
Abstract
Background
Nasopharyngeal carcinoma (NPC) is endemic in Hong Kong with a skewed geographical and ethnic distribution. We performed an epidemiological study of NPC in Cheung Chau Island, a fishing village with very minimal residential mobility, and compared its demographics and survival with the rest of Hong Kong.
Methods
NPC data in Cheung Chau and non–Cheung Chau residents between 2006 and 2017 treated in our tertiary center were collected. The incidence, stage distribution, and mortality of Cheung Chau NPC residents were compared with those of their counterparts in the whole Hong Kong obtained from the Hong Kong Cancer Registry. Propensity score matching (PSM) was performed between Cheung Chau and non–Cheung Chau cases in a 1:4 ratio. Overall survival (OS), progression-free survival (PFS), and cancer-specific survival (CSS) were compared between these two cohorts by product limit estimation and log-rank tests.
Results
Sixty-one patients residing in Cheung Chau were identified between 2006 and 2017. There was a significantly higher NPC incidence (P < .001) but an insignificant difference in the mortality rate in Cheung Chau compared to the whole Hong Kong data. After PSM with 237 non–Cheung Chau patients, the Cheung Chau cohort revealed a stronger NPC family history (P < .001). However, there were no significant differences in OS (P = .170), PFS (P = .053), and CSS (P = .160) between these two cohorts.
Conclusion
Our results revealed that Cheung Chau had a higher NPC incidence but similar survival outcomes compared to the whole of Hong Kong. Further prospective studies are warranted to verify this finding and to explore the possible underlying mechanisms.
Introduction
The epidemiology of nasopharyngeal carcinoma (NPC) is unique for its distinctly skewed geographical distribution. 1 It is rare in most parts of the world but it is endemic in Southeast Asia and southern China including Hong Kong. In 2018, it was the sixth commonest cancer in men and the 17th in women in Hong Kong and accounted for 2.4% of all new cancer cases. Extensive epidemiological studies of NPC in endemic areas have been carried out for the past few decades. Extensive epidemiological studies of NPC in endemic areas have been carried out for the past few decades. While NPC incidence and mortality in southern China were at high levels in the world,2,3 studies demonstrated the ethnic and geographical distribution of NPC cases in other endemic regions like India and eastern Africa and suggested an association between the host and environmental factors.4-8
The public healthcare referral system in Hong Kong is divided into seven geographical clusters, namely, Hong Kong West, Hong Kong East, Kowloon West, Kowloon Central, Kowloon East, New Territories West, and New Territories East, under the management of the Hospital Authority, the only statutory public healthcare provider serving the whole Hong Kong population of more than 7.5 million living in an area of 1107 km2. Cheung Chau Island, one of the largest outlying islands in Hong Kong, is located about 10 km southwest and connected to Hong Kong Island only by pubic ferries where the central business district, the major governmental offices and residential areas are situated (Figure 1). Cheung Chau has a comparably large population of over 22,000 people with an area of 2.46 km2, making it the most densely populated island in Hong Kong (8519 persons/km2 compared to 6788 persons/km
2
in the whole Hong Kong territory).
9
Although Cheung Chau belongs to the Hong Kong East Cluster in terms of public healthcare provision (mainly because of the availability of helicopter transport service for emergency cases), almost all residents in Cheung Chau who have cancers are referred to the Hong Kong West Cluster (HKWC) (because of geographical vicinity) in which Queen Mary Hospital (i.e., our tertiary referral center) is the only tertiary public oncology center as well as one of the two university teaching hospitals in Hong Kong for further management, if they wish to seek further management in the public sector.
10
On the other hand, there are only 6 private clinics and one public hospital (which only provides general internal medicine service) in Cheung Chau, the corresponding doctor-to-population ratio is 1:3493 which is significantly lower than that of the rest of Hong Kong (1:511), suggesting that Cheung Chau residents have a lower accessibility to healthcare services which may pose a risk of delayed cancer diagnosis and its subsequent management.
11
More importantly, Cheung Chau share some similarities with other island countries in Southeast Asia in which the majority of the indigenous inhabitants are Hakka and Hokkien Chinese fishermen and their descendants, who have the habit of preserving their catch into salted fish for later consumption. Their children also share the same dietary habits with their parents who consume salted fish at an early age. Furthermore, the residential and geographical mobility in Cheung Chau has remained stable (7.10% in 2011 and 6.99% in 2016 in Cheung Chau vs 18.61% in 2011 and 17.08% in 2016 in the rest of Hong Kong), providing a good source of epidemiological studies on genetically related diseases and cancers including NPC.12,13 (A) Geographical location of Cheung Chau in Hong Kong and (B) geographical representations of seven clusters of public healthcare services under the management of Hospital Authority based on locations. Color dots in (A) represent the locations of government hospitals (larger dots) and their satellite out-patient clinics (smaller dots) within their respective clusters. Adapted and modified from Clusters, Hospitals, & Institutions. The Hospital Authority. https://www.ha.org.hk/visitor/template101.asp?Parent_ID=10004&Content_ID=10036&.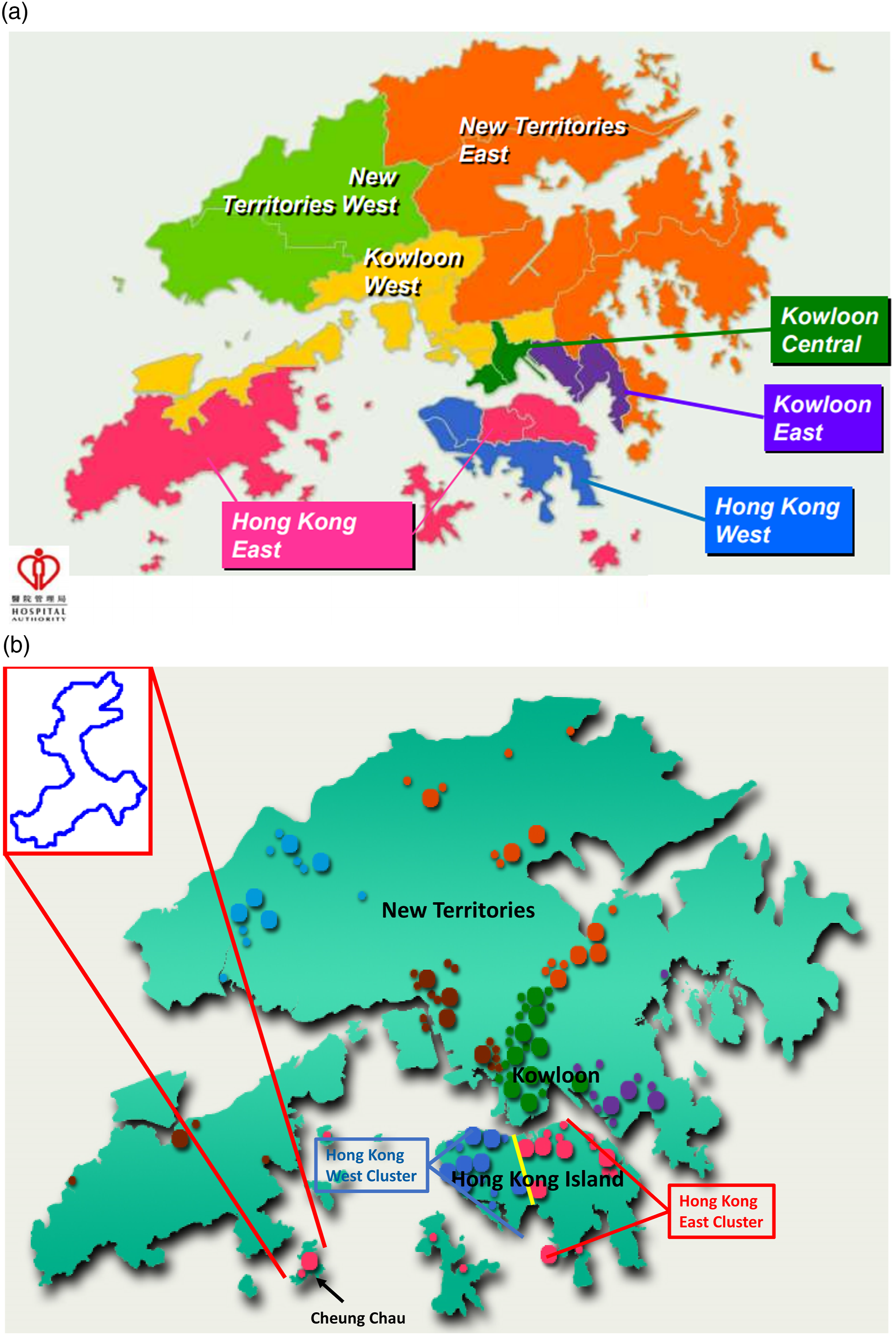
Hong Kong Cancer Registry (HKCaR) is a population-based cancer registry, which covers essential data including incidence, mortality as well as distribution of age, sex and stage of major cancer types including NPC. However, such information is just confined to the whole Hong Kong territory, and corresponding data among different administrative districts/regions within Hong Kong are not captured and provided. In view of the limited access to healthcare services, consistent dietary habits, and low residential mobility, Cheung Chau is an ideal place to study NPC epidemiology. We hypothesized that Cheung Chau has a much higher incidence of NPC compared to the whole Hong Kong territory. Therefore, we carried out this study to investigate the NPC incidence, mortality as well as its stage distribution and survival outcomes in this island which were compared to the figures in the whole Hong Kong territory, including all NPC patients treated in the era of intensity-modulated radiation therapy between 2006 and 2017. The results shall facilitate us to carry out future studies on genetic and dietary predisposing factors as well as highly focused screening and preventive measures for this prevalent malignancy within the highly endemic sub-district(s) of Hong Kong.
Methods
Patient Selection
The population data of Cheung Chau in the official census and by-census years in Hong Kong, that is, 2006, 2011, and 2016 were obtained from the Hong Kong Census and Statistics Department while those in the remaining years were estimated by interpolation based on the census data.12-14 The incidence and mortality rates of NPC in Hong Kong between 2006 and 2017 were retrieved from HKCaR, 15 while the corresponding data of NPC patients living in Cheung Chau as well as their demographics, family history of NPC (defined as having NPC in first-degree or second-degree relatives of the index patients), and NPC treatment details in the same time period were identified from Department of Clinical Oncology of Queen Mary Hospital in HKWC (i.e., our tertiary referral center) as previously mentioned. In the current study, the tumor–node–metastasis (TNM) stage of every patient’s previously untreated NPC was re-staged in accordance with the eighth edition of American Joint Committee on Cancer/Union for International Cancer Control TNM staging system for further stage distribution comparison between the Cheung Chau cohort, non–Cheung Chau cohort treated in our tertiary referral center, and all the NPC cases registered in HKCaR between 2006 and 2017. Approval from the local institutional review board for this study was obtained before study commencement (Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster, reference number UW 12-153 and UW 06-242 T/1267). It was conducted according to the guidelines of Declaration of Helsinki and Good Clinical Practice.
Statistical Analysis
The crude incidence of NPC in Cheung Chau and its mortality in our Cheung Chau cohort during this period were calculated and their differences against the whole Hong Kong territory were subsequently demonstrated in odds ratio (OR). 16 The rates were then standardized by the direct method using the world standard population as the reference. Poisson regression model was employed to estimate the average annual percentage change (AAPC) of the standardized rates so as to measure the temporal trend of NPC. The average annual percentage change with a 95% confidence interval (CI) of > 0 was considered a significantly increasing trend while AAPC with a 95% CI of < 0 was considered a significant decreasing trend.
To further compare the survivor outcomes between Cheung Chau and non–Cheung Chau patients treated in our tertiary referral center, we used propensity score matching (PSM) approach to adjust for unbalanced population and potential baseline confounders. A logistic regression model was established to calculate the propensity scores in which age, sex, T-category, N-category, and M-category were considered as predefined matching covariates. Patients living in Cheung Chau were matched with those living in regions other than Cheung Chau (the non–Cheung Chau cohort) but all treated in our tertiary referral center on a basis of nearest neighbor matching at a 1:4 ratio, in light of the huge population size difference between Cheung Chau and outside Cheung Chau.
Product-limit estimation of survival outcomes and log-rank tests were calculated for comparing survival differences between Cheung Chau and non–Cheung Chau patients before and after PSM. The survival endpoints in this study included progression-free survival, overall survival , and cancer-specific survival.
All data analyses were performed by Statistical Package for the Social Sciences version 26.0. All tests were two-sided, and P values less than .05 were considered statistically significant.
Results
Incidence and Mortality
Baseline Patient Characteristics Before and After Propensity Score Matching.

Abbreviations: IMRT: intensity-modulated radiation therapy; RT: radiation therapy.
Note: Family history of NPC in our study is defined as the presence of first-degree relatives (parents, offspring, and siblings) or second-degree relatives (aunts, uncles, grandparents, grandchildren, nieces, nephews, and half-siblings) who had NPC.
Age Standardized Incidence Rates (Per 100,000 Persons) of Nasopharyngeal Carcinoma by Year and Age Group in the Cheung Chau cohort and in Whole Hong Kong Territory.

Age Standardized Mortality Rates (Per 100,000 Persons) of Nasopharyngeal Carcinoma by Year and Age Group in the Cheung Chau Cohort and in Whole Hong Kong Territory.

Survival Outcomes After PSM
Survival Endpoints of Nasopharyngeal Carcinoma Patients Stratified by Residence and Disease Stage Before and After Propensity Score Matching.
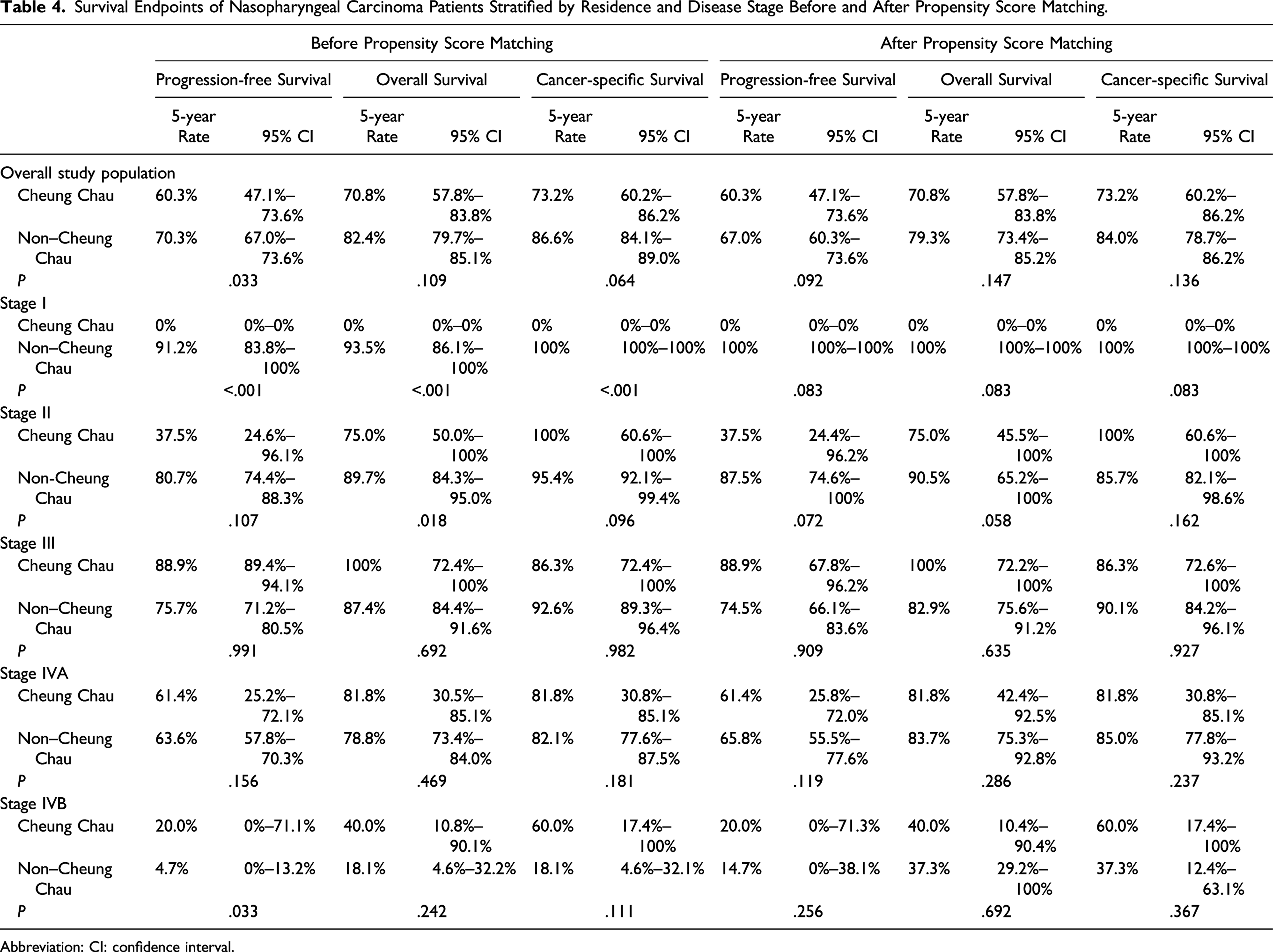
Abbreviation: CI: confidence interval.
Figure 2 and Table 4 show the survival differences between patients from the Cheung Chau cohort and the matched cohort of non–Cheung Chau patients after PSM. There was no statistical difference between the Cheung Chau and non–Cheung Chau cohorts, in either proportion of all-cause deaths (P = .97) or NPC-specific deaths (P = .88). No statistically significant difference was also found in 5-year PFS (60.3% vs 67.0%), P = .092 (Figure 2A), 5-year OS (70.8% vs 79.3%, P = .147) (Figure 2B), and 5-year CSS (73.2% vs 84.0%, P = .160) (Figure 2C) between Cheung Chau and non–Cheung Chau patients. Similarly, significant differences in survival outcomes were not observed when stratified by stages. Kaplan–Meier estimations of survival outcomes of cohorts of Cheung Chau patients and non–Cheung Chau patients with nasopharyngeal carcinoma after propensity score matching. (A) Progression-free survival, (B) overall survival, and (C) cancer-specific survival.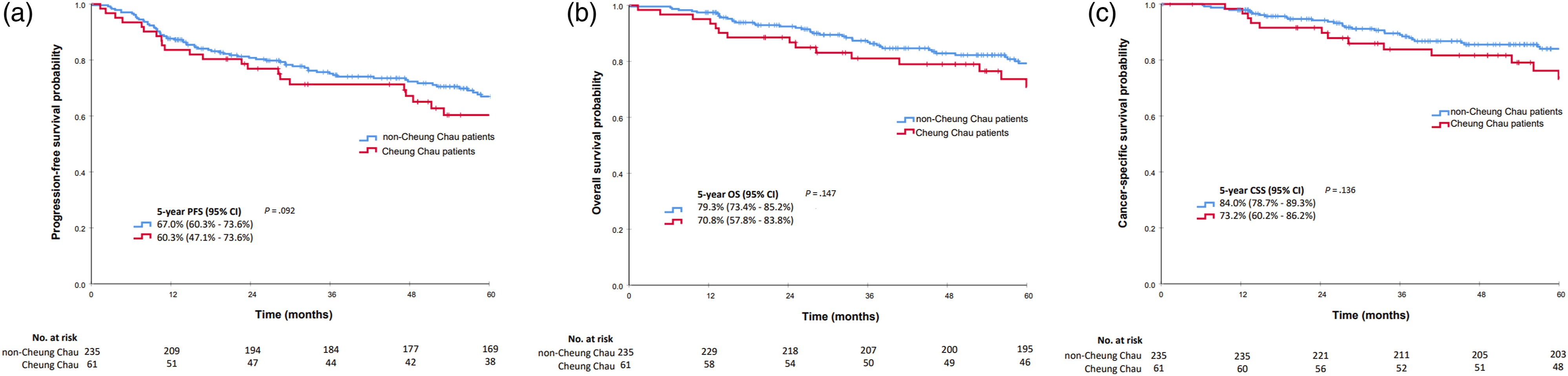
Discussion
A progressive decline in both the incidence and the mortality of NPC was observed in Hong Kong over the period of 2006–2017 based on the data from HKCaR. Such improvement was most likely attributed to dietary modification, easier accessibility to tertiary public healthcare service, advances in diagnostic and surveillance tools as well as advent of multimodality and multidisciplinary treatment.17-22 It is within our expectation that the Cheung Chau cohort showed no difference in NPC mortality rates and survival outcomes when compared to their counterparts in the whole Hong Kong population, since almost all NPC patients living in Cheung Chau received the same and prompt standard treatment based on standardized treatment protocols as for other NPC patients in all tertiary public oncology hospitals in Hong Kong under the management of the Hospital Authority, in which NPC management is one of the key performance indicators. 23 Besides, NPC management in Hong Kong has long been spearheaded by Hong Kong Nasopharyngeal Cancer Study Group which was established since 1993 and gathered all NPC experts working in all public healthcare clusters in Hong Kong who have collaborated and published numerous clinical trials on NPC for the past 3 decades.
The Cheung Chau cohort, on the other hand, is 85% more likely to develop NPC as compared to the whole Hong Kong population. Significant stronger family history of NPC in the cohort of Cheung Chau patients was observed in our study. In view of geographical characteristics and the restricted geographical mobility of its residents, Cheung Chau is an ideal place to study NPC epidemiology for four main reasons. First, due to the limited access to public and private healthcare resources, most of the Cheung Chau patients will be referred to the single institution (i.e., our hospital) for further management. This provides convenient data collection and the data collected represent the unique characteristics of NPC in Cheung Chau. Second, most of the Cheung Chau residents are indigenous southern Chinese population or Hakka and Hokkien descendants, who have a higher risk of developing NPC compared to other Asian ethnic groups.7,24 The higher NPC incidence can provide more effective population size due to higher occupation rate. Third, salted fish is one of the major food consumed by Cheung Chau residents as they share similar dietary habits of their ancestors who were mostly fishermen. The correlation between Chinese-style salted fish consumption and NPC development has been proven and confirmed.25-28 Finally, stable and restricted geographical mobility in Cheung Chau with such a small living area reduces the chance of case loss or case mix through emigration and immigration, respectively. This strongly enables us to study the familial penetrance and inheritance patterns of NPC in greater details.
The high NPC incidence in our Cheung Chau cohort could be explained by genetic predisposition, dietary habits, and lifestyle as well as the interactions among. First, family history is associated with higher risk of NPC as demonstrated. Substantial evidence showed that there is a heritable component in the risk of NPC.29-32 Second, studies have also suggested that childhood consumption of salted fish and other preserved food is one of the major risk factors of NPC among Chinese population.25-28,33-36 Risk of NPC was found to be increased with an earlier age of first exposure, frequency, and duration of consumption of these food items. Cheung Chau has traditionally been an island of fisher folk whose diet contains a high proportion of salted fish and others like preserved vegetables and shrimp paste. These are also common food consumed by inhabitants in Southern China, emigrant Chinese populations in Malaysia, and other Southeast Asian populations.27,33 All of these population groups have intermediate-to-high susceptibility to NPC development as demonstrated in previous studies.2,12,27,33 We believe that this traditional southern Chinese dietary factor still plays an important role in developing NPC in Cheung Chau at present in spite of decreasing proportion of fishery workers and the adoption of more westernized diet nowadays. A study in China further demonstrated that there is a possible interaction between family history of NPC and consumption of salt-preserved fish in the development of NPC. 37 In addition, incense burning, a traditional daily practice in Chinese households, is associated with an increased NPC risk. Cheung Chau is a well-known place with lots of Chinese temples organizing large-scale annual Chinese folk religious activities which involve frequent incense burning.38,39 Prolonged inhalation of carcinogens from incense burning was shown to significantly increase the risk of having NPC.39,40
We acknowledge several limitations in our study. First, we could not provide a clear and representative record of the amount of salted fish consumption and exposure to incense burning of our Cheung Chau patients owing to the retrospective nature of this study. Further to a recently published study in Hong Kong suggesting the role of preserved food in NPC risk, 41 additional studies such as investigations on the lifestyle of patients from Cheung Chau and the subsequent gene-environment interaction of NPC in Cheung Chau are definitely warranted to verify our results. Furthermore, there was a possibility of not collecting Cheung Chau NPC cases managed at other public or private hospitals. Consequently, we believe that we have captured almost all Cheung Chau patients diagnosed with NPC in Hong Kong within the study period since our institution is the only public oncology hospital and tertiary referral center in closest proximity to Cheung Chau, which welcomes and provides comprehensive cancer service to all Cheung Chau patients. However, any extra Cheung Chau NPC cases treated outside our institution would imply even a higher incidence than that presented in the current study. Closer collaboration with other hospitals and private practice would certainly enhance the robustness of our data. Inclusion of other fragmented outlying islands with similar characteristics in the future research would also provide much epidemiological information and reinforce our hypothesis.
Conclusion
Cheung Chau, a geographically and ethnically distinct place, shows a higher-than-average NPC incidence and a stronger family history of NPC than the rest of Hong Kong. It provides epidemiological information for future research in NPC carcinogenesis, screening, and prevention.
Footnotes
Acknowledgments
The authors would like to thank all the staff members of Department of Clinical Oncology of Queen Mary Hospital, Hong Kong for their contributions.
Author’s Note
This study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (reference number UW 12-153 and UW 06-242 T/1267). Informed consent was obtained from all subjects or, if subjects are under 16, from a parent and/or legal guardian. Access to the raw data from Hong Kong Census and Statistics Department does not require any prior administrative permissions. All methods were performed in accordance with Declaration of Helsinki and Good Clinical Practice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The datasets presented in this article are not readily available due to national legislation and the terms of the study’s ethics approval which do not allow dataset sharing outside of the institutions participating in the analysis. The corresponding author should be contacted for reasonable request to data of this study.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.