
Abstract
Esophageal cancer (EC) is a highly aggressive cancer with poor outcomes under current treatment regimens. More recent findings suggest stroma elements, specifically cancer-associated fibroblasts (CAFs), play a role in disease occurrence and progression. Cancer-associated fibroblasts are largely the product of converted fibroblasts, but a variety of other local cell types including epithelial cells, endothelial cells, and mesenchymal cells have also been shown to transform to CAFs under the correct conditions. Cancer-associated fibroblasts primarily function in the communication between the tumor microenvironment and cancer cells via cytokine and chemokine secretions that accentuate immunosuppression and cancer growth. Cancer-associated fibroblasts also pose issues for EC treatment by contributing to resistance of current chemotherapeutics like cisplatin. Targeting this cell type directly proves difficult given the heterogeneity between CAFs subpopulations, but emerging research provides hope that treatment is on the horizon. This review aims to unravel some of the complexities surrounding CAFs’ impact on EC growth and therapy.
Introduction
Esophageal cancer (EC) is responsible for claiming more than half a million lives each year and is the eighth most prevalent cancer type worldwide. 1 EC also ranks sixth in respect to cancer mortality rates. 1 Late detection contributes to decreased survival rates in EC as only about 20% of cases remain locally confined at the time of initial diagnosis. 2 EC is subdivided into two major histological types, which include esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma (EAC). 2 ESCC persists as the prevailing subtype in large portions of Asia while EAC rates have spiked in various western countries including the United States.1,2 Both EC subtypes share some similarities in risk factors with poor diet and tobacco usage overlapping.2,3 On the other hand, many risk factors differ between the two cancers as relationships between ESCC disease instance and heavy alcohol consumption, pickled vegetables, and hot food have been documented. 4 Conversely, EAC rates correlate heavily with obesity, gastroesophageal reflux disease (GERD), and Barrett’s Esophagus (BE). 5
Although the incidence of EC continues to increase worldwide, the field still lacks treatment options addressing issues of recurrence and advanced disease stage. 6 Recent studies have pointed toward the tumor microenvironment (TME) as a culprit in therapeutic resistance to conventional treatment options. 7 The TME is composed of diverse cell types, including macrophages, endothelial cells, pericytes, adipocytes, dendric cells, natural killer (NK) cells, and cancer-associated fibroblasts (CAFs).8-10 Particularly, CAFs persist as a vital component in EC as their heterogeneity and lack of clear origin present issues when attempting to specifically target them. 7 Crosstalk between stromal cells and with cancer epithelial cells contributes to immune suppression and, in turn, creates optimal conditions for tumor progression and metastasis. 10 Growing interest has been placed on the role of CAFs in EC, from tumor growth to treatment resistance. 11
Origins of CAFs and Heterogeneity
While CAFs have garnered attention when targeting EC, the origins of CAFs remain unclear. Resident fibroblasts remain the most abundant source of CAFs, but studies have unearthed various other cell types capable of transforming into CAFs including adipocytes, pericytes, stellate, endothelial, and epithelial cells as well as mesenchymal stem cells.12-15 Additionally, the variation between CAF subtypes has posed challenges for researchers attempting to distinguish their markers, secretions, and implications in EC progression. 16 Recent studies continue to unearth the numerous queries surrounding the development and heterogeneity of this important EC stromal component.
One of the initial interests of investigators is to understand the conversion of normal fibroblasts to the cancer-associated phenotype. One such mechanism involved modification of fibroblasts via transforming growth factor β (TGF-β) induced upregulation of SMAD, which results in a shift toward CAF expression, revealed through alpha-smooth muscle actin (α-SMA) presentation. 16 Manipulation of the Notch signaling pathway by cancer cells has also been suggested as a possible mechanism in CAF generation. 17 While still not well understood in EC, the implication of the pathway on fibroblast activation varies between cancer types with some conversions appearing by cell-to-cell contact and others through loss of Notch signaling.16-18 Interestingly, CAFs also appear to utilize this pathway as means of promoting cancer progression. 18 Others have noted that certain processes, such as epithelial–mesenchymal transition (EMT) and endothelial–mesenchymal transition (EndoMT), as well as cytokines observed in EC, for example, interleukin-6 (IL-6), also assist in the conversion of some cell types into CAFs. 19 Some studies have even implicated chemoradiotherapy to increase CAF populations, although the impact is still unknown in EC. 20
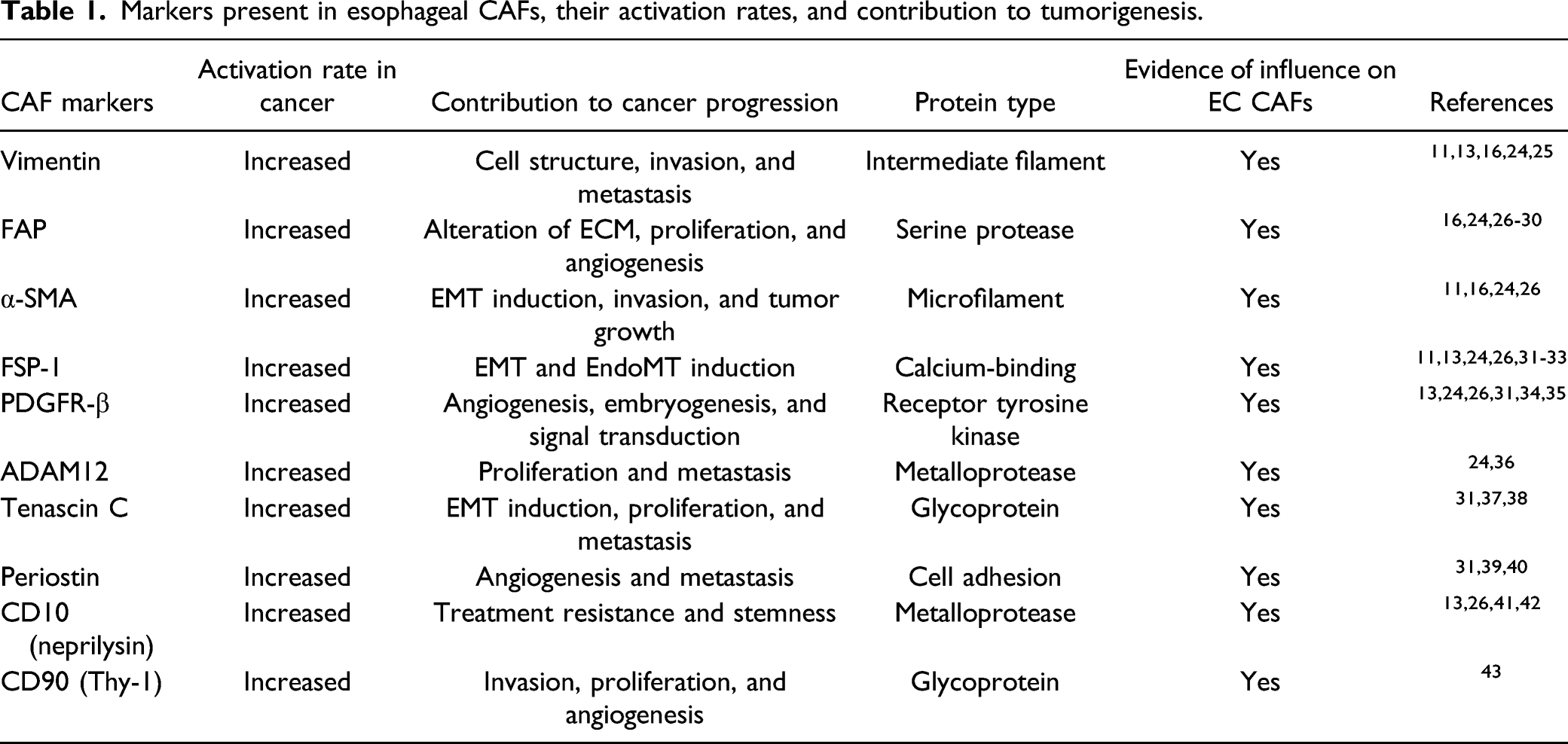
Markers present in esophageal CAFs, their activation rates, and contribution to tumorigenesis.
Cytokines, Chemokines, and Growth Factors Associated With CAFs in EC
The heterogeneity of CAFs also yields a TME diverse with assorted signaling proteins and interactions between stromal cells and cancer cells. 44 Cytokines exist in numerous subtypes, which can function in tumor-suppressing and tumor-promoting manners. 45 Cytokines are signaling proteins that vary in size from 5–20 kD 46 and have major implications on tumorigenesis as well as patient survival in EC and other cancer types.47,48 They allow for cell-to-cell communication via cancer cells and stromal cells and assists in inducing an immune-suppressed microenvironment necessary for EC development, progression, and metastasis.45,47 Chemokines are a subset of cytokines, which tend to measure between 8–10 kD 49 and are divided into four groups, CC, CXC, CX3C, and XC, based on the location of their cysteines with respect to their N-terminus.45,49,50 Like with other cancers, EC utilizes specific cytokines and chemokines in order to create a climate suitable for tumorigenesis. 7 While cancer cells assist in setting the stage for the microenvironment, CAFs maintain it and contribute to further carcinogenesis. 11
TGF-β
TGF-β is an anti-inflammatory cytokine involved in numerous cellular functions. 51 The cytokine exists in three different isoforms (TGF-β1, TGF-β2, and TGF-β3) that have various contributions to EC. 47 TGF-β was first identified with epidermal growth factor (EGF) as a factor that pushed fibroblasts into different phenotypes. 52 The cytokine plays a major role in general cell signaling with a strong impact on SMAD transcriptional regulation.51,53 The prevalence of SMAD signaling throughout cell types paired with the pleiotropic nature of TGF-β allows for manipulation of the pathway by EC cells.51,53 In fact, since its discovery in the 1980s, TGF-β has been strongly implicated in the initiation as well as the progression of many cancer types, including EC.52,54,55
TGF-β levels remain abundant throughout the EC TME. Under normal conditions, TGF-β displays tumor-suppressing properties, even inducing apoptosis in EC. 50 Upon subsequent alterations of the TGF-β pathway, cancer cells are able to highjack the machinery to inhibit the cytokine’s tumor-suppressing abilities. 51 Cancer cells are able to utilize TGF-β to activate pathways involved in weakening the immune response to EC and building an immune suppressive microenvironment. 53 One major method of immune suppression by cancer cells is to convert resident fibroblasts into a phenotype more conducive to cancer progression. 54 The creation of CAFs allows for direct feedback with the cancer cells as well as further conversion of other local fibroblasts. 54 Following fibroblast activation, TGF-β is secreted by CAFs to assist in EC cancer cell progression and further development.51,54
Secretions of TGF-β have been widely implicated in many physiological processes that support tumor initiation, progression, and metastasis. As previously mentioned, TGF-β allows cancer cells to signal to resident fibroblasts for conversion to a cancer-associated phenotype; however, TGF-β also has the ability to act on other stromal elements to induce cancer-favoring processes. 54 In EAC, clinical data has shown an association between TGF-β and tumor stage, with lower cytokine levels associated with favorable patient survival. 47 The TGF-β pathway has been observed to assist in the remodeling of EC extracellular matrix components via upregulation of matrix metalloproteinase 9 (MMP9), thus creating a habitat hospitable for tumor progression and metastasis.54,56 Furthermore, TGF-β is linked to EMT, which has been shown to transform epithelial cells to mesenchymal stem cells.57,58 The mesenchymal stem cells create an environment that is more evasive to the immune system, thus promoting invasion and metastasis in EC.53,57,58 In ESCC, TGF-β has also been shown to impact EMT via upregulation of MALAT1 and XlAP.59,60 Additionally, EMT has been linked to decreased patient survival rates and increased metastasis in EC.58,60 More recent data has also suggested a role of TGF-β on upregulation of PD-1 in CD8+ T-cells, which could decrease the efficacy of therapeutics targeting the PD-1 or PD-L1.
Tumor Necrosis Factor-α (TNF-α)
First discovered in the 1970s, TNF-α has long been associated with many cancers including EC. 61 The pleiotropic cytokine binds to two different receptors, TNFR-1 and TNFR-2, and plays an important role in various oncogenic pathways such as NF-kB and MAPK.62,63 TNF-α can be secreted by both cancer cells, including EC, as a method to activate fibroblasts and conversely, through CAFs as means to convert other resident fibroblasts and support cancer cell proliferation.14,64 In stark contrast with its tumor progressive functions, TNF-α has also been shown to kill cancer cells at high concentrations. 61 While promising, the increased cytokine concentration produces toxicity in patients but yields lower side effects when administered locally.61,62
Although TNF-α implores a variety of functions, more recent studies have shifted focus to the cytokine’s involvement in the mediation of cancer-related processes. TNF-α has been shown to be involved in cisplatin resistance in ESCC via induction of EMT by increased superoxide dismutase mitochondrial (SOD-2) production. 65 TNF-α also increased in vitro proliferation of human ESCC cells. 65 TNF-α signaling has been associated with EMT activation in other cancer types by similar mechanisms, as well.66,67 TNF-α also plays a complex role in the progression of BE to EAC through multiple mechanisms.68,69 Previous studies suggest that the loss of glutathione peroxidase 7 (GPX7) is attributed to an upregulation of TNF-α, thus producing NF-kB induced tumorigenesis. 68 More recently, TNF-α has been implicated in promoting the expression of other CAF secretions such as IL-8 that impact the progression of BE to EAC. 69
Interleukin-6
First discovered in 1986, IL-6 is another pleiotropic cytokine that plays an important role in several processes from metabolism to tissue and cell maintenance.70-72 The 25 kD cytokine has since become the focal point of extensive efforts to halt the progression of numerous cancers, including esophageal.70,73 IL-6 is able to have such vast impacts on various cancer types via its role in numerous oncogenic pathways including STAT3, NF-kB, PI3K, and MAPK.71,74 In addition, IL-6 is also enlisted in creating a tumor niche that employs an abundant number of hallmarks necessary for EC and other cancers, specifically angiogenesis and metastasis.73,75,76
While noted throughout most cancer types, IL-6 is extremely prevalent in EC, evoking an impactful role in tumor progression. 77 In vivo experiments elucidated the importance of IL-6 on carcinogenesis via injection of co-culture of CAFs and EC cells in mice, demonstrating its ability to provide a unique, intercellular feedback system between a variety of components in the TME. 78 This communication between stromal components and cancer cells allows for alterations to the immune landscape of the TME. Through increased secretion by CAFs, IL-6 promoted decreased CD8+ and increased FoxP3+ tumor infiltrating lymphocyte levels within intratumoral tissue which have been implicated clinically in immune system suppression and reduction in overall patient survival. 79 In EC, IL-6 has been further implicated in immune suppression for its role in impairing NK cells functionality. 80 The cytokine is able to render the NK cells ineffective in EC by promoting the expression of CD39, as demonstrated via blocking of the effect by the receptor antagonist tocilizumab. 80
While IL-6 has also been cited in numerous forms of cancer progression, the protein plays a major role in resistance to various treatments. IL-6 has been directly linked to decreased efficacy of cisplatin for treating ESCC patients.81,82 These findings were verified by utilizing siRNA targeting IL-6 to display the restored sensitivity to cisplatin. 81 The cytokine yields further prognostic value with respect to patients undergoing esophagectomies where IL-6 rates have been associated with poor response to radiotherapy and chemotherapeutics. 83 Furthermore, the IL-6/CXCR7 axis has been shown to activate the STAT3/NF-kB pathway in EC and induce EMT, leading to further chemoresistance and decreased patient survival. 84
Interleukin-8
Interleukin-8, also referred to as CXCL8 and neutrophil-activating factor, was the first chemokine identified in humans and is produced in a plethora of cell types from neutrophils to EC CAFs.49,85,86 Regulation of this proinflammatory cytokine is controlled via its two receptors, CXCR1 and CXCR2, which assist with cancer hallmarks like angiogenesis in EC. 87 In EC, CXCL8 expression yields activation of several different pathways such as Akt1/RelA, STAT3, and NF-kB.88-90 IL-8 also has wide-reaching effects on EC progression via interactions with other cytokines such as IL-6 and has since been noted as a possible biomarker for ESCC.91,92
Although IL-8 has been contemplated for immune targeting, the cytokine continues to pose obstacles as it resists many current treatment methods while aiding in carcinogenesis. The presence of IL-8 greatly impacts the recruitment of certain myeloid-derived suppressor cells (MDSC), which cause increased EC tumor progression. 93 A clinical study observed that recurrence-free survival rates fell in ESCC patients expressing the CXCL8/CXCR2 system. Those same patients also experienced resistance to chemotherapy and radiation. 94 Similar results were observed in a later study demonstrating that IL-8 assists EC cells in resisting radiation therapy. 95 IL-8 is able to manipulate miR-27b-5p expression to aid in the upregulation of proliferating cell nuclear antigen (PCNA), which was the main contributor to EC radio-resistance. 95
Hepatocyte Growth Factor (HGF)
Initially observed in the primary culture of rat liver cells, HGF, also known as scatter factor, was discovered in 1984.96,97 The pleiotropic cytokine is made up of two subunits (alpha and beta), weighs 84 kD and has immense implications in EC and other diseases.96,98 The role of HGF on EC development and progression is accentuated by the wide range of stromal elements that secret the cytokine, with CAFs producing large quantities.96,97 HGF is able to promote tumorigenesis in EC through binding of mesenchymal–epithelial transition (MET) receptor tyrosine kinase and subsequent activation of its pathway. 99
In addition to EC, the activation of the HGF/MET pathway has been involved in many cancer types. HGF has been shown to increase proliferation in certain ESCC cells while also recruiting VEGF to assist in promoting angiogenesis. 100 Further studies noted increased HGF levels in over half ESCC histology samples while linking the cytokine’s expression to tumor size and stage. 101 Additionally, heightened degrees of HGF in ESCC patient plasma were associated with advanced disease stage and metastasis. 102 Upregulation of the cytokine’s receptor has also been observed in esophageal adenocarcinoma as well as its precursor, Barrett’s esophagus. 103 Recent findings demonstrated another relationship between HGF and EAC with decreased patient survival rates as cytokine frequencies were elevated. 104
Other Relevant Signaling Proteins
Although CAFs are able to manipulate the microenvironment of EC via secretion or response to the aforementioned cytokines, recent studies have begun unveiling other signaling proteins involved in EC tumorigenesis. For instance, CXCL12, also known as stromal cell-derived factor-1, is a chemokine that, via upregulation of twist1, is produced and secreted at high volumes by CAFs in EC.45,105 Subsequently, CXCL12 is able to bind its receptor, CXCR4, to induce EMT and promote EC metastasis.45,105 CCL2 is another chemokine that has been implicated in tumor progression of ESCC. 106 CCL2 secretions appear to have some association with FAP expression in CAFs. Knockdowns of FAP in subpopulations of EC CAFs resulted in a reduction of CCL2 secretions. 106 IL-1 is a prevalent cytokine in esophageal carcinogenesis with secretions producing an environment conducive to treatment resistance in ESCC.45,107 In addition to its role in ESCC, increased levels of IL-1 were shown to induce a BE phenotype in mouse models. 108 Furthermore, previous studies demonstrated a significant increase of IL-1 expression in both BE and EAC 109 . CXCL10, also referred to as interferon-γ inducible protein-10 (IP10), is an anti-inflammatory chemokine where increased rates correlated to improved patient survival in ESCC; however, others observed raised levels of the chemokine associated with advanced stages of EAC.49,110 Similarly, IL-33 is another cytokine that is upregulated by CAFs and a contributor to metastasis in EC.45,111
Cancer-Associated Fibroblast Contribution to Current and Future Treatments of EC
In the past half-century, cancer research has evolved into a growing field with immense opportunity for expanding the understanding of the disease, but adequate treatment options for some cancers, including esophageal, remain elusive. In EC, chemotherapeutics, radiation, and combination approaches comprise the most common methods of treating late stages of the disease; although, toxicity to patients and susceptible adjacent normal cells create issues for treatment.112,113 Surgical interventions such as esophagectomies and other less invasive resection methods also serve as possible treatments; however, survival rates vary drastically between patient populations and disease stages. 114 A vast obstacle for current EC treatments to overcome is CAFs as they have been shown to contribute to resistance against common chemotherapeutics like cisplatin as well as combination treatments with radiation.36,82,115,116 More recent advances, such as immunotherapy and other targeted approaches, address some of the concerns surrounding CAFs and serve as new possible avenues for treatment of EC that does not respond well to current approaches. 112
Immunotherapy is a form of therapeutic intervention that directs the patient’s immune machinery to destroy specific markers involved in cancer survival. 117 One such method utilized to halt cancer is via the implementation of immune checkpoint inhibitors. 118 These inhibitors target proteins implicated in numerous signaling pathways that assist in blocking immune responses, and allow cancer to evade the immune system. 119 The inhibitors include monoclonal antibodies, which primarily target cytokines or their receptors.118,120 The treatment has shown impressive results in various cancer types, specifically solid tumors, including breast, melanoma, colorectal, and lung.119,121,122 Another approach known as targeted therapy has also shown great promise in treating cancers via small molecules. While both immune checkpoint inhibitors and targeted therapy remain fairly novel in the treatment of EC, some targets include HER2, HGF/MET, EGFR, PD-1, and PD-L1. 123
Treatments Targeting Cancer Cells that are Impacted by Interactions with CAFs
Human epidermal growth factor receptor 2, HER2, is a key target of numerous therapies available for EC treatment.123,124The first FDA approved HER2-specific treatment was the monoclonal antibody trastuzumab that demonstrated improved patient survival in combination with chemotherapy and the immune checkpoint inhibitor.123,124 Its approval has led to the development of targeted therapies focused on the tyrosine receptor kinase, including pertuzumab and zanidatamab.123,125 While the results are encouraging, subsequent studies in breast cancer have demonstrated trastuzumab resistance via CAF secretion of FGF5, although the phenomenon has yet to be observed in EC. 126 Additionally, side effects such as cardiotoxicity have been observed in various patient populations including those with EC. 124
Another receptor tyrosine kinase with profound opportunities for targeting EC is epidermal growth factor receptor (EGFR).123,125,127 Approved for the treatment of colorectal cancer, cetuximab is a chimeric monoclonal antibody that demonstrated promising results in initial trials with EC.123,125 Nimotuzumab is another anti-EGFR therapy, which has shown positive results in EC when paired with radiation.125,128 Recently, lapatinib, a small molecule inhibitor, is gaining traction in EC, which shows dual inhibition of EGFR and HER2. 123 Although promising, recent in vivo studies in lung cancer highlight concerns over therapeutic resistance of tyrosine kinase-specific therapies as cancer cells have been shown to utilize lactate to direct CAF secretion of HGF, hindering therapies such as lapatinib and other immune checkpoint inhibitors (ICIs). 129 The findings have yet to be replicated in EC, but questions persist on the responsiveness of EC to the treatments due to inconsistent results in clinical trial. 123
Targeting the interaction between MET and its ligand HGF is another avenue that researchers have explored to combat blockades against the immune system.123,130-132 Overexpression of c-MET has been demonstrated in both ESCC and EAC while HGF is a known secretion of CAFs.97,125 Current therapies targeting the pathway have shown promise in obstructing cancer signaling; however, EC patient survival rates have not been significantly impacted. 123 One MET inhibitor gaining attention is AMG337, and while still early in clinical trials, displays anti-cancer properties. 123 That said, CAF-induced therapeutic resistance poses roadblocks with prolonged treatment efficacy. 129 Although still unobserved in EC, CAFs have also been implicated in gradual resistance to MET inhibitors in lung cancer. 129 While various targeted agents have shown potential, therapeutic efficacy and adverse effects on the heart have led some researchers to seek alternative approaches. 132
A subsequent target that has drawn scientist’s attention is the PD-1/PD-L1 interaction. Programmed death 1 (PD-1) and its ligand (PD-L1) are responsible for the suppression of T-cell response, allowing for evasion of the immune system in esophageal and other cancer types.118,120 EC cells express PD-L1 on their surface while immune cells like macrophages display PD-1. 123 The interaction between ligand and receptor leads immune cells to perceive the EC cells as harmless, allowing them to escape immune destruction.123,125,133 Immune checkpoint inhibitors targeting this interaction have shown potential in clinical trials with pembrolizumab, a monoclonal antibody blocking PD-1, demonstrating promising results as improved overall survival when administered alongside chemotherapeutics.120,123,133 On the other hand, recent studies have shown certain subtypes of CAFs impact the effectiveness of pembrolizumab in melanoma treatment. 134 Though yet to be observed in EC, CAF clusters were significantly elevated in patients unresponsive to pembrolizumab. 134 Conversely, other immunotherapies targeting the ligand-receptor, such as nivolumab and camrelizumab, have shown promise in treating EC.123,125
Treatments Directly Targeting CAFs
More recent research has since shifted to disrupting the TME and even utilizing stromal elements, such as CAFs, to assist in killing cancer. 135 Various methodologies have been hypothesized for directly targeting CAFs in other cancers, which remains a challenge given their heterogeneity and lack of definitive markers.64,118,135 Recent clinical trials have attempted to utilize antibodies in order to target FAP-α directly in CAFs (https://clinicaltrials.gov/ct2/show/NCT02209727?cond=sibrotuzumab&draw=2&rank). 136 For instance, sibrotuzumab, an anti-FAP-α antibody, was discontinued after failing to produce favorable outcomes. 136 In fact, the antibody actually decreased patient survival; however, subsequent immunotherapies that target FAP-α, such as RO6874281, have been proposed in combination with existing therapeutics in hopes of improving treatment efficacy in EC (https://clinicaltrials.gov/ct2/show/NCT03386721). 136 Alternatively, as single-cell analyses become more widely available, numerous studies have begun seeking subpopulation-specific therapies in other cancer types.64,137 One such study targeted CAFs in breast cancer by utilizing pirfenidone and observed favorable results in declining CAF viability; however, the anti-fibrotic drug alone did not impact metastasis as initially hoped. 138 Another approach has been to interfere with CAFs ability to perform autophagy. 139 Disrupting the function was shown to decrease levels of proinflammatory cytokines, increase responsiveness to chemoradiation, and decrease cell proliferation. 139 Other techniques to obstruct CAFs that have been investigated seek to revert the cell type back to its quiescent phase.13,137 This reversion has been observed experimentally through the usage of distinct agents like all-trans retinoic acid (ATRA), vitamin D, and vitamin A.135,137 While these cutting-edge studies continue trying to reprogram and repurpose CAFs in other cancers, work remains in order to elucidate whether these findings can produce similar results EC.
Conclusion
The rise of esophageal cancer worldwide continues to raise concerns with incidents of EAC rising extensively throughout the western world while ESCC remains the predominant type within Asia. Although various treatment methods have begun to address EC, numerous factors have created hurdles for effective therapeutics. The immune-deficient environment, influenced greatly by CAFs, has created difficulties in targeting cancer cells. Additionally, the similarity of markers to normal fibroblasts and heterogeneity of CAFs generate issues in attacking them. However, more novel approaches such as single-cell analysis and fibroblast reversion techniques have created optimism that CAF-targeted treatments are on the horizon for EC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Indiana University School of Medicine and Goshen Center for Cancer Care.
An ethics statement
All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.