
Abstract
Colorectal cancer is the third most common cancer and the second leading cause of death from cancer worldwide. In Vietnam, the disease is the fifth leading cancer (8.9%), with 14 733 new cases in 2018. In recent years, the mFolfox6 regimen has been indicated commonly as the adjuvant chemotherapy after curative resection for patients with colorectal cancer. However, the efficacy of the regimen in Vietnamese patients has not been assessed and reported. In this retrospective study, we reviewed medical records of 83 patients with stage II or stage III colorectal cancer who received mFOLFOX6 regimen in order to investigate simultaneously survival and safety of this chemotherapy regimen. Three-year overall and disease-free survival were 84.3% and 79.5%, respectively. Our data revealed that postoperative Carcinoma Embryonic Antigen (CEA) level was a significant prognostic factor for survival, with hazard ratio of 3.83 and 3.67, respectively (P < .05), for overall survival and disease-free survival in the elevated CEA level group when compared to the normal CEA level group. The regimen also demonstrated to be well tolerated and can be used in routine practice as an adjuvant chemotherapy.
Introduction
Colorectal cancer is the third most common cancer and the second leading cause of death among all types of cancer worldwide. In Vietnam, the disease is the fifth leading cancer (8.9%), with 14 733 new cases in 2018. 1
Surgical treatment is the main method to remove primary tumors and regional lymph nodes in colorectal cancer. While surgery is a regional treatment that prevents the spread of the cancer, chemotherapy is still necessary for the prevention of metastasis and recurrence, leading to improved disease-free survival (DFS) and overall survival (OS). 2 -4
The MOSAIC trial demonstrated the role of oxaliplatin in adjuvant chemotherapy for colorectal cancer and recommended the FOLFOX regimen consisting of fluorouracil (5FU), leucovorin, and oxaliplatin as standard therapy in clinical practice. 3,5 To reduce the duration of hospitalization and treatment cost, the FOLFOX4 regimen was modified to mFOLFOX6, which has been indicated more commonly as standard adjuvant chemotherapy for stage II and stage III colorectal cancer. 2 In Vietnam, this regimen was applied in recent years, but its efficacy and toxicity profile among Vietnamese patients have not been reported.
Therefore, we conducted this observational retrospective study to determine the efficacy and safety of mFOLFOX6 on survival of Vietnamese patients with stage II and stage III colorectal cancer and its major adverse events.
Methods
Study Design
This was an observational retrospective study.
Participants
Medical records of patients with colorectal cancer who were treated with mFOLFOX6 regimen as adjuvant therapy from December 2013 to December 2015 were reviewed and selected if they met the following eligibility criteria: aged 18 to 75 years old, Eastern Cooperative Oncology Group 0-2, patients with stage II or stage III (according to American Joint Committee on Cancer 7th edition) colorectal adenocarcinoma who have received curative surgery, and patients with 8 to 12 cycles of mFOLFOX6 as adjuvant therapy. Other inclusion criteria included serum creatinine ≤1.5 × Upper Limit of Normal (ULN), total bilirubin ≤1.5 × ULN, Serum Glutamic Oxaloacetic Transaminase (SGOT) and Serum Glutamic Pyruvic Transaminase (SGPT) ≤1.5 × ULN, neutrophil ≥1.5 g/L, platelet ≥100 g/L, and hemoglobin >100 g/L.
Sample Size and Sampling
Based on the results of Alberts et al 6 about the effect of mFOLFOX6 on survival among patients with resected stage III colon cancer, the 3-year OS rate and the width of confidence interval (CI) were assumed to be 0.86 and 0.15. Since α was set at 5%, the sample size required was 83 patients.
Treatment
After having received curative surgery for colorectal cancer, patients were indicated 8 to 12 cycles of mFOLFOX6 regimen (consisting of 2-hour infusion of oxaliplatin [85 mg/m 2 ], 2-hour infusion of leucovorin [400 mg/m 2 ], and fluorouracil bolus [400 mg/m 2 ] on day 1, then 46-hour intravenous fluorouracil [2400 mg/m2] from day 1 to day 2).
Measurements
Patients’ laboratory tests and clinical symptoms were also collected to assess neurotoxicity, gastrointestinal toxicity, blood toxicity, hepatotoxicity, nephrotoxicity, and other toxicities of the regimen. The adverse events were recorded after each cycle and were graded according to the US National Cancer Institute, Common Terminology Criteria for Adverse Events version 5.0.
The survival and disease status of patients were collected 3 years after treatment initiation by telephoning patients or their relatives and reviewing their medical records. Any abnormalities in computed tomography scan, X ray, and laparoscopy results taking place beyond regimen completion were also collected to assess disease recurrence. When receiving this chemotherapy regimen, response was assessed normally after 3 to 6 cycles and was documented in the medical record.
Statistical Analysis and Statistical Methods
The primary outcome of the study was OS. The OS rate at 3 years and median OS were calculated based on the definition of OS by the National Cancer Institute: the duration from the date of diagnosis to death from any cause. The secondary outcomes consist of DFS (length of time from the cessation of primary treatment to relapse or death from any cause), toxicity profile of the regimen, and factors affecting patients’ survival. In our study, factors that were examined included serum Carcinoma Embryonic Antigen (CEA) level before adjuvant chemotherapy, age, sex, stages of disease, and location of tumors. Log-rank test was performed to identify the effect of these variables on survival using R 3.5.1. P < .05 was considered statistically significant.
Results
General Characteristics of the Study Sample
Patient characteristics are presented in Table 1. Eighty-three patients who received mFOLFOX6 regimen between December 2013 and December 2015 were included. The mean age was 54.8 years old, and 57.8% patients were male. Among those who had CEA test after surgery, the large majority had their CEA level lower than 5 ng/mL (50.6% vs 12.0%; patients had CEA level >5 ng/mL). Malignant tumors in rectum were found in four-tenths of the study population, while tumors in ascending and sigmoid colon accounted for 24.1% and 16.9% of patients, respectively. In all, 62.6% patients were indicated CEA tests after curative surgery; those who have normal test results (≤5 ng/mL) made up a majority (50.6% study population).
Baseline Characteristics of Patients.
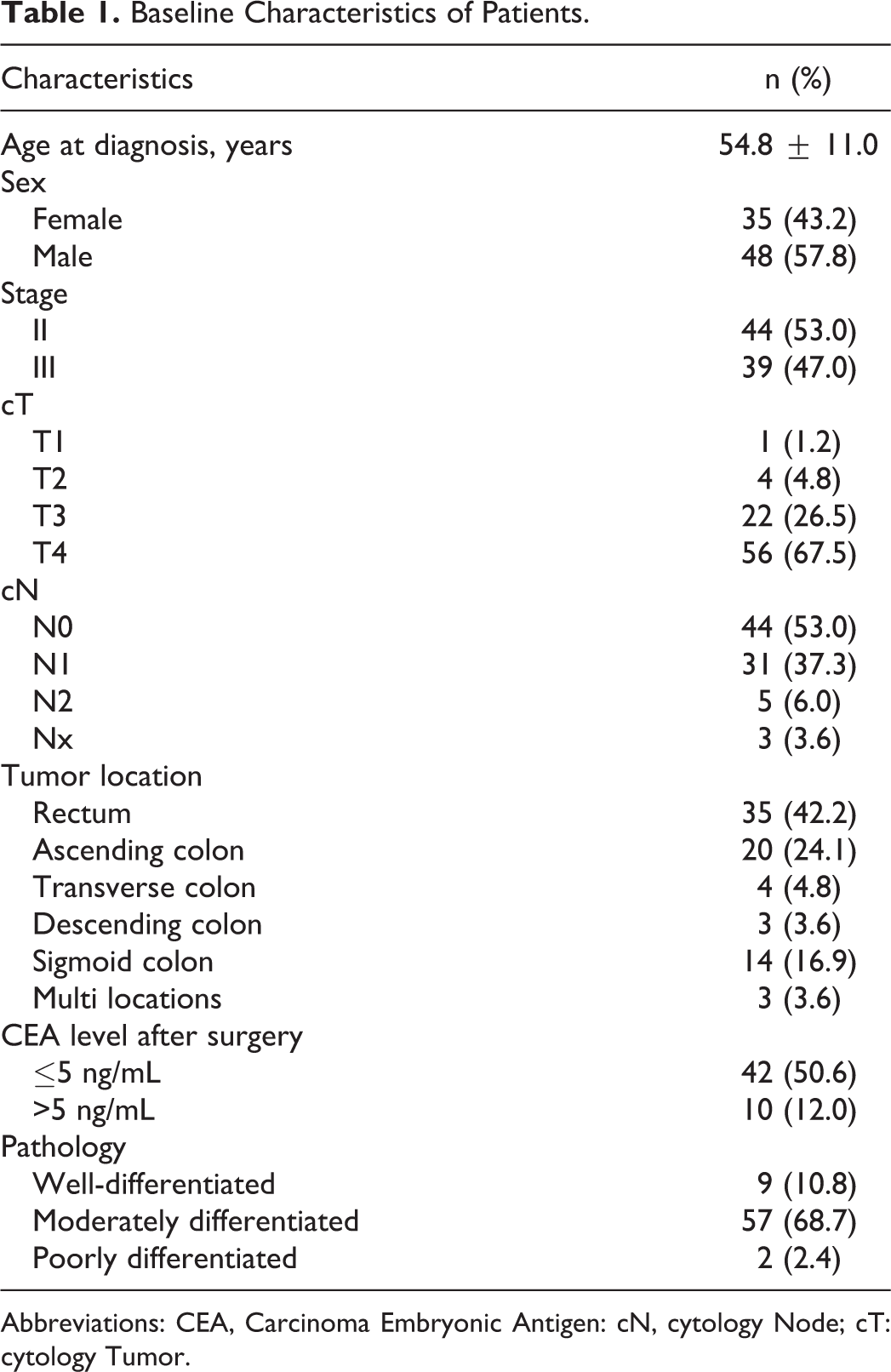
Abbreviations: CEA, Carcinoma Embryonic Antigen: cN, cytology Node; cT: cytology Tumor.
Treatment Characteristics
The majority (88.0%) of patients completed their mFOLFOX6 regimen as the adjuvant chemotherapy. The main reason for incomplete treatment is disease progression (6 patients, accounting for 7.2%). Additionally, stopping the chemotherapy due to adverse events made up 3.6%.
Most of the study population received 8 to 12 cycles (92.8%), and dose reduction (which is defined as a decrease to <90% normal dose) was implemented in only 16.9%. As for response to this regimen, a hefty 77.2% of patients were assessed as objectively responded (consisting of complete response, partial response, and stable disease) (results are shown in Table 2).
Treatment Characteristics.

Main Findings
Survival
Three-year OS rate (95% CI) was 84.3% (76.5%-92.1%), while 3-year DFS rate (95% CI) was 79.5% (70.8%-88.2%) as shown in Figure 1. Among potential factors tested in univariate models, elevated CEA level after curative surgery is the significant prognostic factor for both DFS and OS of patients with colorectal cancer receiving mFOLFOX6 regimen (P < .05) as shown in Figure 2. Disease-free survival in the stage II cancer group is significantly better than that in the stage III group (log-rank test gives a P of .04), although the same is not observed for OS (P = .2) as shown in Figure 3.

Kaplan-Meier estimates of overall survival (OS) and disease-free survival (DFS).

Kaplan-Meier estimates of overall survival (OS) and disease-free survival (DFS), according to Carcinoma Embryonic Antigen (CEA) levels after curative surgery.
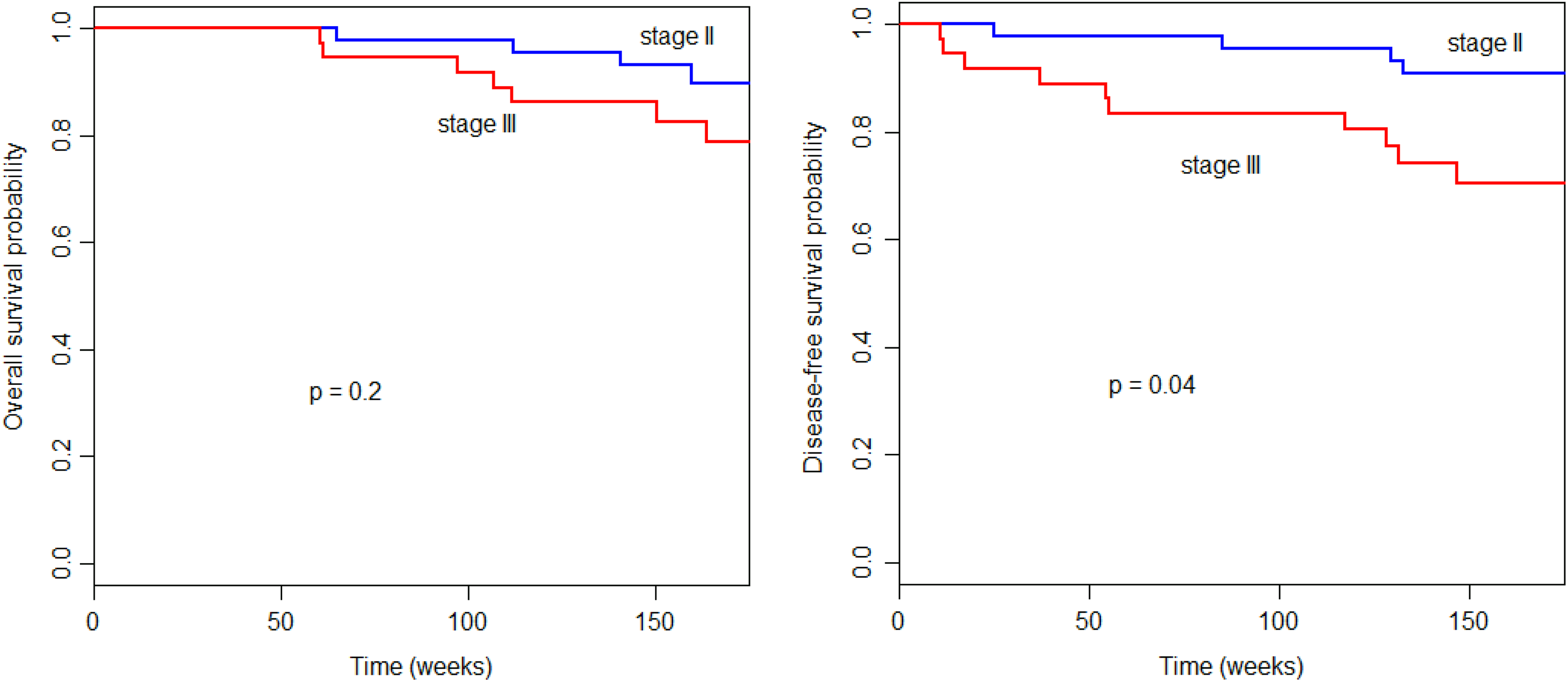
Kaplan-Meier estimates of overall survival (OS) and disease-free survival (DFS), according to stages of cancer.
Hazard ratios (HRs) and CIs are shown in Table 3. Other factors (age, sex, and locations of tumors) do not have a statistically significant influence on survival. Median DFS and median OS are not yet reached, and we are continuing to follow up enrolled patients.
Analysis Overall Survival and Disease-Free Survival According of Stage and CEA Level.

Abbreviations: CEA: Carcinoma Embryonic Antigen; CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; OS, overall survival.
Safety
The most frequent adverse event was elevated transaminases, which was assessed for more than two-thirds of the population is shown in Table 4. Other common toxicities included hematological toxicities and diarrhea. Among adverse events related to hematotoxicity, the most prevalent one was anemia (37.3%). However, all cases experienced only grade 1 to 2 anemia. Meanwhile, neutropenia occurred in fewer patients, but the severity of this event was more substantial (7.2% patients had grade 3 to 4 neutropenia). One-third of the study population had thrombocytopenia, but no one had grade 3 to 4 events. Regarding clinical adverse events, severe events were observed for stomatitis, sensory neuropathy, and diarrhea, but the prevalence was low (2.4%).
Adverse Event of the Patients.
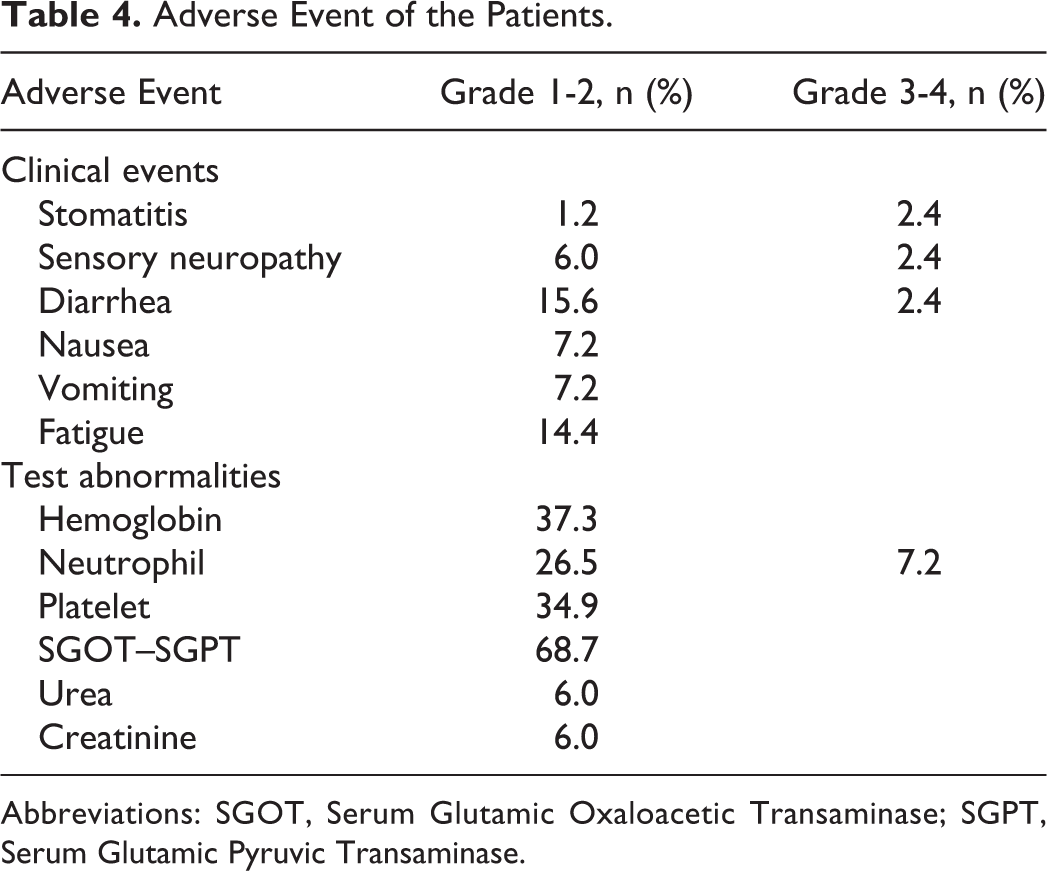
Abbreviations: SGOT, Serum Glutamic Oxaloacetic Transaminase; SGPT, Serum Glutamic Pyruvic Transaminase.
Discussion
To the best of our knowledge, the efficacy of the combination use of oxaliplatin, leucovorin, and 5-flouro uracil was well-documented, and this regimen can be indicated interchangeably with XELOX regimen for early stages, locally advanced stages, and metastatic stage, without or in combination with monoclonal antibodies. 3,7,8 Among different FOLFOX regimens, the modified FOLFOX6 (mFOLFOX6) was used commonly as adjuvant therapy after curative surgery for stage II and stage III colorectal cancer in Vietnam. Our study provides evidence of clinical outcomes and safety profiles of mFOLFOX6 regimen in Vietnamese population.
Findings of survival were consistent with results published in previous studies conducted in various populations. The 3-year OS rate and DFS rate were 84.3% and 79.5%, respectively, similar to those of a retrospective Korean study (87.5% and 82.9%), which evaluated the efficacy of FOLFOX regimen (including FOLFOX4 and mFOLFOX6) in 82 patients with stage III and high-risk stage II colon cancer. 9 Likewise, a randomized controlled trial that was conducted in North America compared mFOLFOX6 and cetuximab plus mFOLFOX6 and reported that the 3-year OS rate was approximately 87% for patients with resected stage III colon cancer using mFOLFOX6. 6 The estimated 3-year DFS reported in our study was slightly higher than reported in the C-08 trial, which investigated the effect of adding bevacizumab to the current mFOLFOX6 regimen. The 3-year DFS in the control arm (mFOLFOX6 alone) was 75.5%. 10
Compared to the efficacy reported in the literature of other regimens such as FOLFOX4 or XELOX, the regimen of our interest demonstrates its noninferiority when being indicated after curative surgery of colorectal cancer. For instance, the phase III trial investigating the efficacy of bevacizumab plus oxaliplatin-based chemotherapy as adjuvant treatment for patients with curatively resected stage III or high-risk stage II colon cancer reported that the 3-year DFS of FOLFOX4, FOLFOX4 plus bevacizumab, and XELOX plus bevacizumab was 76%, 73%, and 75%, respectively. 11
It is noteworthy that elevated CEA level after surgery was statistically associated with the reduction in OS (HR: 3.83 [95% CI: 1.03-14.3], P = .03) and DFS (HR: 3.67 [95% CI: 1.11-12.0], P = 0.02) among participants, confirming that the CEA level is a good prognostic factor for survival after treatment for colorectal cancer. This result is in accordance with that of previous studies: The identification of postoperative CEA concentration is useful for the planning of follow-up examination after treatment completion. 12,13 Additionally, log-rank test indicated that stages of cancer are, as expected, related to 3-year DFS rate (HR when comparing DFS of stage III subgroup to stage II is 2.86, P = .04); however, OS was not affected (P = 0.2). Other potential factors (age, sex, or location of tumors) were examined but no association was found.
Hepatotoxicity was the most common adverse event reported in our study, occurring in approximately two-thirds of the study population, but all of them experienced mild elevated liver enzymes (grade 1-2). This proportion is contrary to the recent publication of Kosugi et al, which showed that the proportion of elevated SGOT and SGPT is about 3%. 14
Several hematological adverse events were also observed during adjuvant chemotherapy. Decreases in hemoglobin, neutrophil, and platelet were documented in about one-third of patients, of who only 6 (7.2%) patients had grade 3 to 4 adverse events (neutropenia). Thrombocytopenia and neutropenia were most common reasons for treatment delay and administration of granulocyte colony-stimulating factor in our study. As for grade 4 neutropenia, our study reported an insignificant proportion of 1.2%, which is in agreement with that of Kosugi et al’s report (1.5%), 14 although the research of Goldberg et al revealed a larger percentage of this serious adverse event (11.1%). 15 The difference may be derived from the nature of study population.
Apart from those test abnormalities, the most common clinical adverse events were diarrhea and fatigue (18.0% and 14.4%), but only 2.4% patients had grade 3 diarrhea. Finally, other toxicities such as renal toxicity, stomatitis, and sensory neuropathy happened in a small percentage (<10%). These findings consolidate the tolerability and confirm the safe use of mFOLFOX6 regimen in routine practice as adjuvant chemotherapy in patients with colorectal cancer.
In conclusion, the present study shows the significant efficacy of the mFOLFOX6 regimen in Vietnamese patients and demonstrated that its toxicity is acceptable to be indicated routinely in the adjuvant setting.
Footnotes
Authors' Note
The protocol of this study was approved by the Scientific and Ethical Committee in Vietnam National Cancer Hospital (approval no.3722/QD-BVK). All patients provided written informed consent prior to enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.