.57%) underwent RT not only in suprasellar germinomas but also in pineal germinomas, and more than half of the patients (60.86%) received CT in both suprasellar and pineal germinomas (67.93 and 59.50%, respectively). Similar RT administration ratios were observed in recent studies on iGCTs (germinomas and non-germinomatous tumors) as a whole 23 or germinomas only in the suprasellar region. 22 Interestingly, Bhimani et al found that pediatric patients were significantly more prone to receive radiation therapy during treatment than adult patients (79.2 vs 41.0%). Therapies like these could be tailored to pediatric patients to minimize the long-term adverse effects of radiation on cognitive and endocrine dysfunction.12,24 However, we found that the overall administration ratio of CT (63%) reported by Bhimani et al was similar to the 1 found in our study (60.86%). These differences in treatment patterns might be related to patient age rather than primary tumor location. Local radiation therapy is a poor treatment for localized germinoma, and the Pediatric and Children’s Oncology Group of the European Society recommends whole-ventricle irradiation in combination with platinum-based CT.11,25 This explains our finding that RT plus CT was the most commonly performed therapeutic methods in the entire cohort (33.33%), suprasellar cohort (30.19%), and pineal cohort (33.94%).
Moreover, patients with suprasellar germinomas were significantly more likely to receive surgery (including GTR, STR, and biopsy) than those with pineal germinomas (56.86 vs 32.35%). In fact, suprasellar germinomas can be challenging to diagnose, which is most likely to result in delayed diagnosis or misdiagnosis. It was reported that 82% of patients with suprasellar iGCTs experienced a delay in diagnosis ≥6 months. 26 A median time of about 16.8 months was needed to confirm the diagnosis of a pituitary tumor. 27 As a result, a histopathological diagnosis based on a surgical specimen is required. Therapies for iGCTs in Japan are usually based on postoperative histopathology diagnosis that divides patients into 3 risk groups.28,29 In the United States, on the other hand, it is more customary to establish a diagnosis based on clinical symptoms and tumor markers rather than a histology finding. 30 This means that if a germinoma is verified by initial laboratory findings, clinical manifestations, and MR imaging, the patients will receive the standard treatment (RT with or without CT). In present research, 1 unanticipated finding was that surgery was not associated with improved long-term survival results (P = .94). If a preoperative diagnosis for pituitary and pineal tumors is problematic, surgery is essential for a clear diagnosis, and the degree of surgery should also be addressed. 31
The survival analysis suggested that both RT and CT improved the prognosis in the whole study cohort. This is unsurprising, since the survival benefits of receiving RT and CT have been described in many previous studies.3,8,18,22 Bhimani et al even explained why there was insufficient data to clarify the relationship between CT and survival in germ cell tumor patients in past decades. 32 Still, the authors were able to conclude that suprasellar germinomas would benefit from CT. The effect of patient age or concurrent therapies may lead to these outcomes.
Our study did not reveal a significant survival difference between suprasellar and pineal germinomas. This can be explained by the fact that both the pineal region and suprasellar region are located in midline structures, which are typical sites for germinomas, and share similar therapeutic regimens. Earlier studies found differences in the prognosis of germinomas arising from different intracranial sites, with patients suffering from germinomas in typical sites having a relatively more prolonged progression-free survival in comparison with atypical sites (including basal ganglia and the cerebral cortex, P = .03). 32 A biological difference between germinomas at typical or atypical sites has not been discovered. However, this is not the main focus of this article. Moreover, our study suggested that larger tumors may be associated with poorer survival, but the difference was not statistically significant for this cohort. To our best knowledge, there are no reports on the relationship between the tumor size of iGCTs and the prognosis that could serve as a reference. According to the results of K-M curve analysis, we only may speculate that early-stage patients with larger tumor size may have a poorer prognosis.
Some prior relevant studies with adequate sample size have studied intracranial germinoma diagnosis and outcomes to some extent.22,33-35 Our investigation had strengths. First, none of these studies have focused on epidemiology, management, and long-term survival outcomes of intracranial typical site germinomas that are a special category of intracranial germinoma. 3 Therefore, it is necessary to launch a new study to exploit it. Second, we found pronounced epidemiological differences between pineal germinomas and suprasellar germinomas, which could facilitate early detection of pineal germinomas. Third, there was significant variation in the choice of treatment modalities for pineal germinomas and suprasellar germinomas, which do not lead to different clinical outcomes regarding overall survival. This is an interesting finding and deserves further exploration.
Limitations
Our work should be considered in the context of the inherent limitations of the SEER database when critically evaluating the abovementioned findings. The SEER database used in the study containing 18 cancer registries is potentially affected by some particular clinical centers, leading to further validation with patient data. Moreover, data collection and reporting to SEER by different contributors from different clinical centers can present a significant challenge for researchers in terms of accurately capturing and evaluating a specific patient population. Most importantly, there is no information on specific RT and CT regimens in the current SEER database and only de-identified data is available. The chemotherapy regimens applied, including pharmaceutical combinations, dosages, and cycle counts, as well as the dose and radiation field used, were all unknown.36-38 Furthermore, the SEER program did not include data on intraoperative findings, postoperative complications, and molecular diagnoses, as well as changes in endocrine responsiveness and tumor markers before and after therapy. It is regrettable that the treatment data was not sufficient for logistic regression or Cox regression analysis.
Conclusions
In this retrospective study, we attempted to provide more information on the differences in epidemiology, management patterns, and survival outcomes between suprasellar and pineal germinomas. We demonstrated a higher proportion of male patients and larger tumors among the pineal germinoma cases. The administration ratios of RT and CT were similar for the 2 groups, but suprasellar germinoma patients were more likely to undergo surgery. RT and CT were both associated with improved long-term overall survival, while surgery was not. And the tumor site did not affect survival outcomes. Additional research is required to corroborate our findings.
Supplemental Material
Supplemental Material - Epidemiology, Management, and Long-Term Survival Outcomes of Intracranial Typical Site Germinomas: An Analysis of the Surveillance, Epidemiology, and End-Results (SEER) Database
Supplemental Material for Epidemiology, Management, and Long-Term Survival Outcomes of Intracranial Typical Site Germinomas: An Analysis of the Surveillance, Epidemiology, and End-Results (SEER) DatabaseWenqiang Che by Yujiao Wang, Yanmin Zhou, Xiangyu Wang, and Jun Lyu in Cancer Control
Footnotes
Authors’ contributions
Methodology, C.W.; software, C.W.; validation, W.Y, Z. Y, L.J. and W.X.; formal analysis, C.W.; resources, C.W, W.Y.; writing-original draft preparation, C.W.; writing-review and editing, L.J.; supervision, W.X, L.J.; project administration, L.J. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Material
Ethics approval
All patient data in NCI SEER is anonymized, and the study received a waiver for consent from the ethics committee due to its retrospective nature and guaranteed patient privacy.
Consent to participate
Not applicable as the SEER database was analyzed retrospectively.
Consent for publication
All of the authors consented to have their work published for free.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.