
Abstract
Background
The association between the type of anesthesia used and the recurrence of cancer remains controversial. This study aimed to compare the effects of local vs general anesthesia on recurrence-free survival and cost after breast-conserving surgery.
Materials and Methods
We reviewed the data of 2778 patients who underwent breast-conserving surgery followed by radiation at our center between 1999 and 2014. We analyzed the data of 994 patients with hormone receptor-positive and Her2-negative tumors who underwent breast-conserving surgery without axillary lymph node dissection under local or general anesthesia. Patients were grouped according to whether local or general anesthesia was used for the surgery.
Results
Of the 994 patients enrolled in this study, 367 received local anesthesia and 627 patients received general anesthesia. The median follow-up duration for all patients was 93 months. The Kaplan–Meier survival curves did not reveal significant differences between the recurrence-free survival of the two groups, with 5-year recurrence-free survival rates of 96.3% (95% CI, 94.3–98.3%) in the local anesthesia group and 97.3% (95% CI, 95.9–98.7%) in the general anesthesia group. The total cost of hospitalization in the local anesthesia group was significantly lower than that in the general anesthesia group (P <.001). The difference in the cost between the two groups remained significant, irrespective of the type of hospitalization, after excluding 165 patients receiving chemotherapy during their hospitalization.
Conclusions
Our analysis indicated no association between the type of anesthesia used during breast-conserving surgery and the long-term prognosis of breast cancer. However
Introduction
Breast cancer is the most common cancer affecting women worldwide. 1 Breast-conserving surgery, in conjunction with radiation therapy, has become a routine treatment, which yields survival rates equivalent to those of mastectomy in early-stage breast cancer.2-6 There has been some debate regarding the influence of anesthetic agents on the recurrence of breast cancer. 7 Previous clinical studies have compared the regional and general anesthetic approaches, and several studies have shown that local anesthetics significantly inhibit cancer cell survival in vitro.8,9 However, the effect of local anesthetics on tumor recurrence in patients is unclear, 10 while it is also noteworthy that local anesthetics constitute the less expensive option.11,12 Controlling costs is an important factor during the decision-making and treatment-planning process in the current health care milieu. These two aspects, that is, outcome and cost, are key factors that determine the course of action for treatment, necessitating a better understanding of these factors. In our clinical practice, local anesthesia is one of the options for breast-conserving surgery without axillary lymph node dissection. This retrospective study compared the outcomes and hospital costs between patients who underwent breast-conserving surgery under local and general anesthesia, respectively. We hypothesized that the recurrence-free survival and cost would differ between the local and general anesthesia groups.
Materials and Methods
The reporting of this study conforms to the STROBE guidelines. 13 The research protocol was examined and approved by the Ethics Committee.
Patient Characteristics
Data on 2778 women with primary invasive breast cancer who underwent breast-conserving surgery followed by radiation between December 1999 and December 2014 were obtained from a database created and managed by the Breast Cancer Center, Peking University Cancer Hospital. The inclusion criteria for this study were as follows: patients who underwent breast-conserving surgery without axillary lymph node dissection under either local or general anesthesia (axillary lymph node dissection was avoided in patients with negative sentinel lymph nodes, and those with positive sentinel lymph nodes after 2010 if they met the characteristics of the ACOSOG Z0011 trial 14 ); a negative margin; and hormone receptor-positive (estrogen receptor-positive and/or progesterone receptor-positive, >1% positive cells by immunohistochemistry staining) and Her2-negative tumors. This study included 994 patients. The need for specified informed consent was waived due to the retrospective nature of the study. All patient details have been de-identified.
Anesthesia
General anesthesia was induced with fentanyl and propofol, while tracheal intubation was facilitated by succinylcholine or a non-depolarizing muscle relaxant. Alternatively, a laryngeal mask was used. Anesthesia was maintained with sevoflurane or isoflurane in oxygen, balanced nitrogen, fentanyl, or propofol. Alternatively, total inhalation anesthesia or intravenous anesthesia was used for the maintenance of general anesthesia at the discretion of the anesthesiologist. Patients who underwent general anesthesia did not receive local anesthesia during breast-conserving surgery.
Local anesthesia was administered by surgeons in the operating room using 10 mL of 1% lidocaine with adrenaline 1:200 000 in 40 mL normal saline at a total volume of 50 mL. The initial skin infiltration was performed and the local anesthetic solution was infiltrated around the marked lump/lesion. The administration of local anesthesia was performed slowly, on either side, above, and below the lump. If necessary, another 50 mL of the solution was administered.
Surgical Procedures
Sentinel lymph node biopsy with a 99mTc-labeled rituximab tracer was performed before breast-conserving surgery. The tumors were localized preoperatively using ultrasonography or marked with skin tattoos prior to the administration of neoadjuvant treatment. During breast-conserving surgery, surgeons attempted to remove .5–1 cm of normal tissue with the primary tumor. Glandular reshaping was utilized to close the defect and improve the long-term cosmetic outcomes. If a positive margin was identified on the intraoperative frozen section, additional tissue was excised during the same surgery according to the patient’s surgical cavity to obtain a negative margin. The final margin status was determined by examining the permanent paraffin-embedded sections.
Follow-up
The duration of follow-up was calculated from the date of surgery. Patients were advised to undergo examination every 6 months after surgery for the first 5 years of follow-up, and annually thereafter. Ultrasonography was performed at each follow-up examination and mammography was performed on an annual basis.
The primary endpoints of this study were local relapse, recurrence-free survival and breast cancer-specific survival. The secondary endpoint was the cost of hospitalization. Recurrence-free survival was defined as the interval between the date of surgery and the date of breast cancer recurrence or death. The recurrence-free survival events included any recurrence of breast cancer or death, including locoregional or systemic events, excluding contralateral breast cancer. Breast cancer-specific survival was defined as the interval between the date of surgery and the date of breast cancer-related death.
Statistical Analysis
Statistical power calculation was not performed before the study. The patient characteristics were compared between the subtypes using the chi-squared test. Survival probabilities were estimated using the Kaplan–Meier method. Cox proportional hazards regression was used to assess the independent associations of several variables with recurrence-free survival. The independent sample t-test was used to assess the cost of hospitalization. Odds ratios and their 95% confidence intervals (CIs) were estimated using a Cox model with a backward stepwise method. All reported P-values were two-sided with values <.05 considered as statistically significant. All statistical analyses were performed using SPSS 23.0 (IBM, Armonk, NY, USA).
Results
Among the 994 patients enrolled in our study, 367 (36.9%) received local anesthesia, and 627 (63.1%) patients underwent general anesthesia. A total of 981 (98.7%) received endocrine therapy.
Characteristics According to Anesthetic Approaches.
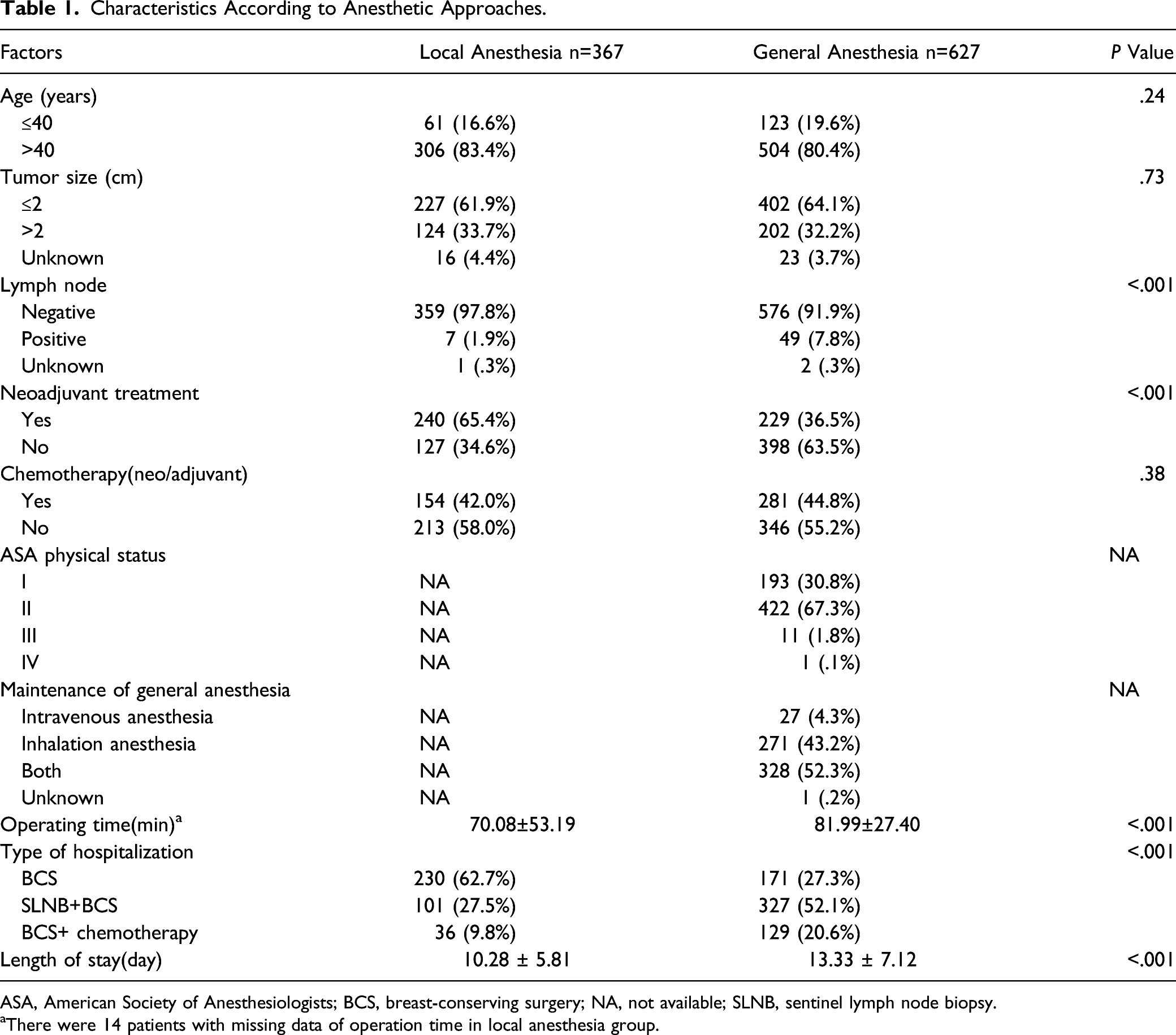
ASA, American Society of Anesthesiologists; BCS, breast-conserving surgery; NA, not available; SLNB, sentinel lymph node biopsy.
aThere were 14 patients with missing data of operation time in local anesthesia group.
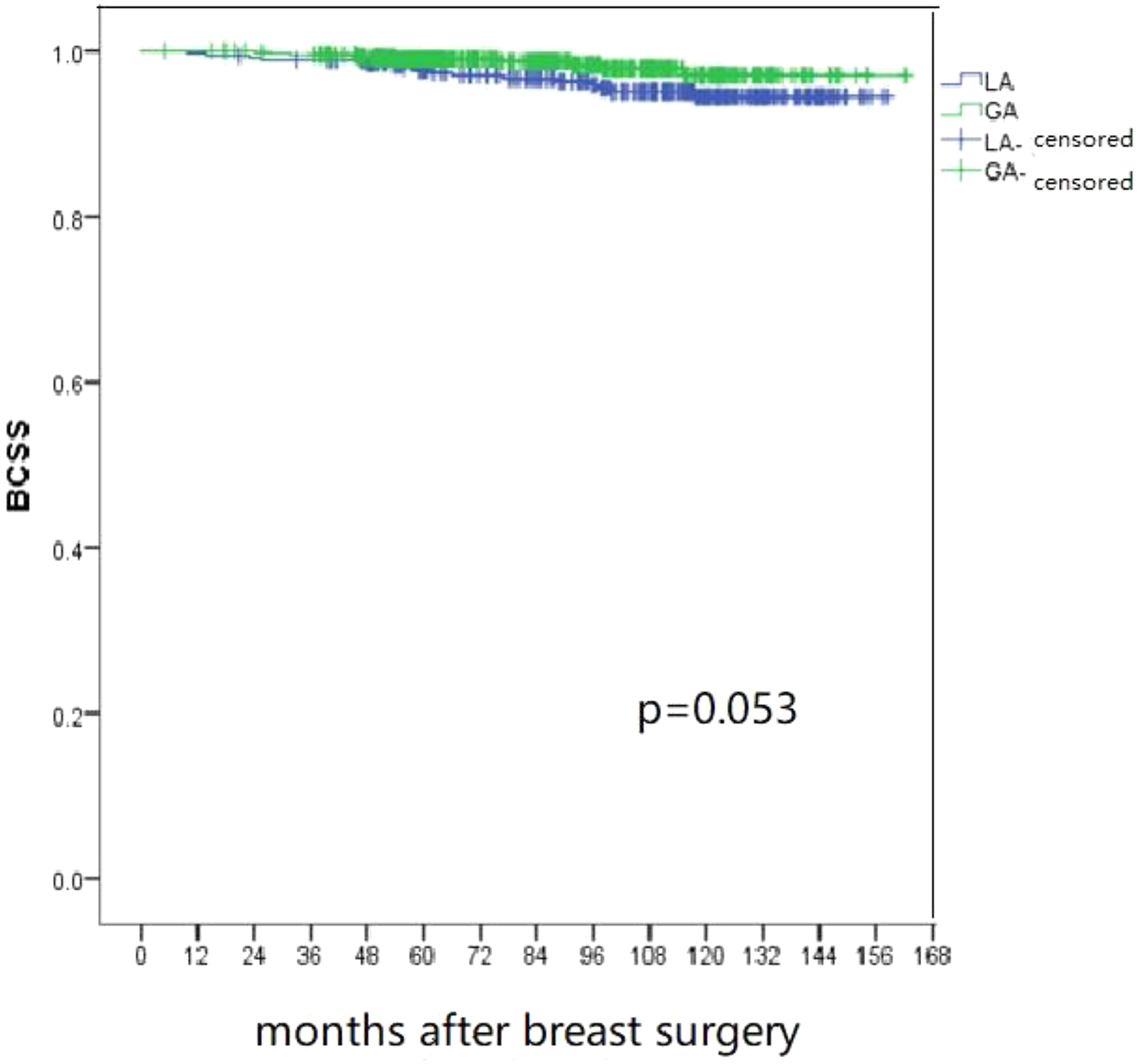
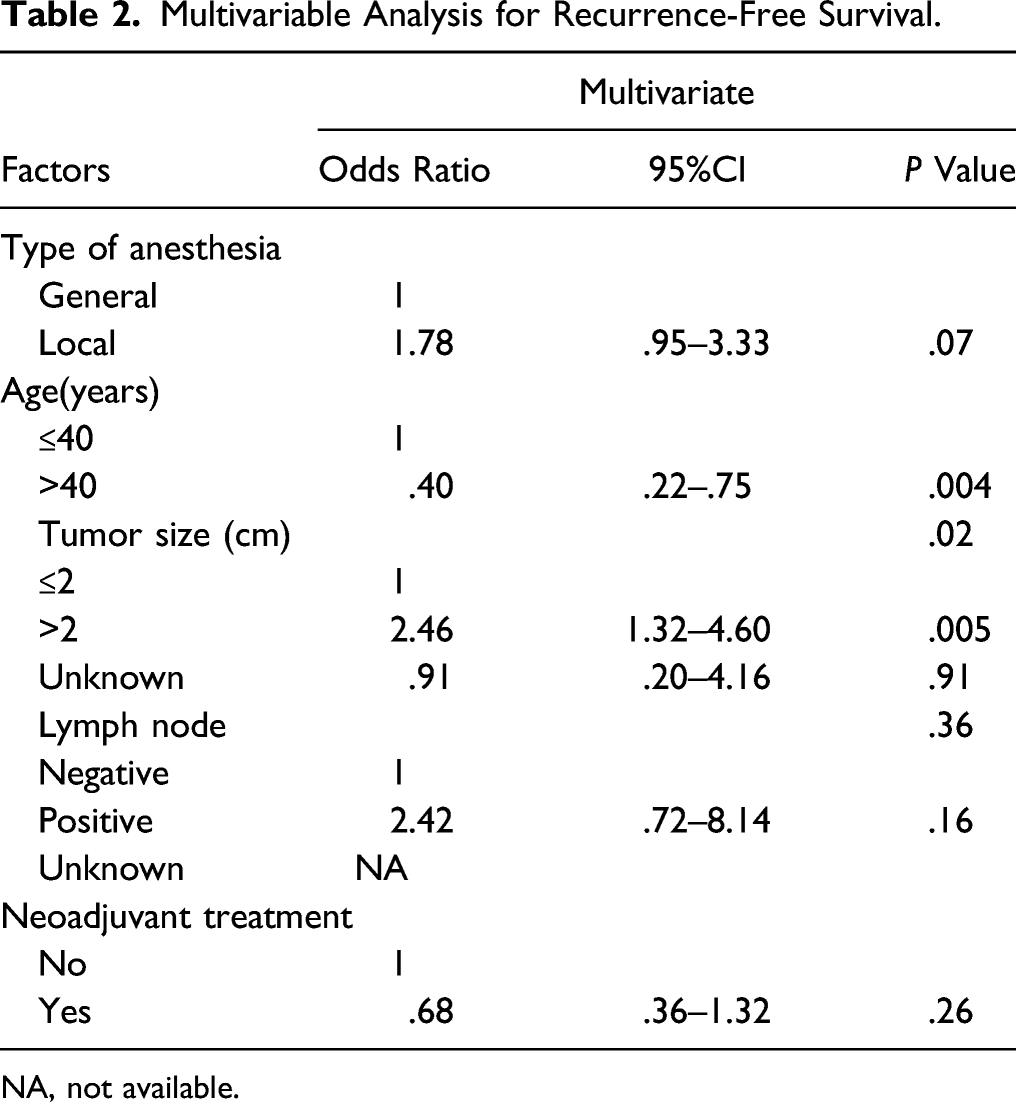
The median follow-up duration was 93 months (range, 5–162 months) for all patients. The 5-year local relapse rate was .7% and .3% in the general and local anesthesia groups, respectively. The Kaplan–Meier survival curves revealed 5-year recurrence-free survival rates of 97.3% (95% CI, 95.9–98.7%) in the general anesthesia group and 96.3% (95% CI, 94.3–98.3%) in the local anesthesia group, while the respective 5-year breast cancer-specific survival rates were 99.0% (95% CI, 98.6–99.4) and 97.7% (95% CI, 96.9–98.5). There was no significant difference in the local relapse (P =.48), recurrence-free survival (P =.21) and breast cancer-specific survival (P =.053) between the two groups (Figures 1-3). Multivariable Cox regression revealed no significant association between local anesthesia and poorer recurrence-free survival (odds ratio, 1.78; 95% CI, .95–3.33; P =.07; Table 2) compared to the general anesthesia group. The Cox proportional hazards model showed that age ≤40 years and tumor size ≥2 cm were associated with poor prognosis (Table 2). Cumulative local relapse rate in two groups. GA, general anesthesia; LA, local anesthesia. Kaplan–Meier survival curve for recurrence-free survival in two groups. GA, general anesthesia; LA, local anesthesia; RFS, recurrence-free survival. Kaplan–Meier survival curve for breast cancer-specific survival in two groups GA, general anesthesia; LA, local anesthesia; BCSS, breast cancer-specific survival. Multivariable Analysis for Recurrence-Free Survival. NA, not available.

Total Cost of Hospitalization.

Total cost of hospitalization after excluding 165 patients received chemotherapy during their hospitalization.

BCS, breast-conserving surgery; SLNB, sentinel lymph node biopsy.
Discussion
In this study, we found that local anesthesia or general anesthesia had no influence on local relapse or recurrence-free survival in patients who underwent breast-conserving surgery without axillary lymph node dissection. Furthermore, there was no significant association between the type of anesthesia used and prognosis after breast-conserving surgery.
Numerous comparative analyses of cancer recurrence have been conducted using data of patients who received general or general and regional anesthesia, including studies that specifically targeted patients with breast cancer. One retrospective study suggested that paravertebral anesthesia and analgesia for breast cancer surgery reduced the risk of recurrence or metastasis. 15 On the other hand, two randomized trials found no apparent protective effect of regional anesthesia.16,17 Another retrospective cohort study found no significant impact of total intravenous anesthesia or inhalation anesthesia on the recurrence of breast cancer. 18 Few studies have focused on local anesthesia vs general anesthesia in breast cancer. Theoretically, non-ventilated anesthesia with local anesthesia is less inflammatory and the local anesthetic acts directly on the breast cancer cells, which may reduce breast cancer recurrence. However, the present study showed that local anesthesia may not have a more positive effect on the prognosis after breast-conserving surgery compared to general anesthesia. Prospective randomized controlled trials that compare local anesthesia and general anesthesia in breast-conserving surgery are needed.
One ongoing phase III trial evaluating the effect of peritumoral injection of lidocaine in breast cancer (NCT01916317) may help ascertain the effects of local anesthesia alone on tumor recurrence.
This study found a strong association between age and the risk of cancer recurrence after breast-conserving surgery. Several other studies have also confirmed that the prognosis of young patients with breast cancer is significantly poorer than that of older patients.19,20 In our study, neoadjuvant treatment was more frequent in the local anesthesia group than that in the general anesthesia group. We did not find an association between neoadjuvant treatment and recurrence-free survival. However, tumors downsized by neoadjuvant treatment may facilitate breast-conserving surgery under local anesthesia.
Our results showed a higher reduction in the total cost of hospitalization for patients who underwent breast-conserving surgery without axillary lymph node dissection using the local anesthesia method compared to general anesthesia. Similarly, several studies reported that cutaneous surgery, such as vitrectomy and thyroidectomy, could be performed under local anesthesia with lower costs.11,12 The mean operating time was shorter in the local anesthesia group than in the general anesthesia group; hence, the utilization of the operating room was reduced. In our practice, local anesthesia was administered by surgeons, and breast-conserving surgery under local anesthesia required fewer health care experts, thereby lowering the cost compared to general anesthesia.
There were several limitations to our study. First, this study was retrospective in design, and power calculation was not conducted for the estimation of the required sample size. Studies with small sample populations are usually too underpowered to show any statistical significance. Second, only patients with hormone receptor-positive and Her2-negative tumors were included because the differences in systemic treatment for triple-negative or Her2-positive patients, such as therapy with or without platinum agents and trastuzumab, may have confounded the results. Third, the surgeons decided which patients would receive local or general anesthesia, which could have introduced a degree of selection bias.
Conclusions
We found no significant impact of local anesthesia or general anesthesia on the local relapse and recurrence of breast cancer in patients who underwent breast-conserving surgery. However, local anesthesia may cost less than general anesthesia, making it a viable option for breast-conserving surgery without axillary lymph node dissection in some circumstances.
Footnotes
Acknowledgments
The authors would like to acknowledge Lize Wang who managed the data base. We appreciate Yingjian He who worked on statistics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by capital’s funds for health improvement and research (code: 2018-2-2152).
Ethical approval
The research protocol was examined and approved by the Ethics Committee of Beijing Cancer Hospital.