
Abstract
Background
Asian American women face disproportionate burden of cervical cancer (CC) than non-Hispanic white women in the U.S. The goal of this study was to assess the feasibility and impact of a culturally tailored intervention to promote Human papillomavirus (HPV) self-sampling test among hard-to-reach Asian American women.
Methods
We adopted the community-based participatory research (CBPR) approach to conduct this efficacy study. A total of 156 female participants (56 Chinese, 50 Korean, and 50 Vietnamese) were recruited from community-based organizations (CBOs) in the greater Philadelphia metropolitan area. The intervention components included HPV-related education, HPV self-sampling test kit and instructions, group discussions, and patient navigations, all available in Asian languages. We examined several outcomes, including the completion of HPV self-sampling, HPV-related knowledge, perceived social support, self-efficacy, and comfort with the self-sampling test at post-intervention assessment.
Results
The majority of Asian American women had low annual household income (62.3% earned less than $20,000) and low educational attainment (61.3% without a college degree). We found significant increase in participants’ knowledge on HPV (baseline: 2.83, post: 4.89, P <.001), social support (baseline: 3.91, post: 4.09, P < .001), self-efficacy (baseline: 3.05, post: 3.59, P < .001), and comfortable with HPV self-sample test (baseline: 3.62, post: 4.06, P < .001).
Conclusion
To the best of our knowledge, this is the first intervention study that promoted HPV self-sampling test among Asian American women. Our findings showed that CBPR culturally tailored intervention of self-sampling was highly effective in empowering low-income Asian American women to conduct HPV self-sampling tests.
Keywords
Introduction
Human papillomavirus (HPV) is the most common form of sexually transmitted infection in the United States. 1 The Centers for Disease Control and Prevention (CDC) estimated that 79 million individuals in this country have been infected with HPV, and each year 14 million new cases occur. 2 HPV is associated with numerous health complications, including genital warts and various forms of cancer affecting the cervix, vulva, vagina, penis, anus, and oropharyngeal cavity. 2 There are more than 40 strains of HPV, which have varying impacts on human health. High risk HPV (hrHPV) strains, particularly HPV16 and HPV18, are highly related to cancer development. 2
Cervical cancer (CC) is the most common form of HPV-related cancer. The National Cancer Institute (NCI) estimated that there were 13,170 new diagnoses of CC and 4250 CC-related deaths in 2019 alone. 3 Public health professionals and health providers see a real opportunity in eradicating CC through high coverage of CC screening and HPV vaccination.4-6 Screening for CC can be accomplished through a Pap smear or through HPV testing. 7 In 2018, the US Preventive Task Force (USPTF) established guidelines for CC screening for women ages 21 to 65, recommending a Pap smear every 3 years for women ages 21 to 29 and a Pap smear every 3 years or a Pap smear and HPV co-test every 5 years for women ages 30 to 65. 8
Recent immigrants and low-income Asian Americans are at significant risk of health disparities when it comes to CC/HPV screening and prevention.9-11 These populations face multi-level barriers, including financial difficulties, lack of health insurance, lack of access to culturally and linguistically competent health providers, and discrimination, as well as stigma.12,13 Previous research has uncovered suboptimal CC screening rates in Chinese (72.05%), Korean (64.29%), and Vietnamese (66.67%) immigrant communities in the United States. 14 These rates are well behind the 93% target goal set by the Healthy People 2020 Plan. 15
Literature has suggested that cultural barriers must be considered in public health efforts to promote CC screening. Misconceptions about Pap smears remain common in Asian Americans, especially among recent immigrants and those who are underprivileged and medically underserved. Some of these misconceptions arise as a result of low knowledge about CC and psychosocial factors, which include fear about the screening process.16,17 In addition, some Asian Americans believe that they do not need to be screened for CC, owing to their sexual activity behaviors or because they self-identify as healthy. 18
HPV self-sampling test for hrHPV types (hereafter referred to as self-sampling test) is an accurate and feasible alternative to the clinician-led exam, especially among underprivileged or medically underserved women who are less likely to receive traditional HPV/CC screening.19,20 A review of clinical accuracy and feasibility found that the hrHPV testing on self-samples was “at least as, if not more, sensitive for cervical intraepithelial neoplasia grade 2 or worse (CIN2+) as cytology or hrHPV detection on clinician-obtained cervical samples, though often less specific” 20 (p. 2223) and that it has the potential to improve HPV/CC screening among women who lacked access to conventional screening in clinical settings. The self-sampling test allows women to take their sample using a brush, lavage, or other collection device, and it can be done by women in the comfort of their home or other private setting; thus, avoiding the feelings of embarrassment or even shame that people experience at doctors’ offices. 21 In addition, the self-sampling approach allows women to conduct the testing at any point in time, which removes time constraints and relieves financial burden, two factors that are significant barriers to screening.22,23 A few studies have found self-sampling rates to be more than two times higher than those from clinical settings. 21 However, there has been very limited research on the acceptance of the HPV self-sampling test by Asian American women. Compared to Western women, Asian American women, especially foreign-born Asian immigrants, may be less experienced with tampons or vaginal medications and might feel less comfortable or confident with inserting a foreign object into the vagina.24-27
So far, only a small number of studies have examined factors related to HPV self-sampling. Greater HPV-related knowledge, 28 younger age, 29 and higher educational attainment 29 appear to be significantly associated with HPV self-sampling test uptake. Studies on preventive HPV vaccination and Pap tests found that greater levels of self-efficacy and comfort are associated with greater use of HPV vaccines and Pap tests. In addition, studies have found that social support from friends and family serves as a significant facilitator for routine Pap testing, which is in line with the broader body of literature on psychosocial predictors of preventive behaviors, as indicated by the Health Belief Model (HBM). 30 However, there have been very few studies on HPV self-sampling tests in Asian Americans communities.
Guided by the HBM land the Community-Based Participatory Research (CBPR) approach, we designed and implemented an educational intervention to promote HPV self-sampling tests in low-income Asian American communities. The goal of this study is to evaluate our culturally tailored intervention on HPV self-sampling test uptake. Our findings contribute to the growing body of literature on cancer prevention in medically underserved communities.
Methods
Intervention Development
We designed a culturally tailored intervention about the HPV self-sampling test and implemented the intervention in Asian American communities in the greater Philadelphia metropolitan area and in New York City. The goal was to promote awareness and uptake of HPV self-sampling tests. We adopted the CBPR approach in the intervention component design by working closely with community leaders, stakeholders, health providers, and community member representatives in the intervention design and implementation stages.
The intervention consisted of 4 components. First, to address individual-level barriers, such as lack of awareness or knowledge among community members, we conducted group education workshops at local community-based and faith-based organizations. During these educational workshops, our bilingual community health educators gave a presentation on HPV symptoms and transmission, CC risk factors, and early detection strategies and testing to participants. The participants also received individual handouts on HPV and CC prevention to take home or share with friends and family members. Specifically, we used the Health Believe Model to guide the design of the education contents, which included information on Asian American women’s susceptibility to HPV and cervical cancer (prevalence and incidence rates of HPV and cervical cancer in Asian American women, mortality rates of cervical cancer in Asian American women, means of HPV transmission, etc.,); the severity of HPV and cervical cancer, as well as delayed detection or lack of treatment for HPV (symptoms and consequences of HPV and cervical cancer); and the potential benefits of HPV screening (efficacy of HPV screening and vaccination in reducing cervical cancer and other types of cancer). We also included information on different channels for healthcare access, including screening and follow-up care to address the various barriers that Asian American women face. Another HBM construct, self-efficacy, was addressed through the next component of the intervention, detailed below. Facts and statistics related to HPV and cervical cancer were collected from websites and reports of the CDC and the NCI.
Second, the bilingual health educators provided written and illustrated instructions detailing how to perform the self-sampling test in Chinese, Korean, and Vietnamese languages. We translated the official instructions of the HPV self-sampling test kit into Chinese, Korean, and Vietnamese languages and provided additional explanations and clarifications. Each step of the test was described in detail verbally by our health educators to the participants. Each participant received one testing device, along with the illustrated instruction sheets in English and in one of the three Asian languages. Participants then performed the test in private in the bathroom. If participants requested a second testing device for some reason (eg, when they believed they did not collect the sample successfully the first time), they were provided another testing device.
Third, at the end of each educational workshop, we organized a group discussion session. Participants were encouraged to share their experience with the workshop, their opinions or attitudes toward the HPV self-sampling test and HPV/CC detection and prevention. Specifically, we provided the opportunities for the participants to reflect on what they liked or disliked about using the self-sampling kits, receiving the results, as well as follow-up care if they were to receive an abnormal result. We also facilitated discussions regarding participants’ impressions of community norms or stigma related to HPV/CC and about their perceived support from friends and families for HPV/CC testing.
The fourth component of our intervention addressed system-level barriers encountered through patient navigation of health care, including follow-up care. The bilingual community health workers (CHWs) provided assistance in several areas. The CHWs contacted each participant by phone 1 month post-intervention to follow-up on any questions the participants might have had that were related to the HPV self-sampling test and test results and provided personalized feedback. For participants who received inconclusive or abnormal results from the HPV self-sampling tests, the CHWs provided contact information of health providers for follow-up tests, helped participants make appointments, and provided transportation information.
In developing the culturally tailored intervention, we used cultural understanding from focus group and interview research conducted previously. Specifically cultural modifications in the intervention components included the use of bilingual health educators and CHWs, the incorporation of Chinese, Korean, and Vietnamese cultural beliefs and practices, low-literacy materials, and content delivery in Asian languages. In particular, we offered more explanations and contexts to the statistics and texts from the CDC and NCI to make them more accessible. We also created an open and supportive learning environment to encourage questions and discussion among the participants and with the bilingual health educators.
All intervention materials and survey questionnaires were designed in English, translated to simplified Chinese, Korean, and Vietnamese, and translated back to English for accuracy. Translation was conducted by our bilingual community educators with consultation from community stakeholders and health providers. This was to ensure that the translation of educational materials and questionnaire content was both accurate, acceptable accessible to community members, especially those with low education and limited health literacy.
The HPV self-sampling test kit contained a simple nylon brush specifically designed for self-collecting a cervico–vaginal sample, a solid media transport card to transport the specimens, and illustrated instructions. The Just For Me® nylon brush was developed by Preventive Oncology International Inc (POI) (Cleveland Heights, Ohio, USA). The Just For Me® specimen processing card was designed and assembled by GE Health (Piscataway, NJ, USA) under POI’s supervision. For sample collection, the brush was inserted into the vagina, turned 2–3 times to the left and 2–3 times to the right. It was then removed and rubbed onto the purple zone on the specimen processing card and returned with a barcode sticker in the pre-paid envelope. The health educators received the sample specimens from each participant on site, stored them inside a specimen storage box at room temperature, 31 and used standard postal/transportation services to ship the specimens within 3 days after each workshop to a laboratory for subsequent HPV testing. The laboratory was a High Complexity reference laboratory specializing in cancer diagnosis that was accredited by the College of American Pathologists (CAP) and certified through Clinical Laboratory Improvement Amendments (CLIA). Results were usually received within 4 weeks; the health educators translated the test results into Chinese, Korean, or Vietnamese before sending out the results to the participants via mail. Further patient navigation assistance was provided based on participants’ test results and needs.
Data Collection
We recruited participants through community-based organizations and faith-based organizations in 3 ethnicities: Chinese, Korean, and Vietnamese Americans. We first designed flyers in English, Chinese, Korean, and Vietnamese, in which we described the study goal, participant eligibility, and time and location for the intervention; flyers were distributed at community-based and faith-based organizations. Participants were eligible for our study if they: (1) self-identified as Chinese, Vietnamese, or Korean; (2) were biologically female and between ages 30 and 55; (3) were not currently diagnosed with cervical cancer; and (4) had not participated in CC screening within the past 3 years. Informed consent and HIPAA authorization forms were obtained from all eligible participants who were interested in our study. We conducted a baseline survey before each educational workshop and a post-intervention survey immediately following each workshop to collect information on their sociodemographic characteristics, health-related information (health insurance status, family history, etc.), and lifestyle behaviors. We also measured participants’ HPV-related knowledge, awareness of and attitude toward HPV self-sampling tests, perceived social support, and self-efficacy related to the HPV self-sampling test.
In total, 156 eligible participants were enrolled and completed the study, including 56 Chinese, 50 Vietnamese, and 50 Korean American women. All 156 participated completed the baseline and post-intervention surveys. This study was approved by the Internal Review Board (IRB) of Temple University. Written consent was acquired from all participants and CHWs.
Measurement
Outcome measures. One of the main outcomes of interest was participants’ uptake of the HPV self-sampling test 6-months post-intervention. This measure was a dichotomous variable (yes vs no). Other outcomes included changes in participants’ HPV-related knowledge, perceived social support, self-efficacy, and comfort conducting an HPV self-sampling test from baseline to post-intervention assessment. All 4 psychosocial outcome variables were assessed by survey at baseline and post-intervention. Knowledge was assessed with 6 questions that covered participants’ understanding of CC and HPV symptoms, HPV risk factors, HPV transmission, and CC prevention and early detection. We computed a knowledge score by summing participants’ answers to all 6 questions. The knowledge score ranged from 0 to 6, with a higher numeric value indicating greater HPV-related knowledge. Perceived social support was assessed with 11 questions that measured participants’ perceptions of support from spouses, other family members, friends, and physicians with respect to decision making and screening. Participants were asked to rate their attitude toward statements such as “my family will support me if I decide to screen for cervical cancer” or “my sexual partner supports me to have cervical cancer screening.” Their responses were rated on a 5-point Likert scale, from 1 “strongly disagree” to 5 “strongly agree.” We computed the perceived social support score by taking the average of participants’ answers to all 11 questions. The knowledge score ranged from 1 to 5, with a higher numeric value indicating greater HPV-related knowledge. We measured self-efficacy by asking participants about their attitude toward the statement “I am confident that I can conduct the self-sampled HPV test by myself.” Participants were asked to respond on a 5-point Likert scale from 1 “strongly disagree” to 5 “strongly agree.” We assessed participants’ perceived comfort of the HPV self-sampling test with the question “how comfortable would you feel collecting your own vaginal sample at home for an HPV test if your health care provider showed you how?” Participants were asked to respond on a 5-point Likert scale, from 1 “very uncomfortable” to 5 “very comfortable.” The comfort score ranged from 1 to 5, with a higher numeric value indicating greater comfort toward the HPV self-sampling test.
Sociodemographic, health-related, and lifestyle factors. At baseline survey, we collected information on participants’ demographics (age, marital status, education, employment status, and income), information on participants’ health resources and preferences (health insurance, usual source of care, and physician gender preferences when conducting a vaginal exam or cervical cancer screening), and information on participants’ smoking status.
Statistical Analysis
We conducted univariate analysis to describe the sociodemographic characteristics of the study sample. For the HPV self-sampling test uptake, we assessed the test rate 6-months post-intervention. We intended to use binary logistic regression to examine the baseline and post-intervention factors that were significantly associated with HPV self-sampling test uptake. For the psychosocial outcomes, we used paired sample t-test to examine the changes in knowledge, perceived social support, self-efficacy, and comfort conducting an HPV self-sample test from baseline to post-intervention. All statistical analyses were conducted in SPSS 25. 32 A two-tailed P-value lower than .05 indicates statistical significance.
Results
Descriptive Statistics of Sociodemographic Characteristics of Study Participants (N = 156).
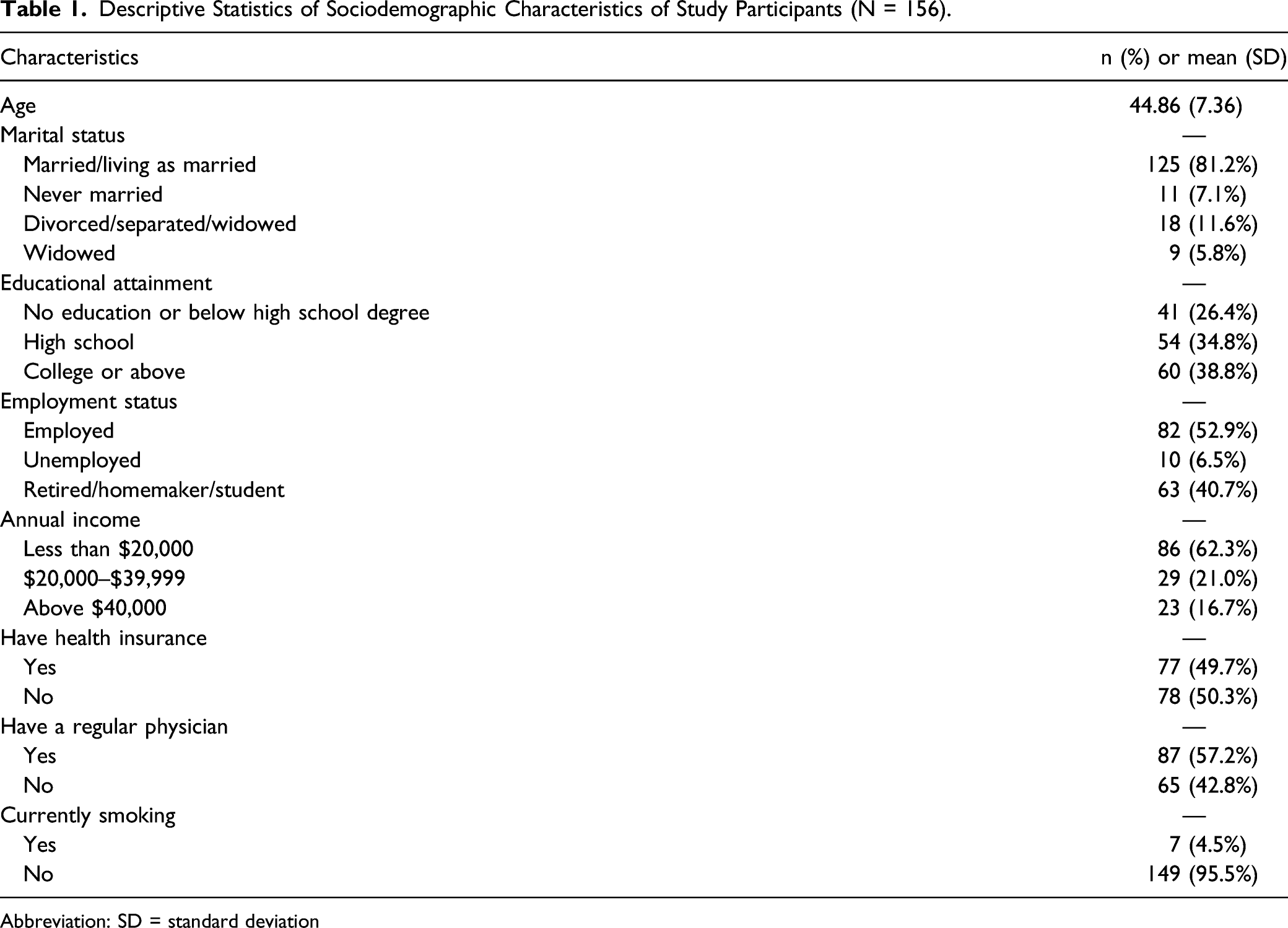
Abbreviation: SD = standard deviation
We examined the HPV self-sampling test update and found that all 156 (100%) participants completed the self-sampling test. The sample specimen from 2 out of the 56 (3.57%) Chinese participants and 9 out of the 50 (18%) Vietnamese participants did not contain any fluid, preventing testing for HPV DNA. Thus, in total, 92.95% of the participants provided satisfactory samples for testing.
Paired Sample T-Test Results of Changes in Psychosocial Outcome from Baseline to Post-Intervention Assessment.

Abbreviation: SD = standard deviation
Discussion
We designed and implemented a community-based, multicomponent intervention to promote HPV self-sampling test among 156 women from Chinese, Korean, and Vietnamese American communities. The intervention components included community-based education, group discussion sessions, device and instructions for self-sampling test, and patient navigation. All (100%) participants performed the self-sampling test and returned test kits after the intervention sessions. This finding adds to the increasing body of literature on HPV self-sampling being a feasible way to promote screening in women with low access to conventional screening tests in clinical settings.20,33 Future studies should explore the feasibility and efficacy of interventions promoting HPV self-sampling in medically underserved populations, including other Asian American and Pacific Island ethnic groups, African and Hispanic American women, as well as sexual and gender minority groups.
In addition, participants had increased knowledge, perceived social support, self-efficacy, and comfort at post-intervention assessment. We found that the intervention effectively improved screening rates over time in our sample as assessed by the immaculate self-sample completion rate. Participants’ average HPV-related knowledge was very low at baseline, but it improved drastically following the intervention, lending support to existing literature on the efficacy of culturally tailored interventions in improving knowledge related to HPV or CC in Asian American communities.34,35 Research has shown that greater knowledge is significantly associated with stronger intention or greater uptake of HPV/CC screening.36-39 More culturally sensitive and tailored education intervention efforts are needed to improve HPV/CC related knowledge and promote HPV/CC screening in underserved Asian American communities. Our findings also add to the existing body of literature on the effectiveness of the Health Belief Model in guiding health promotion interventions in medically underserved populations.40-42 The HBM constructs such as self-efficacy and were significantly predictors to the uptake of healthy behaviors; intervention components need to effectively address these factors with cultural competency to be effective.
We also found that participants perceived stronger social support after the intervention measure. This is likely due to the group discussion. During group discussions, participants exchanged opinions on social or cultural barriers that women faced regarding reproductive health prevention and on how to get more support from their friends and family. The open discussions likely helped participants feel more supported or more confident to seek support from friends and family. Future studies could design and implement interpersonal-level interventions components among family members and peers to directly facilitate social support to HPV self-sampling uptake among other preventive health behaviors.
The majority of participants reported high levels of confidence in their ability to complete the HPV self-sample test. In addition, more than half of participants reported high levels of comfort in completing the test on their own. Such high confidence and acceptance further confirm that Asian American women have high acceptance of HPV self-sampling if provided with culturally sensitive and tailored educational information on HPV, CC, and the self-sampling test. Previous studies have found that when women are unsure whether they conducted self-sampling correctly, they were less confident about the results than the results of tests conducted by a physician.26,40-42
This study is not without limitations. We did not include a control group in this study, hence our inability to demonstrate that the positive changes in outcomes were entirely due to the effects of the intervention components. The 100% self-sampling test uptake among participants made it impossible for us to examine any predictors. In addition, we did not evaluate the efficacy of each intervention component separately. Furthermore, we did not examine any potential differences across the three detailed Asian American ethnic groups because of the limited subgroup sample size. Last but not the least, the 100% rate of test completion limited our ability to explore reasons why women might opt out of the test. To fully assess whether self-sampling could be implemented on a large scale in Asian American or other under-screened communities, further studies are needed. Nonetheless, this study provides valuable pilot data on the feasibility of implementing an HPV self-sampling test for cervical cancer screening in underserved Asian American communities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the faculty research funds under the Center for Asian Health, Temple University (PI: Grace X. Ma, PhD). It is also partially supported by TUFCCC/HC Regional Comprehensive Cancer Health Disparity Partnership, Award Number U54 CA221704(5) from the National Cancer Institute of National Institutes of Health (NCI/NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NCI/NIH.
Ethical Approval
This described study was approved by the Institutional Review Board (IRB) of Temple University (IRB PT: 6940).
Statement of Human and Animal Rights
All study procedures involving participants were consistent with the requirements of the Institutional Review Board (IRB) of Temple University and approved by the Institutional Review Board (IRB) of Temple University (IRB PT: 6940). Written consent was acquired from all participants and CHWs.
Statement of Informed Consent
All participants read and signed the informed consent forms to participate in the study.